2049
The value of quantitative diffusion tensor MRI in diagnosis of hypoxic ischemic brain injury (HIBD) in premature infant1Third Affiliated Hospital of Zhengzhou University, Zhengzhou, China, Zhengzhou, China, 2College of Chemistry, Zhengzhou University, Zhengzhou, China, Zhengzhou, China, 3Zhengzhou Central Hospital Affiliated to Zhengzhou University, Zhengzhou, China, Zhengzhou, China, 4GE Healthcare, MR Research China, Beijing, China, Beijing, China
Synopsis
Diffusion tensor imaging (DTI) is currently the only non-invasive technology available to evaluate the damage to the cerebral white matter (WM) fibers in neonates, which can reflect the occurrence of damage through the decrease of FA values. This study aims to validate the value of diffusion tensor imaging (DTI) to diagnose and predict hypoxic-ischemic brain injury (HIBD) of preterm infants to assist clinical diagnosis and treatment.
Introduction
Neonatal hypoxic ischemic brain damage (HIBD) is a brain injury caused by fetal distress or perinatal asphyxia. Clinically, HIBD manifests a series of nervous system abnormalities 1. Diffusion tensor imaging (DTI) is performed by applying diffusion gradients along multiple directions and can estimate the orientation of white matter (WM) fiber bundles through measuring anisotropic diffusion 2. Due to the limitations of various conditions, there are few studies on DTI of preterm infants. In this study, we explored the application of DTI in diagnosis and prognosis of premature with HIBD by evaluating FA of white matter fiber bundles of preterm neonates with HIBD.Material and Methods
A total of 106 subjects who underwent MRI/DTI from February 2017 to June 2019 in our hospital were included in the study. In the patient group, all cases were clinically diagnosed as HIBD3 (n = 74).. Conventional T1-weighted anatomic MRI and DTI scans were obtained at term age in preterm infants and full-term infants with no brain injury. Conventional MRI and DTI were performed using a 3.0 T scanner (SKYRA, Siemens, Erlangen, Germany). Conventional MR images were obtained using the 3D T1-weighted magnetization-prepared rapid gradient echo (MPRAGE) sequence. The DTI scan was performed using spin-echo echo-planar imaging (SE-EPI) sequence and the parameters are slices 25, FOV 220×220 mm, slice thickness 5.0 mm, TR 3700 ms, TE 92.0 ms, resolution 128×128, average 1, b values 0 and 1000 s/mm2, directions 64, scan time 4’40’’. Forty-six of these infants (24 males, 22 females) were assessed for neurodevelopment (Bayley scales of infant development, BSID) at 6-7 months4. BSID score (both of the two subscores) > 79, favourable outcome; ≤ 79, adverse outcome, which needed the treatment and intervention.Results
