1896
Diffusion tensor imaging in the tibial nerve in patients with diabetic peripheral neuropathy1New York Institute of Technology, Old Westbury, NY, United States, 2Department of Radiology, Bernard and Irene Schwartz Center for Biomedical Imaging, New York University Grossman School of Medicine, New York, NY, United States, 3Department of Radiology, Center for Advanced Imaging Innovation and Research, New York University Grossman School of Medicine, New York, NY, United States, 4Department of Physical Therapy, New York University, New York, NY, United States, 5Department of Radiology, Michigan State University, East Langsing, MI, United States
Synopsis
Prolonged type 2 diabetes mellitus (T2DM) can result in diabetic peripheral neuropathy (DPN), a disease in which ischemic conditions degrade peripheral nerves. Diffusion tensor imaging (DTI) studies have demonstrated significant microstructural changes in upper extremity pathology, yet limited research has focused on the tibial nerve. We found cross-sectional differences in apparent diffusion coefficient between controls and T2DM and DPN. In a separate longitudinal study, insignificant DTI changes were found in DPN patients that were scanned before and after a 10-week exercise intervention.
Introduction
Diffusion tensor imaging (DTI) has shown promise for quantitative assessment of neuronal integrity (1-6). Pathological conditions of peripheral nerves, such as diabetic peripheral neuropathy (DPN), may lead to loss of structural integrity and directional coherence of the nerve fibers, which can be measured by DTI. Neuropathy has been associated with decreased fractional anisotropy (FA), indicating lack of directional preference of protons within the nerve, and increased apparent diffusion coefficient (ADC), potentially indicating inflammation, edema, or injury.In this work, we use DTI to characterize the tibial nerve, which is at risk for degradation in DPN and can be difficult to probe due to its small size and central location in the calf. We investigate cross-sectional differences in neuronal health by measuring FA and ADC in the tibial nerve of healthy controls, individuals with T2DM without neuropathy, and those with DPN. In addition, inspired by recent literature that showed supervised exercise in DPN improved cardiorespiratory function, innervation (7-9) and nerve conduction (10), we investigated whether longitudinal changes in FA or ADC could be detected in the tibial nerve after a 10-week exercise intervention program.
Methods
The studies were conducted in accordance with New York University Langone Health’s Institutional Review Board, and all subjects provided informed written consent. Eighty-two individuals aged from 40 to 70 were enrolled in 2 studies: 50 in a cross-sectional study (16 control, 15 T2DM, and 19 DPN) with 1 MRI scan and 32 DPN in a longitudinal study with 3 MRI scans: 1. baseline, 2. follow-up; approximately 30 days after baseline, and 3. post-intervention, which followed a 10-week supervised, personal exercise program in which participants engaged in aerobic and strength training. The program consisted of 3 supervised sessions per week, which included moderate-intensity aerobic (50-70% of oxygen uptake reserve prescribed individually based on heart rate) (8) and resistance (bicep and triceps curls, bent rows, leg presses, and heel raises) components. DPN status was confirmed prior to MRI using the Michigan Neuropathy Screening Instrument (MNSI) (11).We scanned the mid-calves of all participants on a 3 Tesla MRI scanner (Prisma, Siemens Medical Solutions, Erlangen, Germany) with an in-house developed lower extremity coil (7). We measured FA and ADC using a DTI sequence with the following parameters: TR/TE=5300/65ms, voxel size=0.5×0.5×3.0mm, image matrix=128x128, FOV=160 mm, slice thickness=3mm, b-value=0 and 1200, number of diffusion encoding directions=12, number of slices=60. Initial tractography was completed in manually defined tibial nerve ROIs using MRTrix3 (12) with the assistance of fat-suppressed fast spin echo anatomical images (13). A threshold was subsequently applied to exclude voxels outside the central 37 slices or whose intensity was lower than 50% of the maximum in the tract. The resulting tract ROIs where used for calculation of mean ADC and FA. In the longitudinal cohort, the ADC and FA coefficient of variations (CV) were estimated as the standard deviation divided by the mean of the baseline and follow-up measurements.
Results
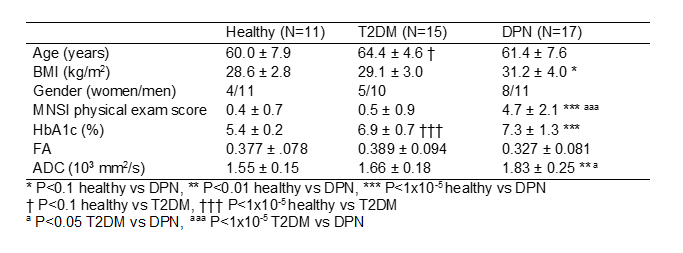
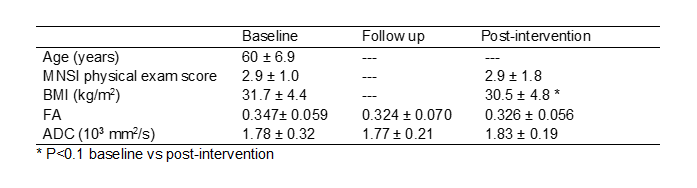
Participants were excluded from the analysis for the following reasons: subject withdrew from the longitudinal study (n=7), subject has not yet completed the longitudinal study due to covid-19 related suspension (n=5), severe motion artifacts prevented reliable tractography (n=5), errors related to corrupted raw data (n=5), or tract contained an insufficient number of slices (n=1). In the cross-sectional study, the ADC was significantly greater in DPN compared to that in controls and T2DM: 1.55±0.15×103mm2/s in controls, 1.66±0.18×103mm2/s in T2DM, and 1.83±0.25×103mm2/s in DPN (Table 1). The difference in ADC was significant between T2DM and DPN (P<0.05) and between controls and DPN (P<0.01). While ADC was 10% greater in T2DM compared to controls, the difference was not statistically significant (P=0.13).Table 2 lists the longitudinal DTI measurements. No significant changes were observed between FA or ADC values measured at baseline, follow up, or post-intervention (P>0.05). The CV was 11.1% for FA and 8.5% for ADC.
