1775
Breath-hold 3D MRCP at 1.5T using Fast 3D mode and a deep learning-based noise-reduction technique1Department of Radiology, International University of Health and Welfare Mita Hospital, Tokyo, Japan, 2Department of Radiology, International University of Health and Welfare Narita Hospital, Chiba, Japan, 3Department of Radiology, The Institute of Medical Science, The University of Tokyo, Tokyo, Japan
Synopsis
The usefulness of breath-hold 3D MRCP at 3T MRI has recently been reported. Moreover, the denoising approach with deep learning-based reconstruction (dDLR) is a novel technique. We assessed the image quality of conventional respiratory-triggered 3D MRCP (Resp) and breath-hold 3D MRCP using Fast 3D mode without and with dDLR (BH, dDLR-BH) at 1.5T, by comparing the overall image quality and duct visibility scores. Breath-hold 3D MRCP compared favorably with respiratory-triggered MRCP at 1.5T. dDLR can improve the overall image quality and duct visibility of breath-hold 3D MRCP, and the visibility of the right and left hepatic ducts was improved statistically.
Introduction
Magnetic resonance cholangiopancreatography (MRCP) is a standard imaging technique that provides anatomical information on the pancreatic duct and biliary tract. Although MRCP was initially performed using 2D techniques, 3D MRCP using turbo spin echo in a navigator or respiratory-triggered manner is currently used for detailed evaluation of pancreatic and biliary disease clinically.1 Regarding its long acquisition time, several reports have highlighted the usefulness of breath-hold 3D MRCP at 3T MRI performed during a