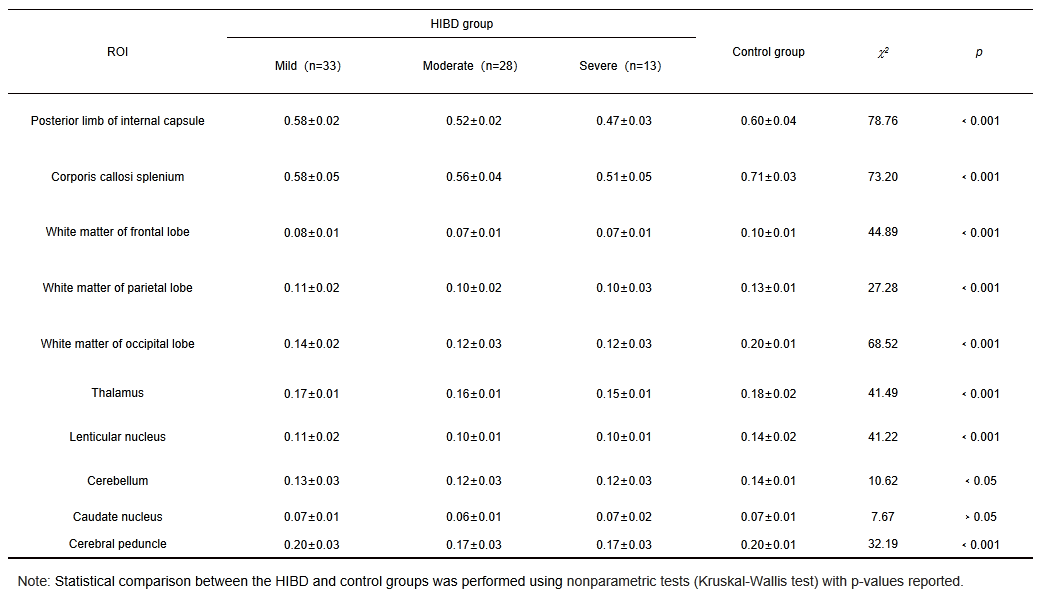
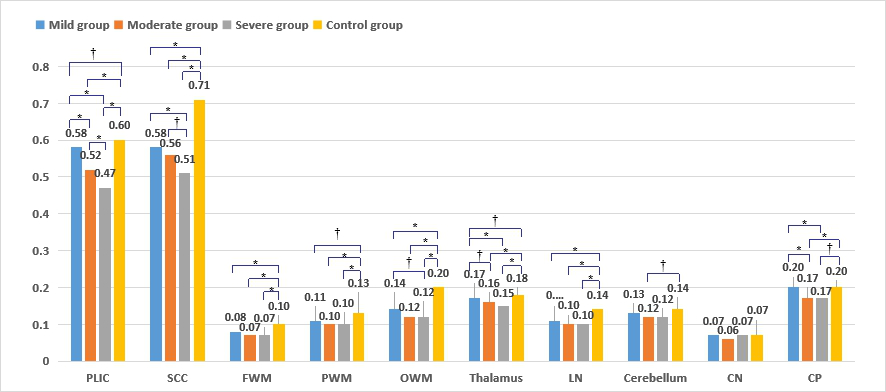
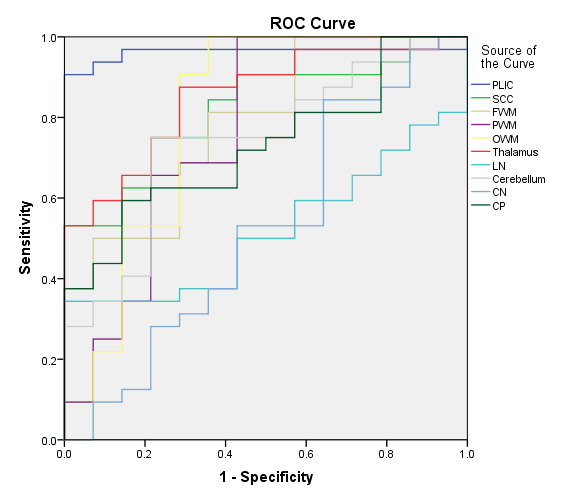
Table 1 compares the FA values between each subgroup (mild, moderate, and severe) and the control group. The four groups had significantly lower FA (p﹤0.05) in all the ROIs except caudate nucleus. Then, multiple comparisons were used to continue the analysis. The results showed that the FA values of PLIC had the most significant difference among the groups (Fig. 1). And we found that FA was correlated with the prognosis. Among the regions with reduced FA, PLIC had the largest area under the curve (AUC) in predicting the outcome (Fig. 2).Discussion
The results showed that FA was negatively correlated with HIBD and positively correlated with BSID. The higher the FA, the HIBD is less severe, and the better the outcome. In the study of prognosis, we found that the FA values of better prognosis group was generally higher than that of poor prognosis group, and most of the differences were statistically significant. It can be seen from the results that the FA values of most regions of interest (ROIs) in the better prognosis group are higher than that in the poor prognosis group, indicating that FA value can serve as a potential prognostic marker in premature infants with HIBD.Conclusion
DTI can detect microstructural damage and predict outcomes in premature infants with HIBD, potentially serving as an imaging biomarker for early diagnosis and prognosis of premature infants with HIBD.Acknowledgements
The National Natural Science Foundation of China (grants 81870983)References
1. Yang X, Zhong M, Chen J, et al. HIF-1<alpha> Repression of PTEN Transcription Mediates Protective Effects of BMSCs on Neurons During Hypoxia. Neuroscience 2018,10;392:57-65.
2. Winter JD, Lee DS, Hung RM, et al. Apparent diffusion coefficient pseudonormalization time in neonatal hypoxic-ischemic encephalopathy. Pediatric neurology 2007,37(4):255-62.
3. Li M, Jiang L, Zhang H, et al. Clinical significance of elevated serum A-FABP and free fatty acid in neonates with hypoxic ischemic brain damage. Experimental and therapeutic medicine 2016,12(2):746-752.
4. Bayley, N. Bayley Scales of Infant and Toddler Development, Third Edition (Bayley-III). San Antonio, TX: Harcourt Assessment, Inc; 2005.
Figures