Discussion and Conclusion
We used DTI to evaluate the tibial nerve in the mid-calf in T2DM and DPN. In a cross-sectional study, we found significant ADC reduction in DPN compared to controls and T2DM, which is consistent with literature (1) and the hypothesis that pathologic conditions result in increased diffusion barriers in DPN. While we found reduced FA in DPN, the difference was not statistically significant in comparison to that in T2DM or controls.In the longitudinal study, we did not observe a significant difference in ADC or FA values following exercise intervention. The lack of change in the longitudinal data indicates that the 10-week exercise intervention did not improve tibial nerve microstructure to the extent necessary for detection with DTI. While not reported in this work, we observed significant reduction in calf adipose infiltration following the short-term intervention, indicating its efficacy for improving muscle composition. The potential disconnect between muscle composition and nerve remodeling suggests that more research is needed to determine the point at which nerve damage cannot be reversed and whether DTI is sensitive enough to track therapy response. In conclusion, this study affirms DTI can detect tibial nerve degradation in T2DM and DPN while its value for monitoring short-term intervention remains unclear.
Acknowledgements
This work was partially supported by National Institutes of Health grants T35 DK007421-37, R21 CA213169, R01 DK106292, R21 AG061579, R01 DK114428, R01-EB028774, and R21 EB027263 and was performed under the rubric of the Center for Advanced Imaging Innovation and Research (CAI2R, www.cai2r.net) at the New York University School of Medicine, which is an NIBIB Biomedical Technology Resource Center (P41 EB017183).References
1. Wu C, Wang G, Zhao Y, Hao W, Zhao L, Zhang X, Cao J, Wang S, Chen W, Chan Q, Zhao B, Chhabra A. Assessment of tibial and common peroneal nerves in diabetic peripheral neuropathy by diffusion tensor imaging: a case control study. Eur Radiol 2017;27(8):3523-3531.
2. Takagi T, Nakamura M, Yamada M, Hikishima K, Momoshima S, Fujiyoshi K, Shibata S, Okano HJ, Toyama Y, Okano H. Visualization of peripheral nerve degeneration and regeneration: monitoring with diffusion tensor tractography. Neuroimage 2009;44(3):884-892.
3. Lehmann HC, Zhang J, Mori S, Sheikh KA. Diffusion tensor imaging to assess axonal regeneration in peripheral nerves. Experimental neurology 2010;223(1):238-244.
4. Sheikh KA. Non-invasive imaging of nerve regeneration. Experimental neurology 2010;223(1):72-76.
5. Vaeggemose M, Pham M, Ringgaard S, Tankisi H, Ejskjaer N, Heiland S, Poulsen PL, Andersen H. Magnetic Resonance Neurography Visualizes Abnormalities in Sciatic and Tibial Nerves in Patients With Type 1 Diabetes and Neuropathy. Diabetes 2017;66(7):1779-1788.
6. Baumer P, Pham M, Ruetters M, Heiland S, Heckel A, Radbruch A, Bendszus M, Weiler M. Peripheral neuropathy: detection with diffusion-tensor imaging. Radiology 2014;273(1):185-193.
7. Fisher MA, Langbein WE, Collins EG, Williams K, Corzine L. Physiological improvement with moderate exercise in type II diabetic neuropathy. Electromyography and clinical neurophysiology 2007;47(1):23-28.
8. Kluding PM, Pasnoor M, Singh R, D'Silva LJ, Yoo M, Billinger SA, LeMaster JW, Dimachkie MM, Herbelin L, Wright DE. Safety of aerobic exercise in people with diabetic peripheral neuropathy: single-group clinical trial. Physical therapy 2015;95(2):223-234.
9. Kluding PM, Pasnoor M, Singh R, Jernigan S, Farmer K, Rucker J, Sharma NK, Wright DE. The effect of exercise on neuropathic symptoms, nerve function, and cutaneous innervation in people with diabetic peripheral neuropathy. Journal of diabetes and its complications 2012;26(5):424-429.
10. Breckwoldt MO, Stock C, Xia A, Heckel A, Bendszus M, Pham M, Heiland S, Baumer P. Diffusion Tensor Imaging Adds Diagnostic Accuracy in Magnetic Resonance Neurography. Invest Radiol 2015;50(8):498-504.
11. Herman WH, Pop-Busui R, Braffett BH, Martin CL, Cleary PA, Albers JW, Feldman EL, Group DER. Use of the Michigan Neuropathy Screening Instrument as a measure of distal symmetrical peripheral neuropathy in Type 1 diabetes: results from the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications. Diabetic medicine : a journal of the British Diabetic Association 2012;29(7):937-944.
12. Tournier JD, Smith R, Raffelt D, Tabbara R, Dhollander T, Pietsch M, Christiaens D, Jeurissen B, Yeh CH, Connelly A. MRtrix3: A fast, flexible and open software framework for medical image processing and visualisation. Neuroimage 2019;202:116137.
13. Constable RT, Smith RC, Gore JC. Signal-to-noise and contrast in fast spin echo (FSE) and inversion recovery FSE imaging. Journal of computer assisted tomography 1992;16(1):41-47.
Figures