2072
Non-contrast 4D Dynamic Coronary MRA using Retrospective EPI (REPI) 4D-Flow Sequence
Yasuhiro Goto1, Michinobu Nagao1, Masami Yoneyama2, Yasutomo Katsumata2, Isao Shiina3, Kazuo Kodaira1, Takumi Ogawa1, Yutaka Hamatani3, Mamoru Takeyama3, Isao Tanaka1, and Shuji Sakai1
1Women's Medical University Hospital, tokyo, Japan, 2Philips Japan, tokyo, Japan, 3Tokyo Women's Medical University Hospital, tokyo, Japan
1Women's Medical University Hospital, tokyo, Japan, 2Philips Japan, tokyo, Japan, 3Tokyo Women's Medical University Hospital, tokyo, Japan
Synopsis
Since the REPI 4D MRA images the entire cardiac cycle, it may be possible to visualize the flow of the pulmonary artery, pulmonary vein, left ventricle, left ventricle, and aorta in addition to morphological evaluation of the coronary artery.The purpose of this study was to examine mainly LAD about the possibility of the practical use of REPI 4D MRA. REPI 4D MRA with choice of the VENC=30 cm/s could well visualize the coronary arteries from proximal to distal of the LAD.
Introduction
Coronary MR Angiography (MRCA) is widely used in the evaluation of coronary artery disease and has the great advantage of being free of radiation and requiring no contrast medium. (1)On the other hand, 3 Tesla has a high SAR limitation, which requires a low flip angle for MRCA imaging, so using the T1TFE sequence results in low coronary signal contrast [2]. Three Tesla MRI has a serious problem with banding artifacts due to B0 non-uniformity.(3)For this problem, we reported the usefulness of whole-heart coronary MR angiography using 3D non-selective bSSFP [4]. However, MRCA is it is mainly reported to assess the form of a coronary artery so far. In addition, the current CMRA uses electrocardiogram synchronization, and it is necessary to input and image the stationary end diastole of the heart. In this study, we proposed a new non-contrast-enhanced coronary MRA technique based on Retrospective EPI (REPI) 4D-Flow sequence (REPI 4D MRA) as an alternative to conventional coronary MRA. The purpose of this study was to explore the feasibility of REPI 4D MRA.Methods
A total of six volunteers (4 men, 2 women, age range 22 to 46) were examined on a 3.0T MRI (Ingenia, Philips Healthcare). The study was approved by the local IRB, and written informed consent was obtained from all subjects. Scheme of the REPI 4D MRA sequence is shown in Figure 1. TFEPI sequence is being combined with EPI readout, it is capable of scan time acceleration and improves SNR. In accordance with AHA classification, divided into four vessels from the main trunk # 5 of the left coronary artery to the left anterior descending peripheral # 8 as a segment, we evaluated the blood vessels of the coronary artery in five-point scales. Three radiologists evaluated the representation of the visual blood vessels. In REPI 4D MRA, setting of right VENC is critical. We evaluated the optimal VENC from 10cm/s, 30cm/s and 50cm/s. Statistical analysis was performed on the REPI 4D MRA by the Steel-Dwass test, and it was judged that there was a significant difference when p <0.05. Imaging parameters for REPI 4D MRA were: FOV (mm) = 300×300, spatial resolution (mm) = 1.8×1.8×1.8, TR/TE (ms) = 9.2/5.3, flip angle (° ) = 10, SENSE factor = 3, TFE-factor=1, EPI-factor=5, Recon heart phase = 15, acquisition time = 7m51s.Results & Discussion
