1884
Accelerated Dynamic MRI for the Assessment of Esophageal Peristalsis During Swallowing
Ethan M I Johnson1, Sourav Halder2, Peter J Kahrilas1, John E Pandolfino1, Neelesh A Patankar2, and Michael Markl1
1Northwestern University, Chicago, IL, United States, 2Northwestern University, Evanston, IL, United States
1Northwestern University, Chicago, IL, United States, 2Northwestern University, Evanston, IL, United States
Synopsis
Pure pineapple juice was reduced by heating to a range of concentrations, and the T1 values were characterized for each concentration. A log-linear relationship between concentration factor and T1 reduction factor was shown. In vivo dynamic MR imaging of esophageal peristalsis was demonstrated using a modified MR angiography sequence and a 50% volume-reduced concentration of pineapple juice as swallowable contrast agent.
Introduction
Common methods for diagnosing esophageal motility disorders, such as achalasia, are manometry or barium swallow x-ray. MRI has been used to detect and stage esophageal cancers [1,2], but time-resolved morphologic MRI, necessary for identifying motility disorders, has been used only in limited feasibility studies [3-5]. Most of these studies have used orally-administered gadolinium contrast to show esophageal wall movement with 2D imaging sequences. A study of 3D morphologic esophageal imaging for targeting ablation interventions used concentrated pineapple juice to enhance the esophagus MRI signal, but motion depiction was not reported [6]. Pineapple juice naturally has a relatively short T1, on the order of 200-300ms, due to its manganese content, and concentrating it by reducing its volume reduces the T1 further [6]. The goal of this study is to systematically characterize the relationship of T1 reduction to juice volume reduction and to employ accelerated MR angiography techniques to perform time-resolved 3D imaging for visualization of esophageal peristalsis motion with an orally administered concentrated pineapple juice.Methods
Pure pineapple juice (100%, Costa Rica) was concentrated by microwave oven (Panasonic) to varied volumes to evaluate the effect upon T1. The juice was placed in a large glass container while microwaving, and intermittent pauses were used to avoid boiling over. The final volume (after heating) divided by initial volume, i.e. remaining percentage volume, was defined to be the juice volume reduction factor. Volumes were recorded from gradations on the glass container. A sample of unheated juice was reserved for reference T1 measurements. For volume-reduced juices, the T1 reduction factor was defined as the T1 value after heating divided by T1 value of the unheated juice. All juice samples were transferred to fill 30 mL plastic bottles for MR scanning. Measurements of T1 at 1.5T (Siemens/AERA) used a variable flip angle signal fit.A time-resolved contrast-enhanced 3D MR angiography sequence (Siemens/TWIST) was adapted for esophageal imaging with pineapple juice. Parameters used were (2.20mm)3 spatial / 2.1s temporal resolution, (352mm)2×141mm coronal FOV, 0.85ms TE, 2.48ms TR, 25° tip, 6/8 partial Fourier, R=2 GRAPPA, 8% central size / 10% outer density view sharing. A 4-channel cardiac coil placed on the upper torso surface was used for imaging. A healthy volunteer (37yo M) was given 10 mL or 20 mL of both raw juice (0% volume removed) and reduced juice (52% volume removed) during the MRI experiment. Juice was administered through a tube attached to a syringe controlled by the scan subject, following verbal instructions from the scan operator. Juice swallows were performed in the same scan session, in the following order: 20 mL raw, 10 mL raw, 20 mL reduced, 10 mL reduced.
Maximum intensity projections (MIPs) were created to visualize the juice bolus transit during esophageal peristalsis. Volume renders were created by intensity thresholding and seeded region growing in each time frame.
