1829
The “Prequence” Concept: Toward Significantly Faster Clinical MRI Exams1Radiology, University of Pittsburgh, Pittsburgh, PA, United States, 2University of Pittsburgh, Pittsburgh, PA, United States, 3Bioinformatics, University of Pittsburgh, Pittsburgh, PA, United States
Synopsis
Availability of clinical fMRI would be much improved via reduction of clinical exam times. A major factor in length of exam times is that typical MRI pulse sequences are optimized for a single image contrast (T1, T2, FLAIR, etc.) necessitating multiple pulse sequences each with significant “dead time” to acquire all desired contrasts for a given protocol. We here propose instead the time-efficient “prequence” (protocol sequence) concept which aims at acquisition of all desired contrasts in one or only a few sequences with minimal dead time. Preliminary proof-of-concept is demonstrated via a simultaneous T1/T2 contrast whole-brain neuro acquisition.
Introduction
A significant barrier to more widespread clinical use of MRI is the length of time required for a clinical MRI exam, which can range from 30 to 60 minutes for a typical neuro exam. Long exam times not only limit patient throughput, but also create difficulties with patient compliance, especially in pediatric and/or cognitively impaired populations, and repeated sedation for MRI is a neurological risk factor1. Shortening exam times is especially important for low-field MRI likely to become prevalent in developing countries due to the substantially decreased cost; low-field MRI inherently requires longer times due to the lower intrinsic SNR.A significant factor resulting in long MRI exam times is that typically a single pulse sequence is dedicated to each type of desired contrast: e.g. one scan for T1 contrast, another for T2 contrast, another for SWI, another for FLAIR, etc. Each of these individual pulse sequences, while optimized for the desired contrast, is highly time-inefficient as it involves “dead time” waiting for spins to acquire the desired contrast characteristics. We propose here the “prequence” (protocol sequence) concept whereby a single scan or set of scans are optimized to acquire all the contrasts required for a particular exam and demonstrate proof-of-concept via a simultaneous T1- and T2-weighted acquisition.
Methods
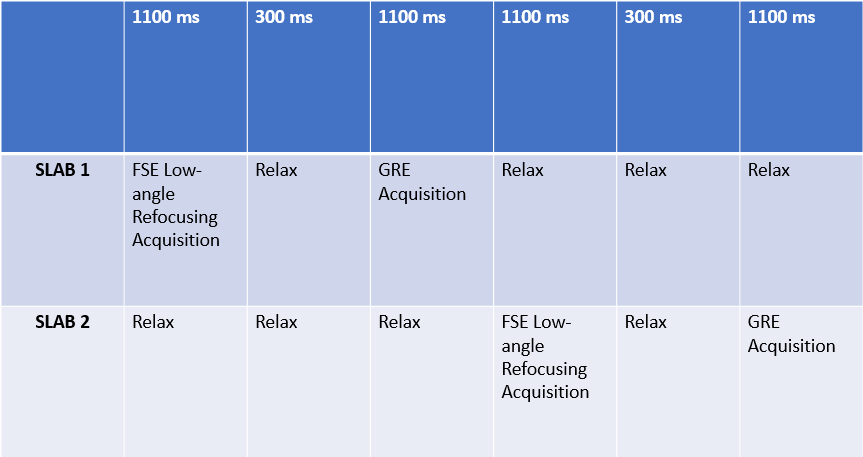
A two-slab sequence for simultaneous acquisition of T1 and T2 contrasts was designed as proof-of-concept (Figure 1). An FSE-like pulse train (echo spacing = 7 ms, 160 echoes) with low flip-angle refocusing followed by an RF-spoiled FLASH (TR = 7 ms, 160 excitations) was acquired for one slab. During this time, spins from the other slab are longitudinally relaxing after the FLASH acquisition to ensure signal for the next FSE acquisition pulse train. The low-angle refocusing flip angles for the FSE were optimized in order to produce exponential-like decays for gray and white matter, with the maximum contrast at the center of the echo train; the flip angles for the FLASH acquisitions were optimized in order to produce the most combined (T1 and T2) gray-white contrast at the center of ky-space, with a penalty term to minimize unwanted T1 contrast during the T2-weighted acquisition. (All optimizations were performed using in-house routines written in IDL).The T1/T2 prequence was implemented on a Siemens 3T Prisma system (image resolution = 1 mm isotropic) and images were obtained from a normal adult male volunteer. Specially tailored RF excitation and low flip-angle refocusing high-bandwidth VERSE2 pulses were used to minimize slab boundary artifacts while not exceeding the peak RF power available on the system. The high bandwidth (~30 kHz) pulses used also minimize signal loss in adjacent slabs due to MT effects and off-resonance saturation3.
