1869
Relationship Between Pancreatic Proton Density Fat Fraction and HOMA-IR in Individuals With and Without HIV Infection
Edgar Adrian Castellanos1, Susan Noworolski2, Diana Alba3, Peter Hunt3, and Suneil Koliwad3
1Department of Radiology and Biomedical Imaging, University of California , San Francisco, San Francisco, CA, United States, 2Department of Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States, 3Department of Medicine and Diabetes Center, University of California, San Francisco, San Francisco, CA, United States
1Department of Radiology and Biomedical Imaging, University of California , San Francisco, San Francisco, CA, United States, 2Department of Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States, 3Department of Medicine and Diabetes Center, University of California, San Francisco, San Francisco, CA, United States
Synopsis
Individuals with HIV+ infection have a higher rate of progression to type 2 diabetes mellitus (T2DM), although the mechanisms are not fully understood. Pancreatic proton density fat fraction (PDFF) measures were shown to not differ between individuals with HIV+ (n=16) and controls (n=16). However, when stratified to high versus low measures of insulin resistance (using HOMA-IR), individuals with HIV+ infection (but not controls), who had high HOMA-IR had higher pancreatic PDFF than those with low HOMA-IR, p=0.01. These results suggest pancreatic PDFF may be useful to monitor in HIV+ infection.
Introduction
It is understood that people infected with Human Immunodeficiency Virus (HIV) are more prone to develop type 2 diabetes mellitus (T2DM). However, the mechanism for this is not well known. A better understanding of the processes involved in this risk of progression to T2DM may aid clinical management of these individuals. Fat in the pancreas has been measured with MR and, in comparison to healthy individuals, higher levels have been associated with insulin resistance and even higher levels with diabetes.1 The amount of fat in the pancreas has not been well studied in individuals with HIV infection, nor has its association with markers of insulin resistance – a known risk factor for T2DM. The goals of this study were to determine if MR-measured pancreatic fat differed between individuals with and without HIV-infection, and if MR-measured pancreatic fat differed between those with high versus low measures of insulin resistance within these cohorts.Methods
We investigated a cohort of 32 individuals, half with HIV infection (n=16) and half as controls, without HIV infection (n=16). Those in the HIV+ cohort were all “stable” status, which meant individuals were under long-term treatment and their viral load was controlled and not progressing into acquired immunodeficiency syndrome (AIDS). Glucose and insulin levels were acquired after a 10 hour fast. The Homeostatic Model of Insulin Resistance (HOMA- IR) was calculated from these values. HOMA-IR values were classified as high versus low using a 2.2 mmol/mU cutoff, which split our control cohort into equal groups.MR imaging was acquired using a 3T GE scanner (GE Healthcare), including a Iterative Decomposition of water and fat with Echo Asymmetry and Least-squares estimation (IDEAL) sequence with 5mm thick axial slices over the abdomen. From the six acquired images in this sequence, the scanner software generated maps of water, fat, R2*, and fat fraction (in %). We generated a proton density fat fraction map in units of 10-times % (FF10) to capture the low levels of fat typically found in the pancreas using the formula: FF10 = (fat × 1000) / (fat + water). Regions of interest (ROIs) were drawn manually within the pancreas on the FF10 maps using in-house software written in IDL ( ITT Visual Information Solutions). Edges of the pancreas were excluded in all three dimensions. Student t-tests were performed between groups to assess significance using the statistical program JMP 15 Pro(SAS Institute) .
Results
No significant differences were found between the HIV+ and HIV- cohorts for pancreatic fat fraction, fasting glucose, fasting insulin, or HOMA-IR. In the control (HIV-) cohort, no significant difference was found for pancreatic fat fraction between those with high HOMA-IR (n=8) and those with low HOMA-IR (n=8), p=0.19 (See Figure 1). However, in the cohort that was HIV+, pancreatic fat was higher in those with high HOMA-IR (n=10) versus those with low HOMA-IR (n=6), p=0.01 (See Figure 2).Discussion and Conclusion
These results suggest there is a possible relationship between higher fat deposition in the pancreas with higher HOMA-IR levels in individuals with HIV+ infection. While there was a wide spread of pancreatic fat fraction in this study, most notably, the individuals with HIV+ infection and high HOMA-IR did not have low levels of pancreatic fat fraction. This greater damage to the pancreas is consistent with the fact that individuals with HIV+ infection have a greater risk of developing T2DM. Whether or not these particular cases would progress to T2DM will require following these individuals. However, as elevated pancreatic fat fraction is associated with insulin resistance and with T2DM, these results suggest measuring the pancreatic fat fraction in individuals with HIV+ infection may be valuable and may aid in the understanding of the development of insulin resistance and T2DM.Acknowledgements
Funding from: NIH: R01DK112304
Diabetes Center
References
1. Szczepaniak LS, PHD1, Victor RG, MD1, Mathur R, MD1, Nelson M D., PHD1, Szczepaniak E.D, PHD1, Tyer N, MD1, Chen I, PHD1, Unger R.H, MD2, Bergman R N., PHD1 and Lingvay I, MD2 Pancreatic Steatosis and Its Relationship to β-Cell Dysfunction in Humans. Diabetes Care 2012 Nov; 35(11): 2377-2383.Figures
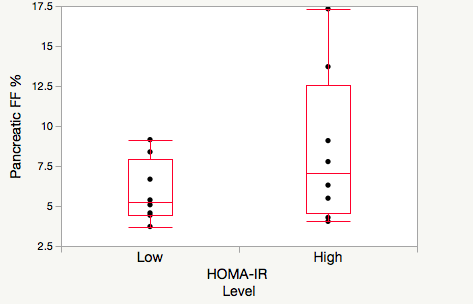
Figure 1 Pancreatic fat fraction in high (>2.2ml/mU) HOMA-IR (n=8) and low (<2.2 mmol/mU) HOMA-IR (n=8) in the HIV- cohort.
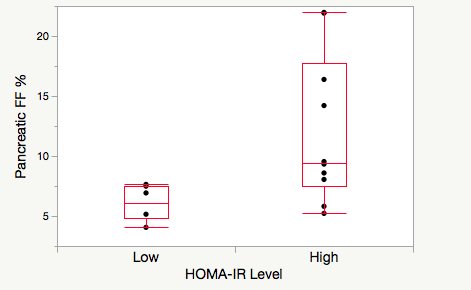
Pancreatic fat fraction in high (>2.2ml/mU) HOMA-IR (n=6) and low (<2.2 mmol/mU) HOMA-IR (n=10) in the cohort with HIV+.