Results
The T1 and volume reduction factors for pineapple juice exhibit a log-linear relationship (fig. 1), with Pearson correlation of r=0.996 (p<0.001). Time-resolved 3D MRA images clearly depicted the movement of the concentrated juice through the esophagus during peristalsis in the human subject volunteer, both for 10 mL and for 20 mL swallows (fig. 2A). The bolus was observed in the esophagus for 3 frames during the 10 mL swallow and for 4 frames in the 20 mL swallow. Swallows of raw pineapple juice were not well visualized due to low conspicuity of the raw juice (fig. 2B).Discussion
Although the unprocessed pineapple juice T1 is short relative to many naturally occurring liquids, concentrating the juice is necessary for use as a contrast agent to visualize esophageal peristalsis motion. The T1 for concentrated juice is reduced in log-proportion to its volume reduction, and it can be achieved by heating the juice to evaporate water. When juice is heavily concentrated the viscocity can increase, but at 50% reduction no impacts upon swallowing were noted. Depiction of the bolus transit in a healthy volunteer was shown here. Evaluation of this technique in patients with achalasia or other esophageal motility disorders is a requisite next step for clinical translation. Some clinical studies, such as manometry, are conducted with patients supine, so positioning for MRI of esophageal disorders is not expected to pose a challenge. Barium swallow procedures are typically conducted with 5 mL bolus volumes, so investigating MRI of swallows smaller than 10 mL would be valuable. It may be necessary to improve spatial or temporal resolution by refining sequence parameter selection, or to test at a higher, 3T field strength for increased signal. The short T1 characteristic of pineapple juice exists also at 3T [7], but its exact T1 values should be confirmed.Conclusion
Dynamic morphologic imaging of esophageal peristalsis using concentrated pineapple juice as a contrast agent is feasible using a commercially available highly-accelerated time-resolved 3D MR angiography sequence. Concentrating the juice is critical in order to shorten its T1 and thereby develop adequate signal for clear bolus depiction as it transits the esophagus. Future work to evaluate depiction of esophageal motility disorders would be beneficial for demonstrating clinical utility.Acknowledgements
NIH TL1TR001423References
[1] Petrillo R, Balzarini L, Bidoli P, Ceglia E, D’Ippolito G, Tess JDT, et al. Esophageal squamous cell carcinoma: MRI evaluation of mediastinum. Gastrointest Radiol. 1990 Dec;15(1):275–8.[2] Riddell AM, Hillier J, Brown G, King DM, Wotherspoon AC, Thompson JN, et al. Potential of Surface-Coil MRI for Staging of Esophageal Cancer. American Journal of Roentgenology. 2006 Nov;187(5):1280–7.
[3] Panebianco V, Habib FI, Tomei E, Paolantonio P, Anzidei M, Laghi A, et al. Initial experience with magnetic resonance fluoroscopy in the evaluation of oesophageal motility disorders. Comparison with manometry and barium fluoroscopy. Eur Radiol. 2006 Sep;16(9):1926–33.
[4] Kulinna-Cosentini C, Schima W, Cosentini EP. Dynamic MR imaging of the gastroesophageal junction in healthy volunteers during bolus passage. J Magn Reson Imaging. 2007 Apr;25(4):749–54.
[5] Marciani L. Assessment of gastrointestinal motor functions by MRI: a comprehensive review: Functional GI MRI. Neurogastroenterology & Motility. 2011 May;23(5):399–407.
[6] Faletti R, Gatti M, Di Chio A, Fronda M, Anselmino M, Ferraris F, et al. Concentrated pineapple juice for visualisation of the oesophagus during magnetic resonance angiography before atrial fibrillation radiofrequency catheter ablation. Eur Radiol Exp. 2018 Dec;2(1):39.
[7] Zhang S, Olthoff A, Frahm J. Real-time magnetic resonance imaging of normal swallowing. J Magn Reson Imaging. 2012 Jun;35(6):1372–9.
Figures
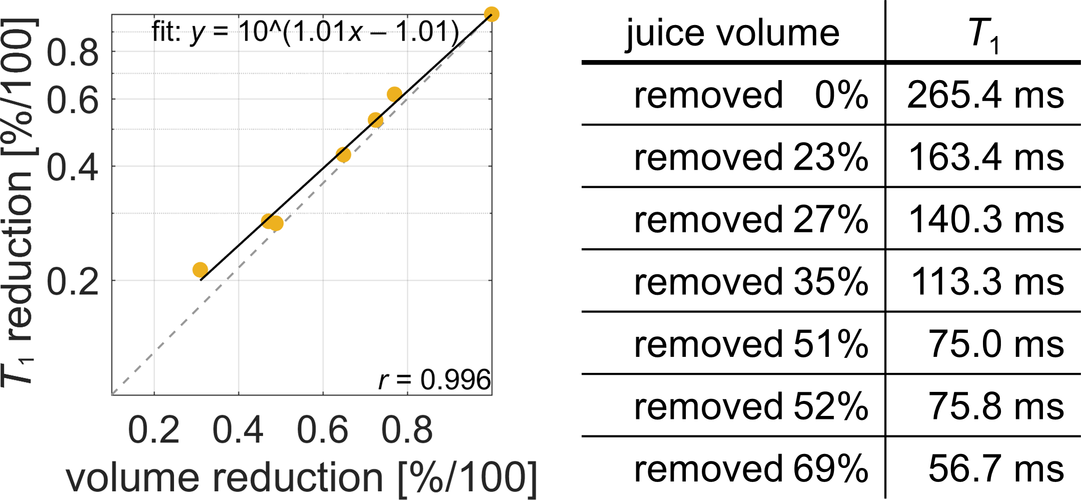
Figure 1. A plot of the measured T1 in pineapple juice at various volume-reduction factors (left) depicts the log-linear relationship between juice T1 reduction and juice volume reduction (right). The dashed line shows a one-to-one log-linear relationship for reference, and the solid line shows the empirical fit. The Pearson correlation coefficient for juice T1 reduction vs. volume reduction is 0.996 (p<0.001).