As a result of visual evaluation, #5 was significantly lower in REPI 4D MRA with VENC=10cm/s than in VENC=30cm/s and VENC=50cm/s. Significant difference between VENC=30 and VENC=50cm/s was not found. There was no significant difference between # 6 and # 7 among VENC=10cm/s, 30cm/s and 50cm/s. In #8, VENC=50cm/s was significantly lower than VENC=10cm/s and VENC=30cm/s. To summarize the results, VENC=10cm/s was poorly visualized proximal to the coronary artery and VENC=50cm/s was poorly visualized distally. From the results, there is a possibility that the flow velocity is different between the origin and the periphery of the coronary arteries. Only VENC=30cm/s was able to depict both proximal and distal totally. However, this study was limited to the left coronary artery LAD. We will verify whether it can be used for RCA and CX. Compared with conventional coronary MRA, REPI 4D MRA does not require to explore exact timing for ECG trigger delay because this sequence applies retrospective cardiac gating, radiologists can find the good static MRA images retrospectively in addition to dynamic (like 4D Flow) information. Furthermore, REPI 4D MRA also has a potential to visualize the flow of the pulmonary artery, pulmonary veins, left atrium, left ventricle, and aorta in addition to morphological evaluation of the coronary arteries. In addition, since REPI 4D MRA is based on 4D flow sequence, it inherently has flow-phase information as well. Thus, the flow velocity might be measured from the same dataset. We will try to measure the flow velocity and flow rate and examine the possibility of calculating FFR in the next study.Conclusion
REPI 4D MRA with choice of the VENC=30 cm/s could well visualize the coronary arteries from proximal to distal of the LAD. REPI 4D MRA can construct images from the direction of high visibility of blood vessels.In addition to the evaluation of the coronary arteries, it was possible to visualize the flow of the pulmonary artery, pulmonary vein, left atrium, left ventricle, and aorta.Acknowledgements
No acknowledgement found.References
(1) Danias PG ,et al: Diagnostic performance of coronary magnetic resonance angiography as compared against conventional x-ray angiography: A meta-analysis.J Am Coll Cardiol. 2004 Nov 2; 44:1867-76. (2) Kaul MG ,et al: Evaluation of balanced steady-state free precession (TrueFISP) and K-space segmented gradient echo sequences for 3D coronary MR angiography with navigator gating at 3 Tesla.Rofo.2004 Nov:176:1560-5. (3) Thomas D1 ,et al: MR-coronary angiography: comparison of SSFP and spoiled GRE sequence (bright blood technique) and a TSE sequence (black blood technique) in healthy volunteers. Rofo. 2004 Nov:176:1589-98. (4) Shiina I ,et.al, ISMRM Virtual Conference & Exhibition, 2020.(Abstract2020).Figures
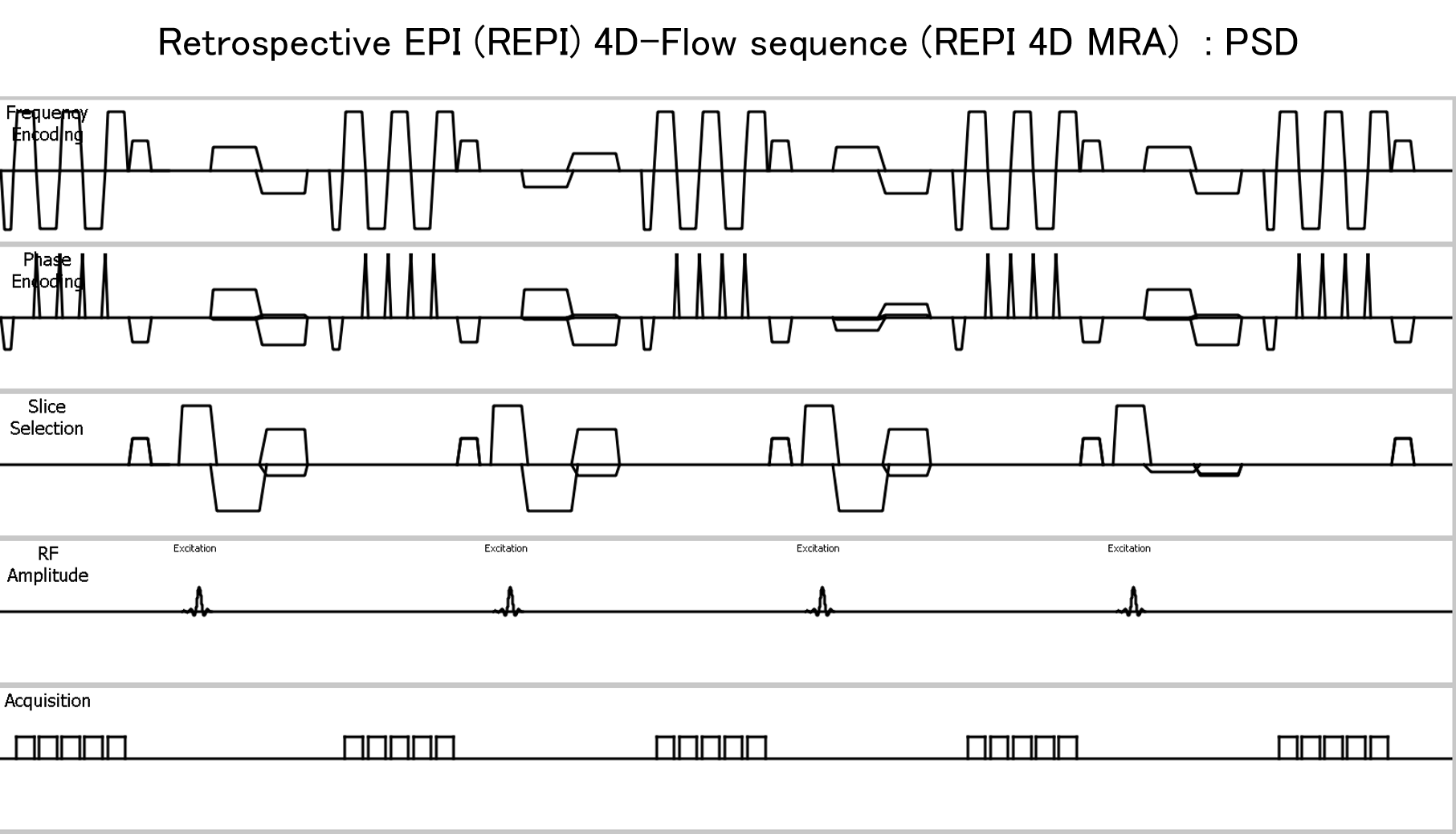
Figure 1.Scheme
of
the REPI 4D MRA sequence.
