2064
Attenuation of left ventricular blood flow kinetic energy and direct flow in repaired Fontan patients: a 4D flow MRI study1Shanghai Children's Medical Center, Shanghai, China, 2National Heart Centre Singapore, Singapore, Singapore, 3GE Healthcare, Shanghai, China, 4Duke-NUS Medical School, National University of Singapore, singapore, Singapore
Synopsis
Four-dimensional flow (4D flow) magnetic resonance imaging (MRI) enables the quantification of blood flow such as kinetic energy (KE) and flow components within the ventricular. Both KE and flow components is associated with ventricular diastolic and systolic function. This study aimed to quantify left ventricular (LV) KE and flow components in repaired Fontan patients in comparison to normal volunteers. The data showed that LV diastolic and systolic KE and direct flow were significant reduced, and residual flow increased in repaired Fontan patients.
Background and Purpose:
Long-lasting underfilling of the single ventricle (SV), increased ventricular afterload were obvious contributors to SV diastolic dysfunction. The low cardiac output and increased ventricular afterload leads to alterations in intracardiac hemodynamic. Four-dimensional flow (4D flow) magnetic resonance imaging (MRI) enables the quantification of blood flow within the ventricles and the aorta [1-3]. Intracardiac higher-order blood flow dynamic metrics such as kinetic energy (KE) and viscous energy loss (EL) can be calculated from 4D flow MRI and advanced analytics [4-5]. In recent years, Sjöberg et al demonstrated decreased left ventricular (LV) diastolic KE in young Fontan circulation patients [6]. Kamphuis et al reported that LV EL was increased in Fontan patients [7]. However, the detailed flow components (direct flow, residual flow, delayed ejection flow and retained inflow), and regional blood flow KE have not been studied in repaired Fontan patients. The purpose of this study was to 1) quantify LV blood flow KE globally and regionally, and flow components in repaired Fontan patients and normal volunteers; 2) compare the differences of cardiac pumping efficiency in repaired Fontan patients and normal volunteers.Method:
