2079
4-D Flow CMR Reveals Inefficient PA Flow Correlates with Afterload in Repaired Transposition of the Great Arteries.1Pediatrics, Children's National Hospital, Washington, DC, United States, 2Sheikh Zayed Institute for Pediatric Surgical Innovation, Children's National Hospital, Washington, DC, United States, 3Industrial Engineering, Universita di Napoli Federico II, Naples, Italy, 4Pediatric Cardiology, Children's National Hospital, Washington, DC, United States
Synopsis
Repair of D- transposition of great arteries (DTGA) involves pulmonary artery (PA) manipulation that alters shape and flow patterns. Many patients experience increased right ventricular afterload and the etiology remains unclear. We examined the contribution of PA flow separation to afterload in these patients using 4D flow CMR imaging of a mock circulatory system incorporating 3D-printed PA replicas. We found that 2 distinct markers of flow inefficiency correlated with afterload. These data emphasize the utility of 4D flow CMR in quantifying abnormal blood flow and identifying important early clinical predictors of complications in DTGA.
Introduction:
Surgical treatment of D- transposition of great arteries (DTGA) involves the Arterial Switch Operation (ASO) and the LeCompte maneuver, where the pulmonary artery (PA) is translocated anterior to the neoaortic root, exaggerating branch pulmonary artery bending and stretching. In many patients, right ventricular dysfunction and increased right RV afterload is observed following ASO1,2. While pulmonary stenosis is a common postoperative complication, flow separation, flow inefficiencies, and energy loss created by this altered PA geometry may contribute to elevated RV afterload in a manner independent of stenosis. Our aim was to understand the correlation between RV afterload and flow characteristics produced by the ASO using 4D flow imaging of a mock circulatory system incorporating 3D printed replicas of ASO patients.Methods:
CMR imaging was analyzed from 16 patients with DTGA (average age 9.2 (+/-8.8) years, 69% male) with (31%) and without (69%) ventricular septal defect, who underwent ASO with LeCompte maneuver. Patients with pulmonary artery (PA) stents, pulmonary hypertension, or other anatomical confounders were excluded. Segmentation was performed on contrast-enhanced angiograms to create PA models that were 3D printed and mounted in an MRI-compatible mock circulatory