TFEPI sequence is being combined with EPI
readout, it is capable of scan time acceleration and improves SNR.
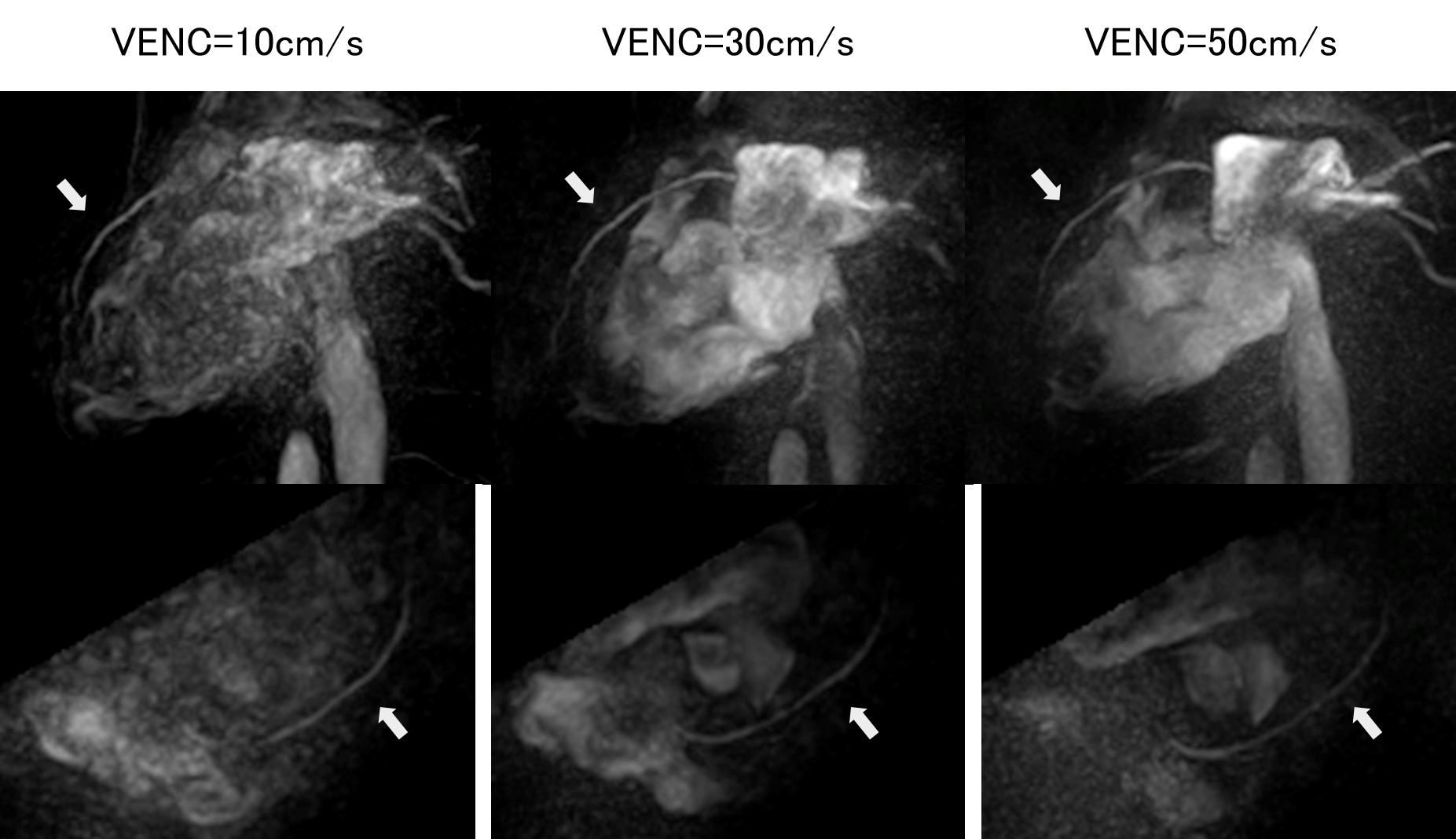
Figure 2. Dynamic coronary artery image with VENC= 10,30 and 50cm/s.