single breath-hold;2-4 however, the image quality generally decreases with the imaging time based on basic MRI principles, especially on 1.5T scanners. Recently, deep-learning techniques for reducing image noise and artifacts have been applied to imaging diagnosis. In particular, a denoising approach with deep learning-based reconstruction (dDLR) is expected to reduce noise while maintaining image contrast.5 We hypothesized that breath-hold 3D MRCP at 1.5T MRI with dDLR would provide higher-quality images and improve the diagnostic performance. This study assessed the image quality of conventional respiratory-triggered 3D MRCP (Resp) and breath-hold 3D MRCP using the newly developed Fast 3D mode without and with dDLR (BH, dDLR-BH) at 1.5T MRI.Materials and Methods
This study was approved by our Institutional Review Board.Subjects and MR examination
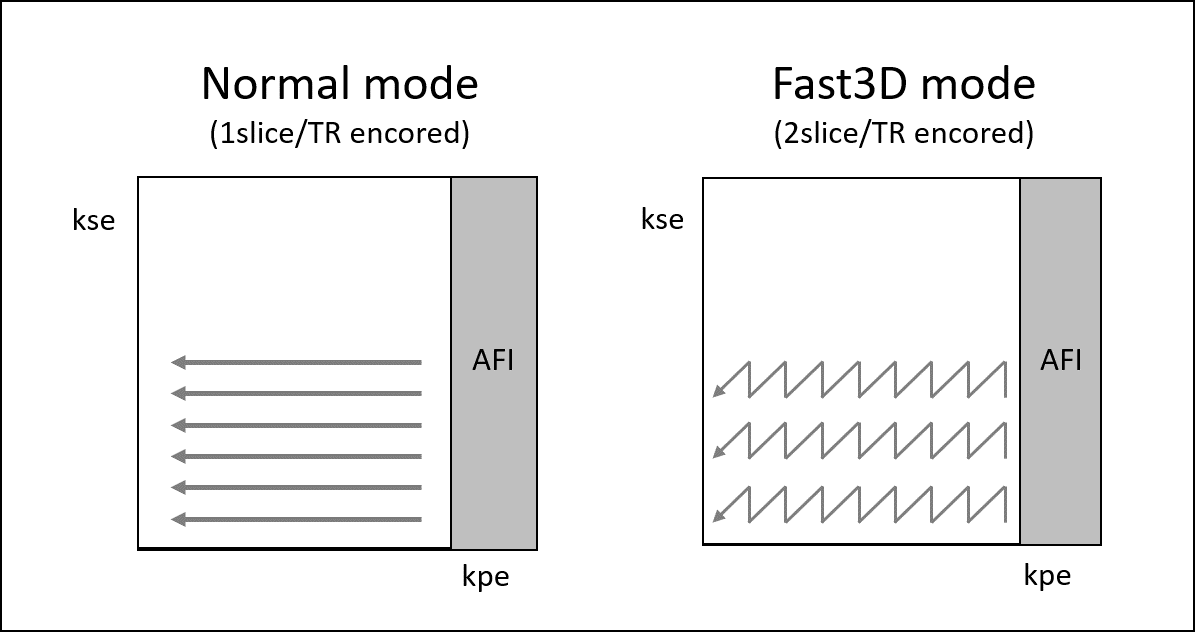
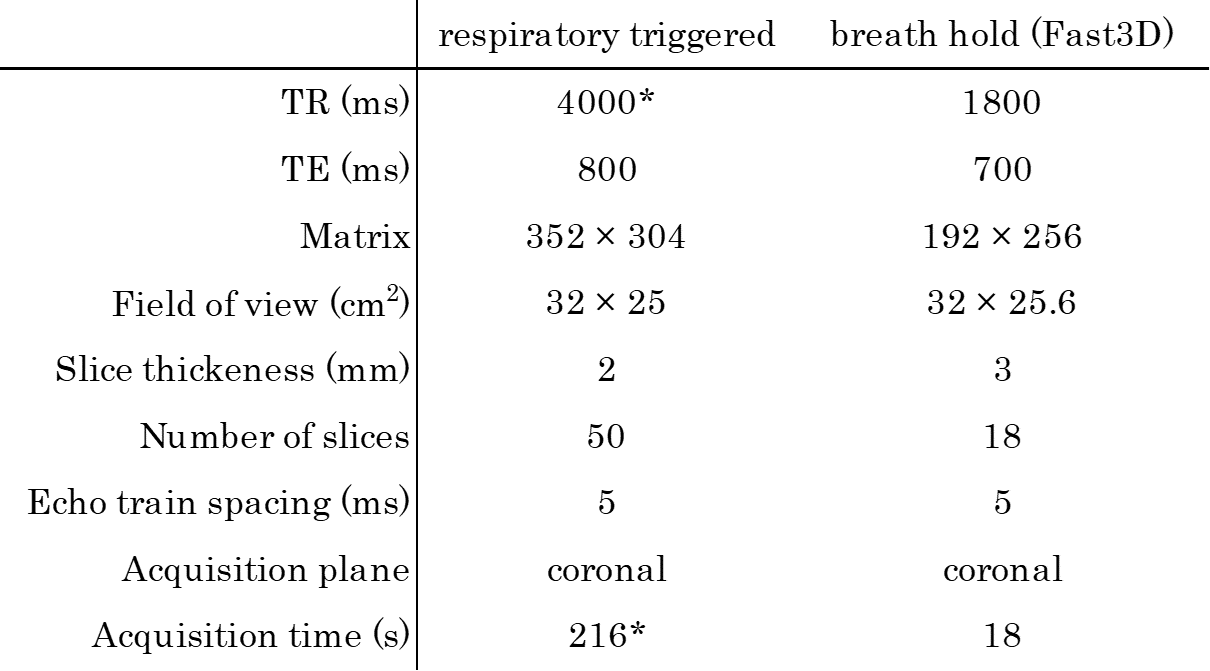
Eight patients (six men, two women; mean age, 58.5 years; age range, 43-89 years) who underwent MRCP examination for suspected pancreaticobiliary disease in a 1.5T machine (Vantage Orian 1.5T, Canon Medical Systems) were enrolled prospectively. The imaging sequences obtained were respiratory-triggered 3D MRCP (Resp) and breath-hold 3D MRCP using Fast 3D mode (BH). Fast 3D mode is a novel rapid imaging technique that enables multislice-encoding within a single repetition time (Figure 1). The combination of this technique and asymmetric Fourier imaging enables quicker image acquisition without reducing image quality. Table 1 gives the details of the imaging parameters.