Results
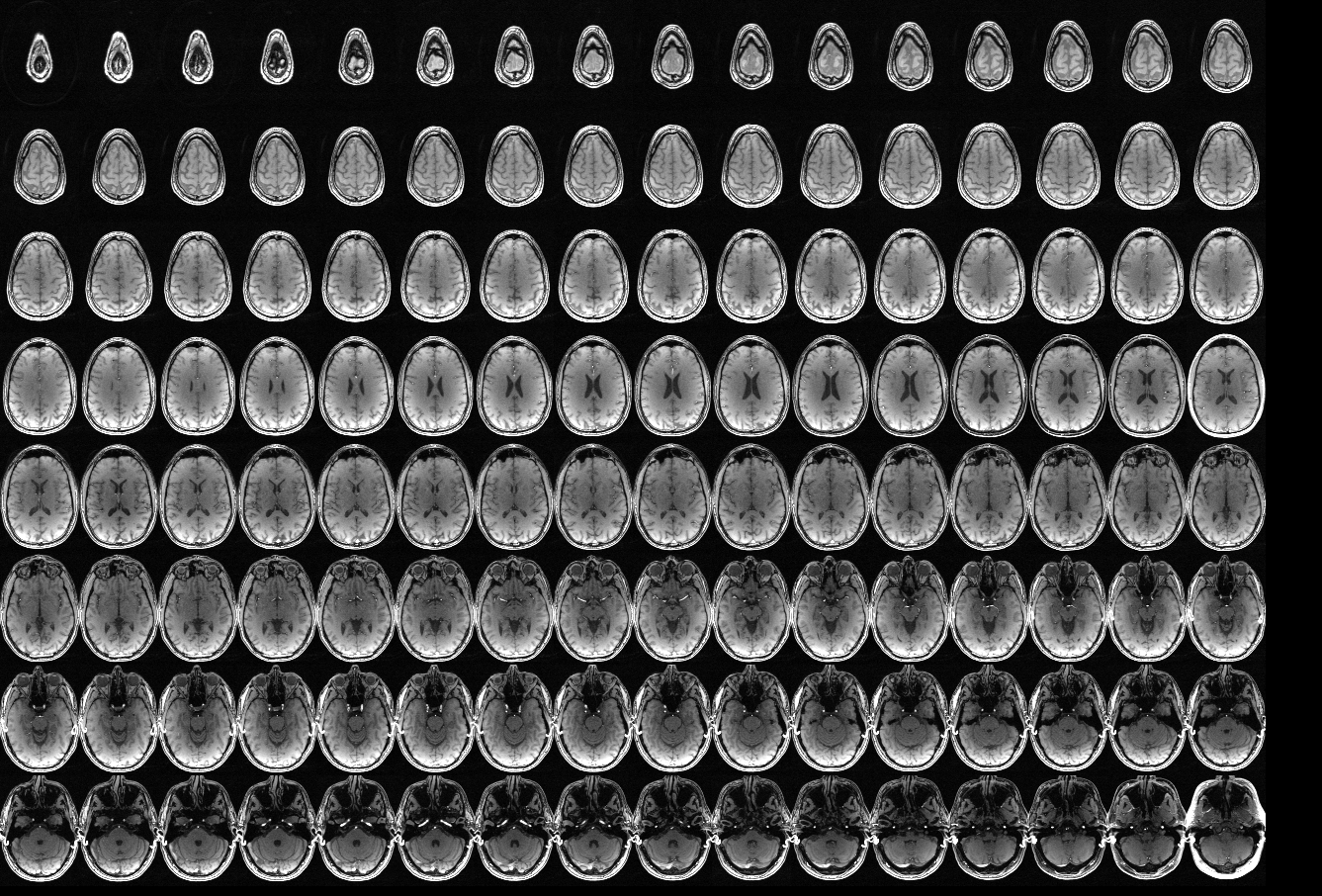
The total acquisition time (involving full k-space sampling) was approximately 6 minutes. SAR deposition was approximately 50% of the limit for the subject’s height and weight. The images display clear T1 (Figure 2) and T2 contrast (Figure 3) between gray matter, white matter, and CSF. Slab boundary artifacts were minimal. However, the SNR/CNR was adversely affected by the sub-optimal long T2 echo train and lack of inversion recovery contrast for the T1 echo train.Discussion
We here demonstrate proof-of-concept for the prequence as shown by simultaneous T1 and T2 image acquisition. The actual SNR of the sequence may be significantly improved via further optimization, as acquisition of the entire ky space in a single pulse train of length > 1.1 s is suboptimal, and inversion pulses may be added to improve T1 contrast. The acquisition time for a full sampling of k-space is approximately equal to the typical time for either a T1 MP-RAGE or T2 FSE acquisition with SENSE/GRAPPA factor of 2. Using SENSE factor = 2, it would therefore be possible to acquire a T1/T2 acquisition in 4X less time than using standard clinical product sequences.Magnetic Resonance Fingerprinting (MRF) is an alternative approach4 which provides simultaneous T1 and T2 contrasts, synthesized from estimation of T1 and T2 parameter values. The prequence approach is not aimed at estimating parameter value estimates, but only providing suitable contrast images for clinical diagnoses, and we expect the fully-optimized prequence to be able to perform this in a fraction of the time of a 3-D MRF scan. The prequence also can, if desired incorporate a balanced steady-state free precession (bSSFP) acquisition as is done in the MRF approach.