The optimal VENC = 30 cm / s REPI4D MRA
provides good visualization of the proximal to
distal portion of the left anterior descending artery (arrow).

Figure 3. REPI 4d MRA of VENC=30cm/s (upper row).
REPI can be visualized in a well-balanced
manner from the ostial to distal portion of the left
anterior descending artery.
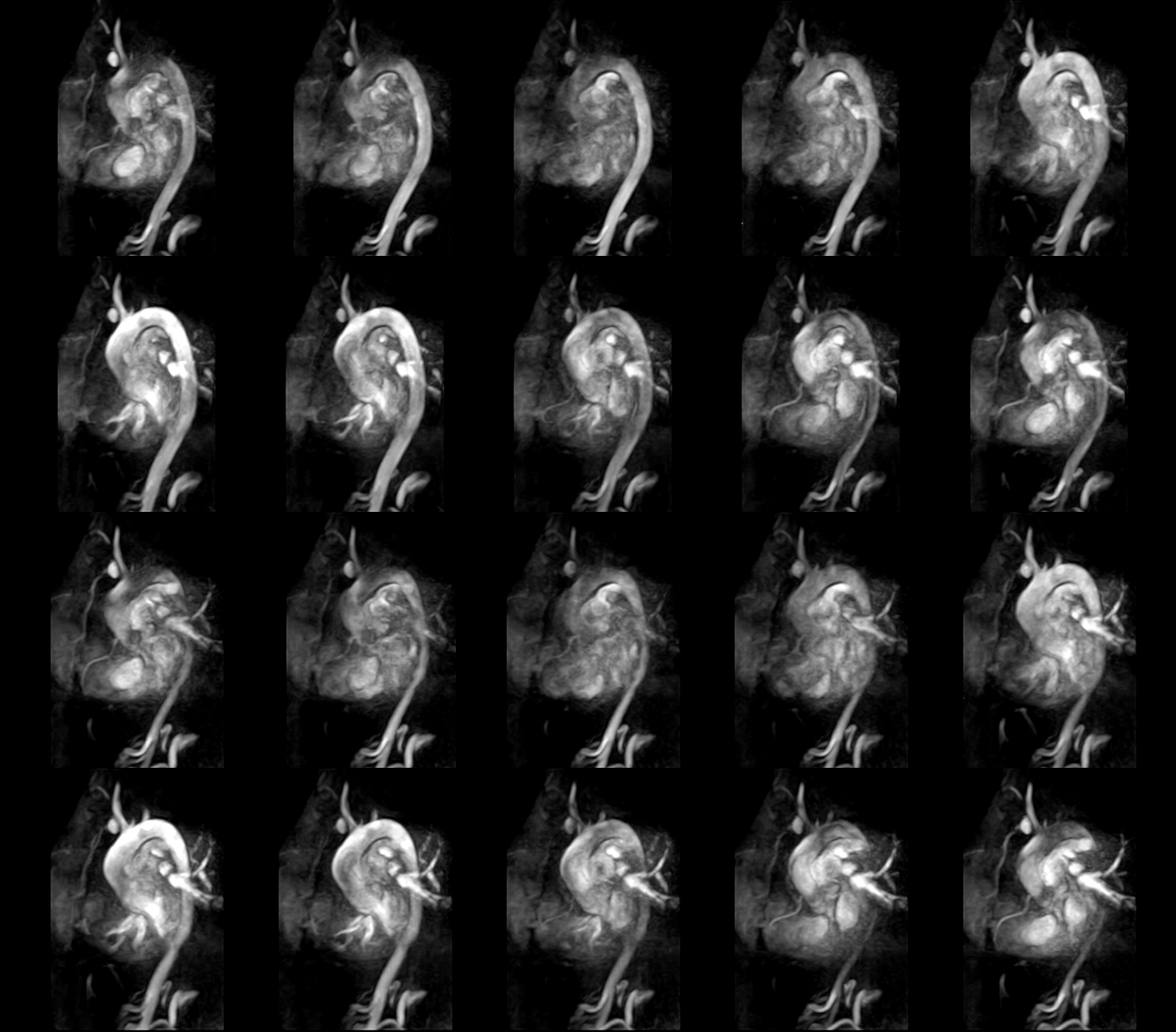
Figure 4. Heart and great vessels
dynamic images obtained from REPI.
