2118
Comparison analysis of IVIM and 4D flow-MRI in patients with liver cirrhosis1The First Affiliated Hospital of Dalian Medical University, Dalian, China, 2Philips Healthcare, Dalian, China
Synopsis
The occurrence and development of liver cirrhosis is accompanied by changes in portal vein blood flow and intrahepatic blood flow, which may eventually lead to liver implantation [1]. Liver-lobe-based IVIM-derived parameters can be associated with cirrhosis [2]. 4D flow-MRI could scope the portal vein blood flow [3]. In this study, we explored the correlation between the perfusion paraments and quantitative values of blood flow in patients with liver cirrhosis using IVIM and 4D flow-MRI, investigating the potential connections between portal vein flow changes and liver cirrhosis.
Introduction
DWI is the non-invasive technique to detect the diffusion movement of water molecules in living tissues. IVIM can distinguish the diffusion signal of Brownian motion of water molecules in tissues from the perfusion signal formed by capillary microcirculation, and is helpful to better describe the complex signal attenuation modes in biological tissues and organs [4]. 4D flow MRI with motion encoding and volumetric and isotropic acquisition achieves quantification of blood flow directions, velocities, wall shear force and pressures in the relatively large vessels, such as portal vein [5]. The purpose of this study is to assess the possible correlation the perfusion paraments and quantitative values of blood flow using liver IVIM and portal vein 4D flow-MRI for cirrhosis patients.Methods
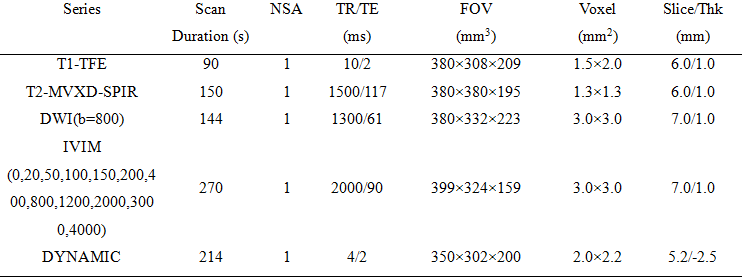
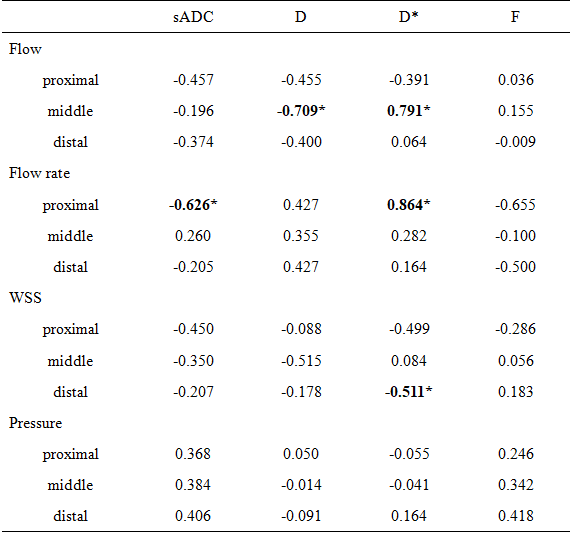
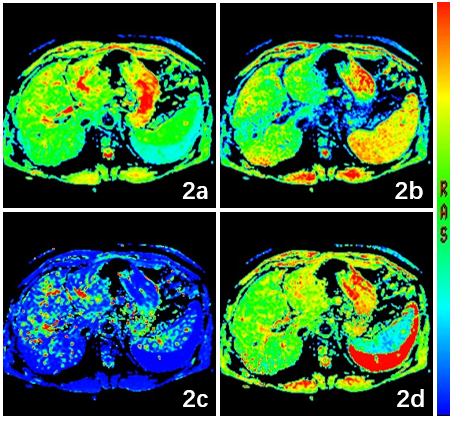
This study has been approved by the institutional IRB. 11 patients were recruited with informed consent acquired from each subject. All patients were scanned using a 3.0 T MR scanner (Ingenia CX, Philips Healthcare, the Netherlands) with a 16-channel abdominal array coil. The MR protocols include T1WI, T2WI, DWI, IVIM, 4D Flow and DYNAMIC sequence. For 4D Flow imaging, a 2D phase-contrast scan was performed first (axial, TR/TE = 4.4/2.7 ms, FOV = 200×200 mm2, resolution = 1.5×1.5×8 mm3, PC direction = RL, PC velocity = 200 cm/s, scan time = 13 s) to measure the flow velocity in the portal vein, as a reference for velocity encodings (VENC). The 4D Flow sequence with 8-fold compressed sensing acceleration was scanned with the following parameters: axial, TR/TE = 5.0/3.2 ms, FOV = 300×350 mm2, resolution = 2.5×2.5×2.5 mm3, PC direction = RL-AP-FH, VENC = 30 cm/s, scan time = 4min37s. The detailed parameters for all the other sequences were listed in Table 1. After the MR scan is