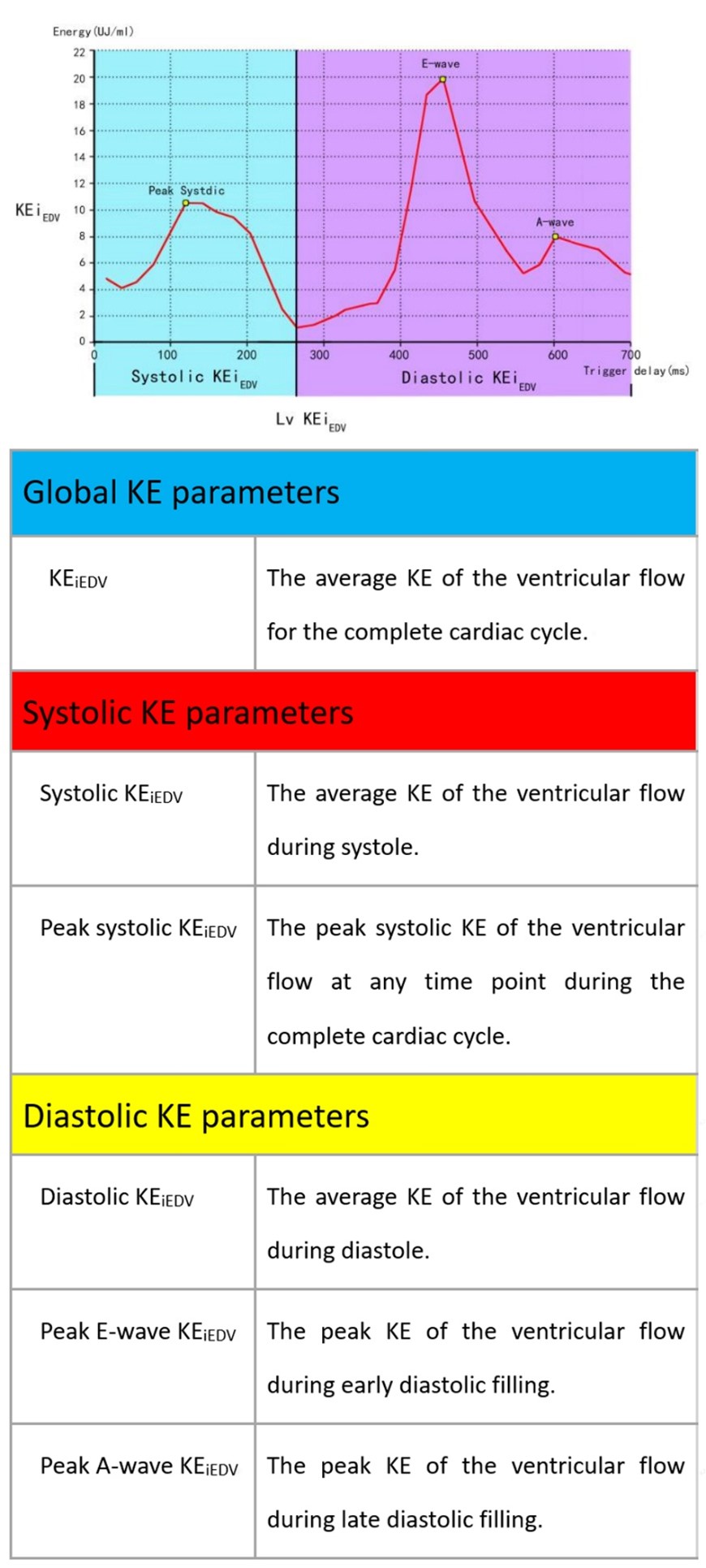
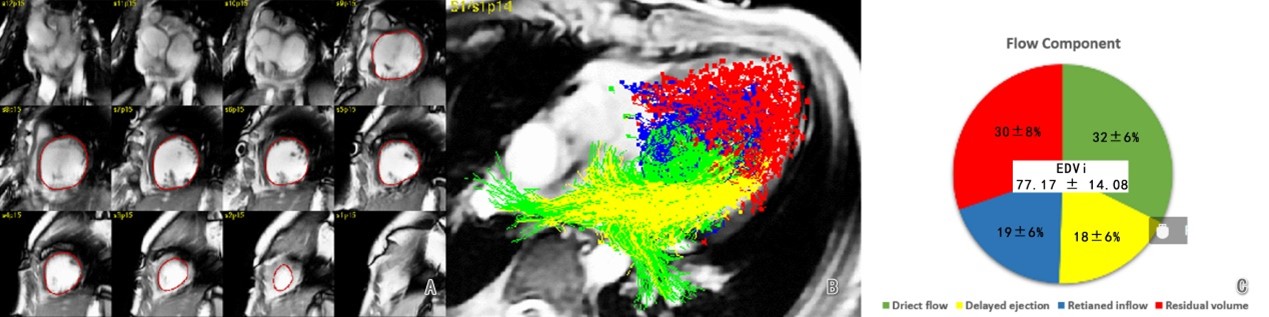
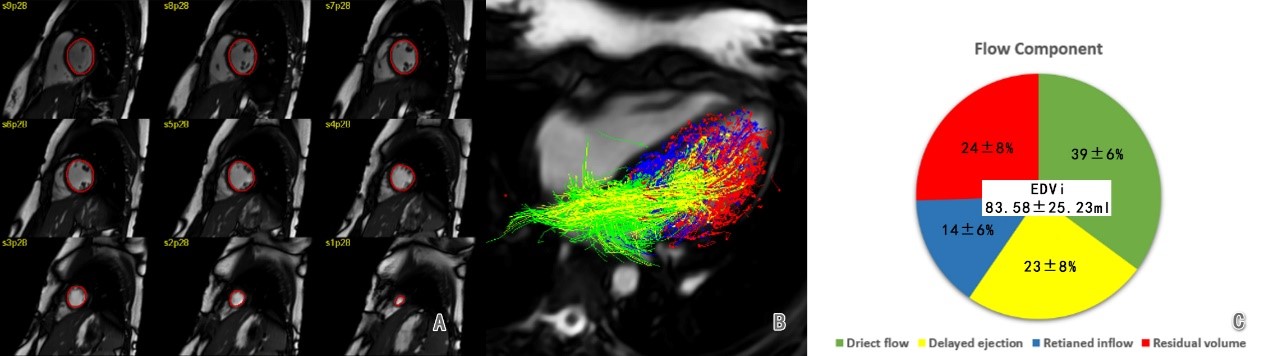
Twenty consecutive children with single ventricle physiology (10 systemic right ventricle, 10 systemic left ventricle) who had undergone Fontan operation between 2017 April and 2020 June were recruited. Fourteen age- and gender-matched normal controls were enrolled. 2D balanced steady state free precession cine sequences were performed with a 3.0 T MRI scanner (MR750, GE Healthcare, Milwaukee, WI) by short-axis view covering both ventricles to measure cardiac function. 4D flow Data sets were acquired with retrospective electrocardiographic (ECG)-gating during free-breathing. The image acquisition volume was in the transverse plane with full volumetric coverage of ventricular. Sequence parameters were as follows: echo time, 2.1 ms; repetition time, 4.3 ms; flip angle 8–12°; voxel size, 1.2 to 1.6×1.2 to 1.6×1.2 to 1.6 mm3; temporal resolution, 34.4-55 ms; velocity sensitivity, 160–200 cm/s; parallel imaging with reduction factor, R=2. From cine CMR images, left ventricular (LV) end-diastolic volume (EDV), end-systolic volume (ESV), stroke volume (SV) and ventricular mass were obtained from short-axis stacks using the dedicated software (CVI 42 Version 5.12.1; Circle Cardiovascular Imaging, Calgary, Canada). 4D flow MRI images were analyzed using MASS software (Version 2020EXP, Leiden University Medical Center, Leiden, The Netherlands). The LV blood flow KE curve was measured and KE parameters were quantified during systole and diastole phases (Figure 1), and all KE parameters were normalized by EDV. The LV flow components were measured (Figure 2 and Figure 3). Ventricular pumping efficiency or ventricular KE loss was determined as the ratio of aortic flow (QAO) and peak systolic KEiEDV.Results:
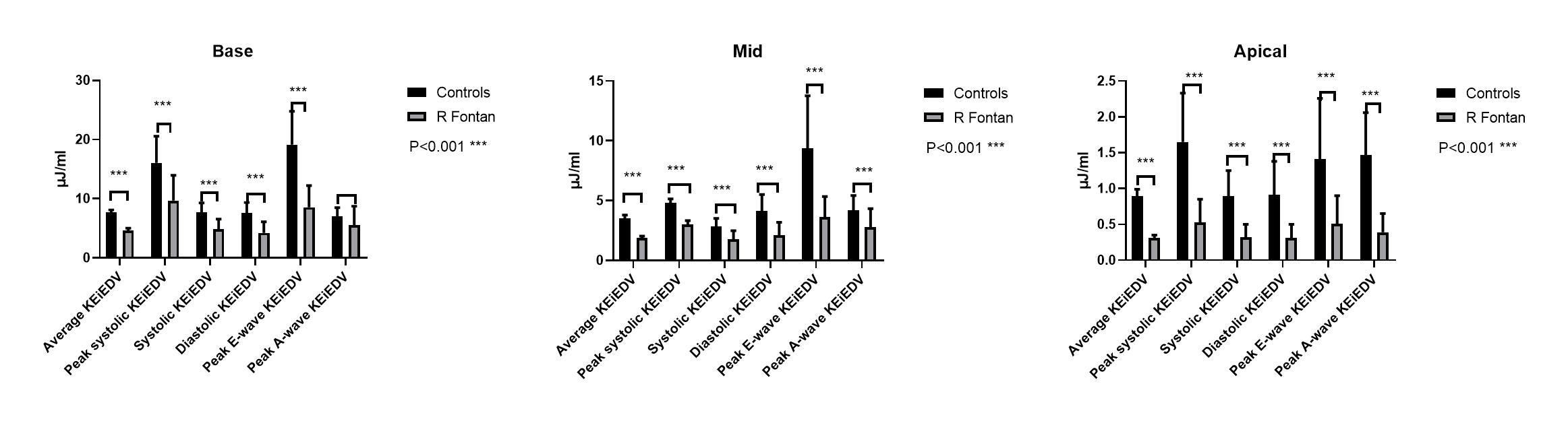
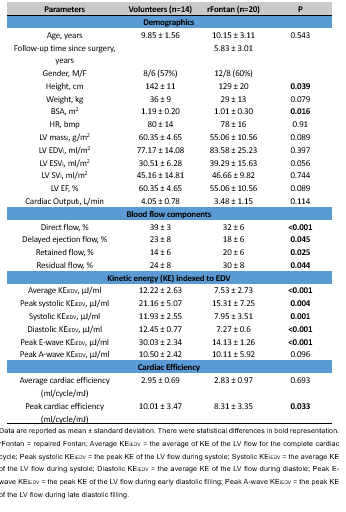
4D flow MRI data analysis were feasible for all participants. Patient’s demographics and LV volume and functional parameters, and flow components and KE parameters were summarized in Table 1. There were no significant differences in LV volume and functional parameters in rFontan patients than normal volunteers. rFontan patients had significant reduced direct flow (32 ± 6% vs. 39 ± 6%) and delayed ejection flow (18 ± 6% vs. 23 ± 8%), but increased retained flow (19 ± 6% vs. 14 ± 6%) and residual flow (30 ± 8% vs. 24 ± 8%) than the normal volunteers. rFontan patients had significant reduced average KEiEDV, peak systolic KEiEDV and systolic KEiEDV, diastolic KEiEDV and peak E-wave KEiEDV than the normal volunteers (all p<0.001). Peak cardiac efficiency was significantly lower in rFontan patients than normal volunteers (P=0.033). Furthermore, rFontan patients had impaired LV regional KE parameters at basal, mid and apical regions than the normal volunteers (Figure 4).Conclusions:
Left ventricular diastolic and systolic blood flow kinetic energies and pumping efficiency were attenuated in repaired Fontan patients compared to normal controls. Direct flow was significantly reduced and residual flow was significantly increased in repaired Fontan patients. This finding may suggest the ventricular KE and flow components from 4D flow MRI represent early imaging markers of ventricular filling and systolic abnormalities.Acknowledgements
No acknowledgement found.References
1. Soulat Gilles, et al. Annu Rev Biomed Eng, 2020, 22:103-126.
2. Garcia Julio, et al. JACC Cardiovasc Imaging, 2019, 12: 252-266.
3. Crandon Saul, et al. Int. J. Cardiol., 2017, 249: 486-493.
4. Zhong Liang, et al. J Magn Reson Imaging, 2019, 50: 677-681.
5. Wong James, et al. J. Appl. Physiol., 2018, 125: 889-900.
6. Sjöberg Pia, et al. Pediatr Cardiol, 2017, 38: 669-680.
7. Kamphuis Vivian P, et al. Eur Heart J Cardiovasc Imaging, 2019, 20: 323-333.
Figures