Dynamic images demonstrate
three-dimensionally the blood flow in the heart,
great vessels, and coronary
arteries throughout a cardiac cycle.
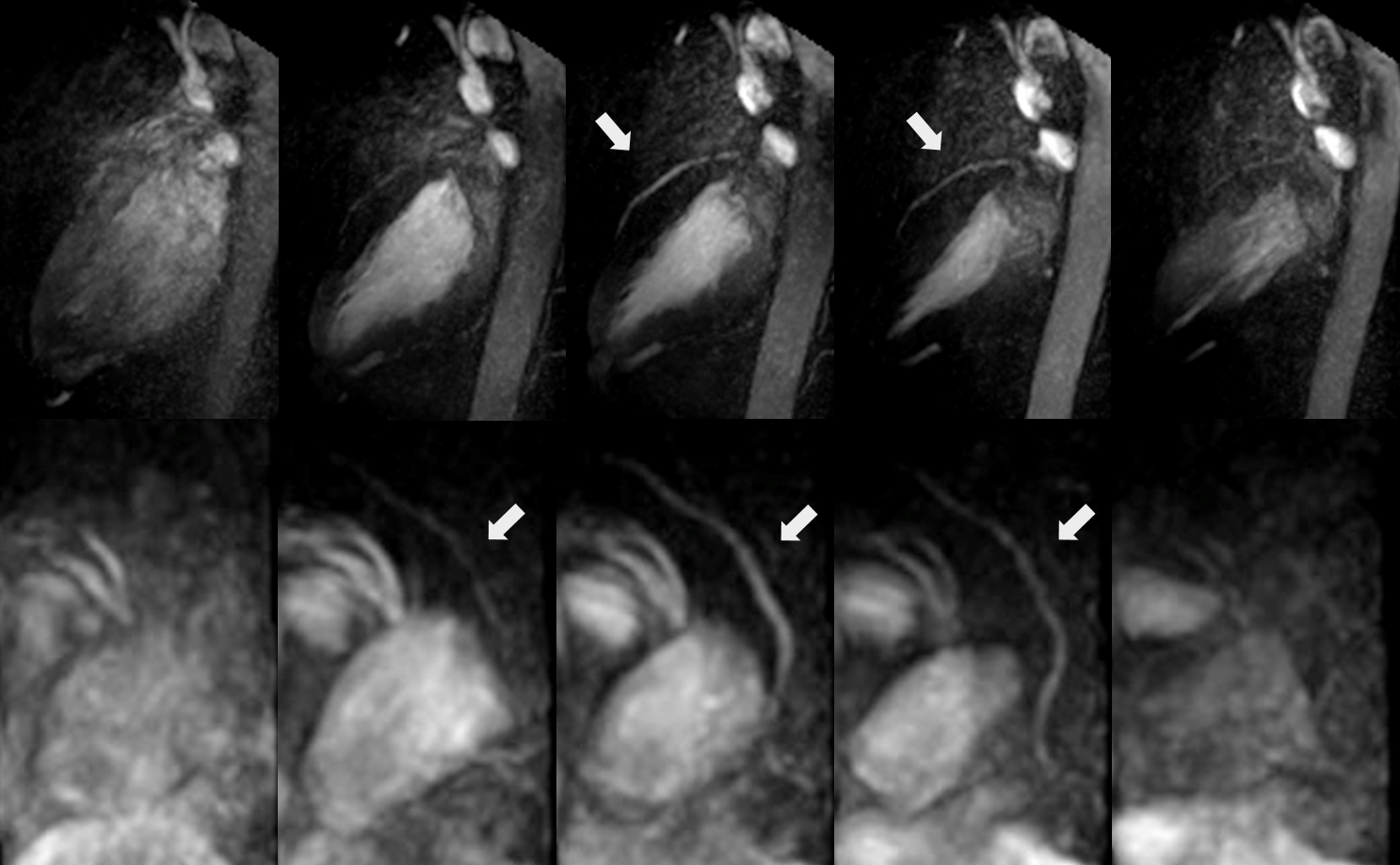
Figure 5. REPI 4D MRA can reconstruct oblique images along the left anterior descending artery (arrow).