dDLR technique
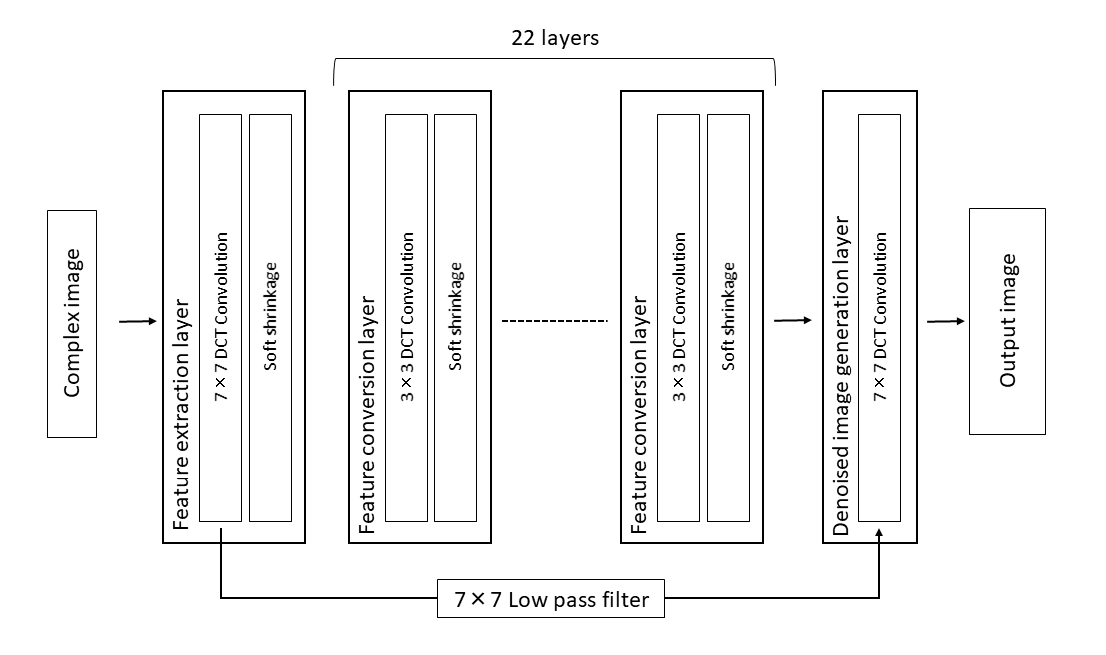
The convolution algorithm of the dDLR method used here uses a 7×7 discrete cosine transform to divide the image data into feature-extraction and zero-frequency- component paths. Separation of the zero-frequency component from the feature-extraction path maintains image contrast. Figure 2 outlines the algorithm. The BH images were further processed with dDLR, which gave noise-removed BH images (dDLR-BH).
Qualitative image analysis
Two radiologists with more than 10 years of experience each in abdominal radiology reviewed coronal source images and reconstructed maximum intensity projections (MIPs) of all subjects in consensus. The overall quality of the pancreaticobiliary tree images was scored on a 5-point scale from 1 (poor) to 5 (excellent). The visibility of the main pancreatic (MPD), common bile (CBD), right hepatic (RHD), left hepatic (LHD), and cystic (CD) ducts was scored on a 5-point scale where 1 = ductal structure not detectable, 2 = ductal structure only partially visible, 3 = most of the ductal structure visible, 4 = ductal structure entirely visible with slight artifact, and 5 = ductal structure perfectly visible with no detectable artifact. Additional 2D MRCP MIP images were used as an anatomical reference. All images were anonymized and shown to the reviewers in random order, and the information of the acquisition method was blinded to the radiologists during image analysis.
Statistical analysis
To assess the effect of denoising with deep learning-based reconstruction, we compared the overall image quality and duct visibility scores of BH and dDLR-BH using the Wilcoxon signed-rank test. P <0.05 was considered statistically significant.