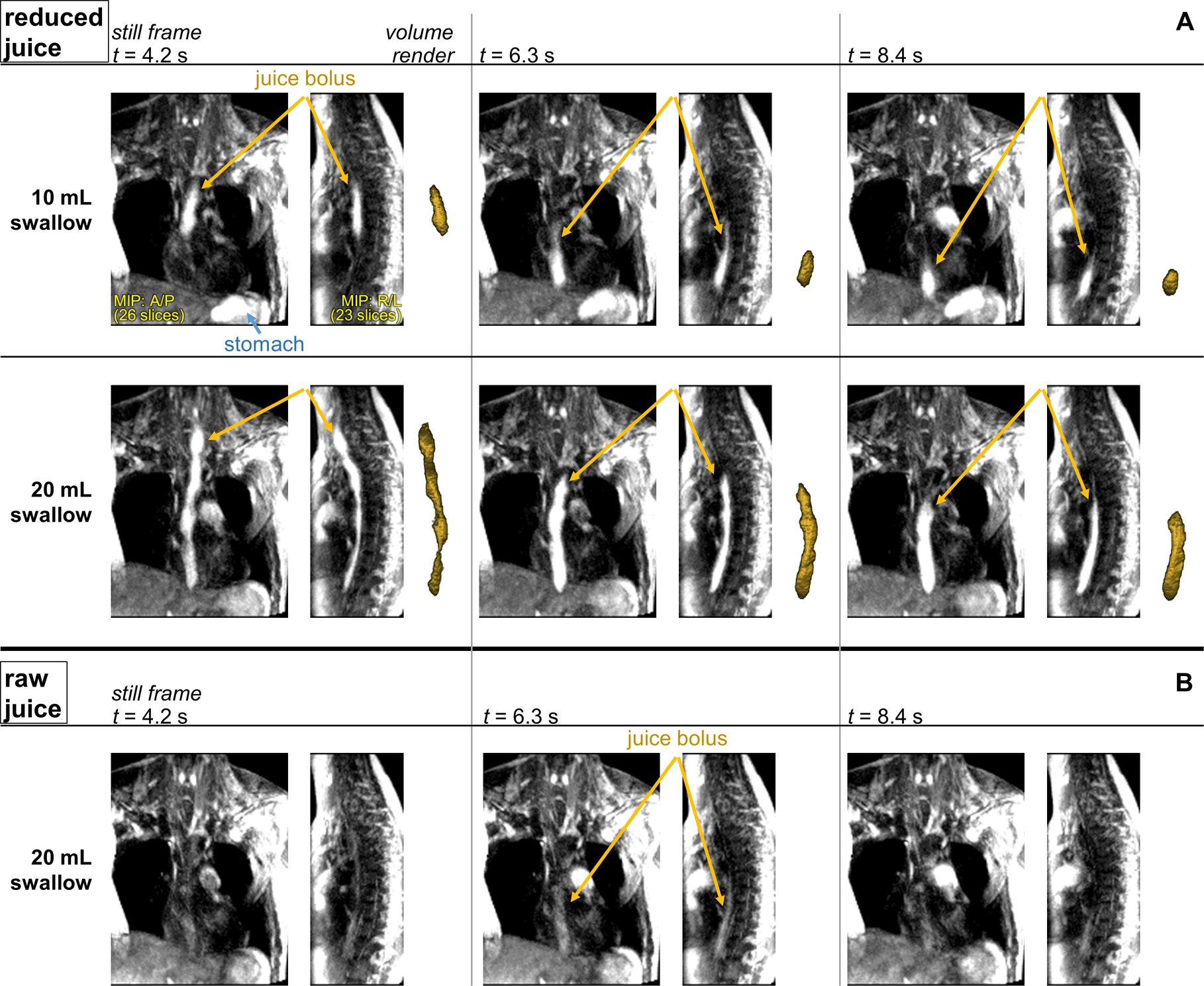
Figure 2. Using a modified MR angiography sequence with view-sharing and parallel imaging acceleration, a reduction of pineapple juice (50% volume) can be clearly and dynamically visualized in the esophagus as it is transported by peristalsis (A). Juice from the 20 mL swallow is visible in the stomach during the 10 mL swallow, which was performed after the 20 mL swallow. Renders of the bolus created by seeded region-growing image intensity thresholding are shown next to MIPs for each time frame. Peristalsis is not well visualized by a swallow of raw pineapple juice (B).