completed, the 4D flow images were processed on CVI42 package (Canada Circle Cardiovascular Imaging)by an experienced radiologist to obtain the 3D angiogram. Four planes were manually placed vertical on the targeted vessel segments to measure the flow direction,the flow rate (cm/s), the axial-wall shear stress (WSS, Pa), and the pressure gradient (mmHg). Three planes were placed at the proximal, middle, and distal of the main portal vein and one at the splenic vein confluence as reference (Figure1). The images of other sequences were analyzed on a post-processing ISP workstation (Intelli Space Portal, Philips Healthcare) to measure IVIM parameters included: sADC, D, D* and F (Figure2). Spearman test (SPSS 22.0) was used to analyze the correlation between IVIM parameters and 4D flow-MRI parameters.Results
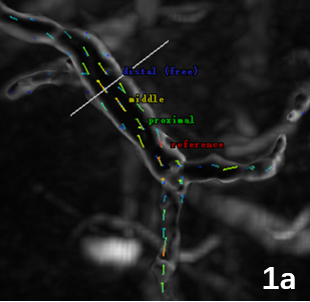
sADC and D values were negatively correlated with the proximal Flow rate (r=0.626, P<0.05) and the middle Flow rate (r=0.709, P<0.05), respectively. D* value was positively correlated with the middle Flow and proximal Flow rate (r=0.900, P=0.037). There was no correlation among the other parameters (P>0.05).Discussion and Conclusion
The changes in portal blood flow during the development of liver cirrhosis were associated with the variation of the signals in intrahepatic blood flow. There is a certain correlation among sADC and D values measured by IVIM and flow rate in 4D flow sequences. The mechanism behind this correlation need the further investigation and may shed light on the disease assessment and the development of novel therapies.Acknowledgements
No acknowledgement found.References
1.Intagliata NM, Caldwell SH, Tripodi A. Diagnosis, development, and treatment of portal vein thrombosis in patients with and without Cirrhosis. Gastroenterology. 2019 May;156(6):1582-1599.e1.
2.Chen F, Chen YL, Chen TW, Li R, Pu Y, Zhang XM, Li HJ, Tang S, Cao JM, Yang JQ. Liver lobe based intravoxel incoherent motion diffusion weighted imaging in hepatitis B related cirrhosis: Association with child-pugh class and esophageal and gastric fundic varices. Medicine (Baltimore). 2020 Jan;99(2): e18671. 3.Soulat G, McCarthy P, Markl M. 4D Flow with MRI. Annu Rev Biomed Eng. 2020 Jun 4; 22:103-126. 4.Luo J, Zhou K, Zhang B, Luo N, Bian J. Intravoxel incoherent motion diffusion-weighted imaging for evaluation of the cell density and angiogenesis of cirrhosis-related nodules in an experimental rat model: comparison and correlation with dynamic contrast-enhanced MRI. J Magn Reson Imaging. 2020 Mar;51(3):812-823. 5. Riedel C, Lenz A, Fischer L, Li J, Piecha F, Kluwe J, Adam G, Bannas P. Abdominal applications of 4D flow MRI. Rofo. 2020 Dec 2. English.
Figures