The prequence approach may include other contrasts (e.g. ASL perfusion, DWI, etc.) as part of the protocol. The goal is to provide all desired contrasts for clinical diagnoses for various protocols (e.g. headache, epilepsy, etc.) in under 15 minutes total scanning time. A multi-contrast EPI scanning sequence has been proposed5; however, it suffers from insufficient resolution for many clinical applications in addition to susceptibility artifacts. The “prequence” approach is not exclusive to neuro exams, and other MRI exams such as musculoskeletal, cardiac, and abdominal may also benefit from this time-saving technique.
Conclusion
A multi-contrast “prequence” approach to MRI pulse design has been proposed in order to reduce “dead time” and acquire all needed contrasts in a reduced total exam time. Proof of concept is demonstrated via a T1/T2 multi-contrast neuro anatomical sequence.Acknowledgements
No acknowledgement found.References
[1] Bjur KA, Payne ET, Nemergut ME, Hu D, Flick R. Anesthetic-related Neurotoxicity and Neuroimaging in Children: a Call for Conversation. J Child Neurol 32(6): 594-602 (2017).
[2] Hargreaves BA, Cunningham CH, Nishimura DG, Conolly SM. Variable-Rate Selective Excitation for Rapid MRI Sequences. Magn Reson Med 52:590-597 (2004).
[3] Sled JG. Modelling and interpretation of magnetization transfer imaging in the brain. Neuroimage 182: 128-135 (2018).
[4] Ma D, Gulani V, Seiberlich N, Liu K, Sunshine JL, Duerk JL, Griswold MA. Magnetic Resonance Fingerprinting. Nature 495(7440): 187-192 (2013).
[5] Ryu KH, Baek HJ, Skare S, Moon JI, Choi BH, Park SE, Ha JY, Kim TB, Hwang MJ, Sprenger T. Clinical Experience of 1-Minute Brain MRI Using a MultiContrast EPI Sequence in a Different Scan Environment. AJNR 4193): 424-429 (2020).
Figures