system (MCS) with simulated PA resistance, compliance, and patient-specific pulsatile flow generated from an MRI-compatible flow pump. Patient-specific flow and resistance was calibrated in the circuit using iterative design and patients were excluded if PA flow curve kinetics could not be accurately reproduced (i.e. delayed systolic flow to branch PAs, n=3). Pressure transducers were utilized during flow simulations to gather peak systolic pressure change from circuit inlet to branch PA as an analog of RV afterload (ΔP). 4D Flow CMR (1.5T Siemens Aera) sequences of each simulation was obtained and flow patterns in systole were quantified using ITFlow© software (Cardio Flow Design, Japan).Results:
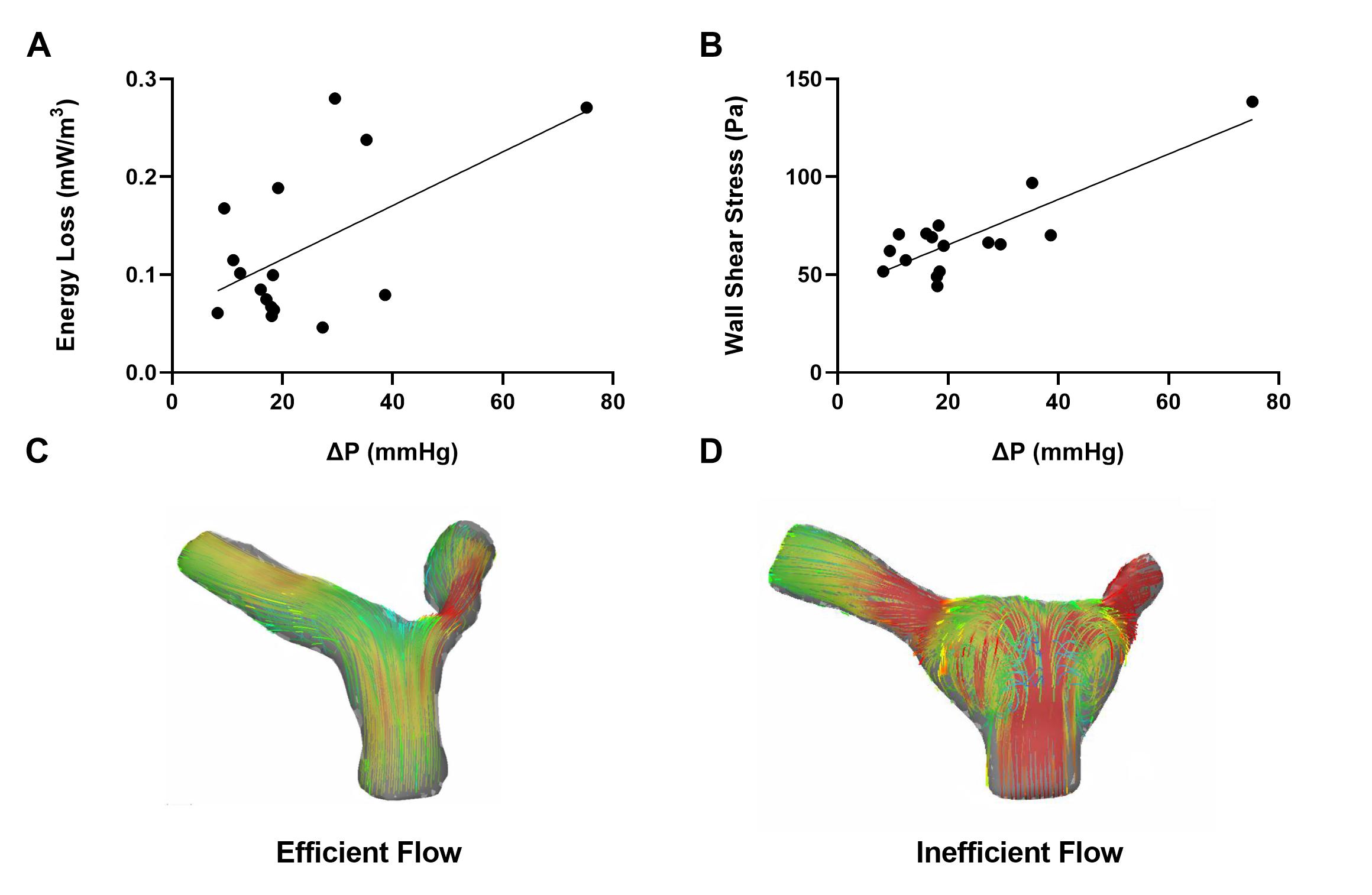
In post-ASO DTGA patients, analysis 4D flow data in MCS simulation reveals ΔP is significantly correlated to maximum systolic energy loss (mW/m3) (p = 0.021, r = 0.57) and maximum systolic PA wall shear stress (Pa) (p <0.001, r = 0.85).Discussion:
4D flow CMR allows the observation and quantification of flow inefficiencies in the post-ASO PA. Quantitative markers of flow inefficiency of peak energy loss and wall shear stress correlate strongly with simulated RV afterload in MCS simulations of post-ASO anatomy.Conclusion:
4D flow is a powerful tool to provide deeper understanding of flow field inefficiencies and subsequent energy loss in repaired DTGA. Inefficient PA flow patterns as quantified by 4D flow CMR are likely mechanistically related to RV afterload in this population and, with further research, may prove to be a clinically useful predictive factor for the management of complications in this growing patient population.Acknowledgements
This project was supported by Award Number R38AI140298 from the NIH National Center of Allergy and Infectious Diseases. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Center of Allergy and Infectious Diseases or the National Institutes of Health.References
1. Loke Y-H, Capuano F, Mandell J et al. Abnormal Pulmonary Artery Bending Correlates With Increased Right Ventricular Afterload Following the Arterial Switch Operation. World Journal for Pediatric and Congenital Heart Surgery 2019;10:572-581.
2. Klitsie LM, Roest AA, Kuipers IM, Hazekamp MG, Blom NA, Ten Harkel AD. Left and right ventricular performance after arterial switch operation. The Journal of thoracic and cardiovascular surgery 2014;147:1561-1567.
Figures