Results
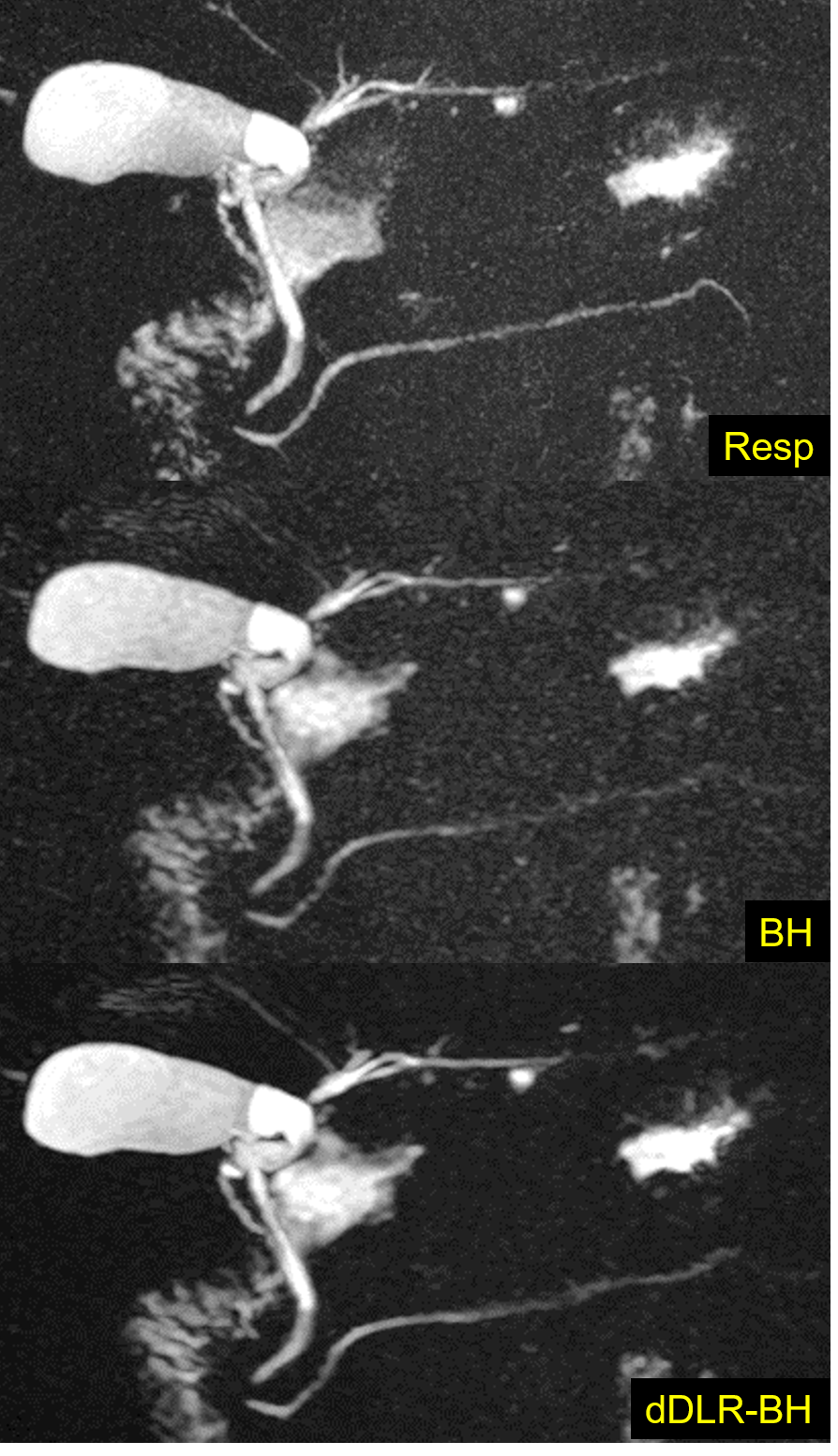
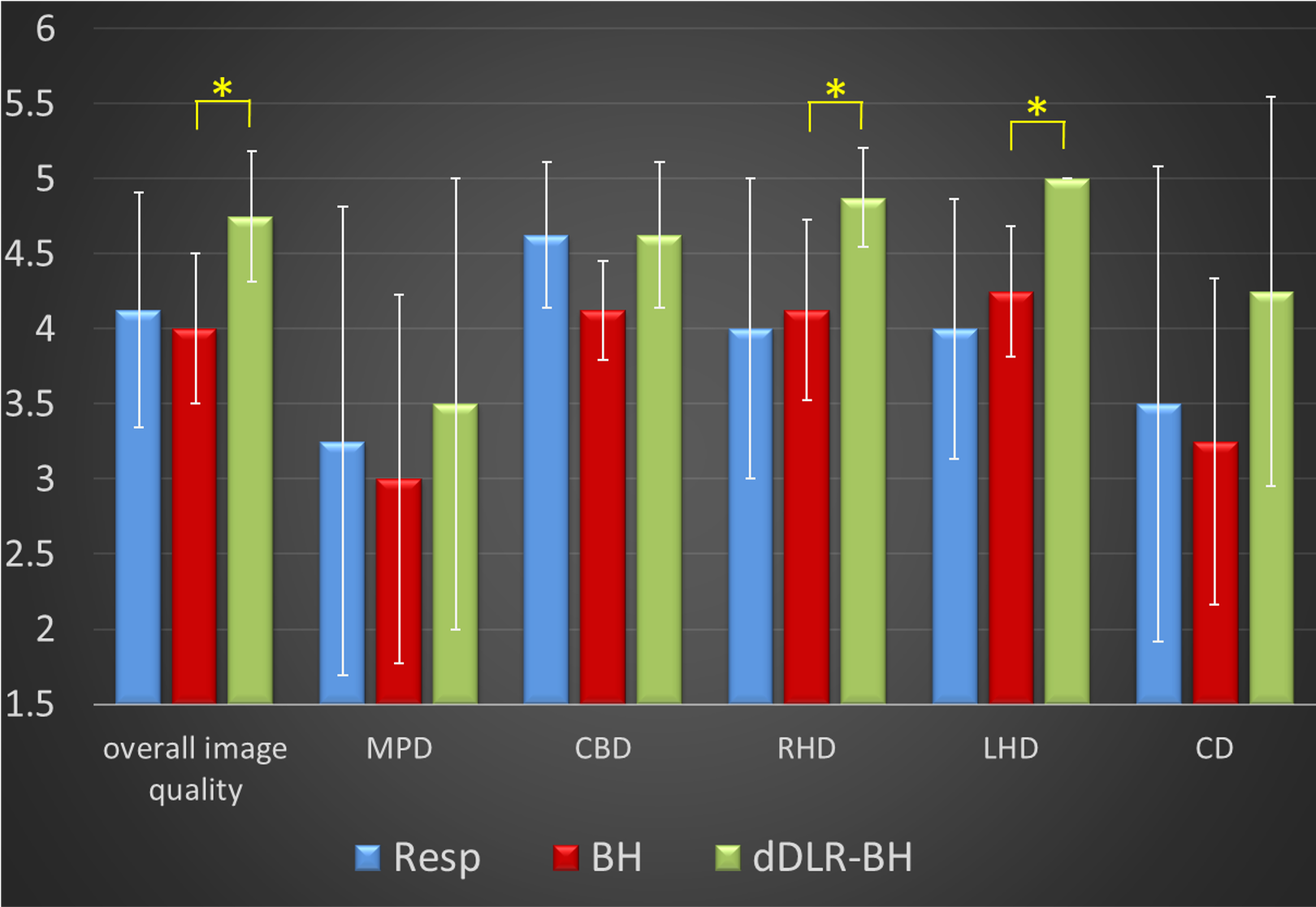
Figure 3 shows representative MRCP images. Figure 4 shows the mean scores for overall image quality and duct visibility. All values are expressed as the mean ± standard deviation (SD). The mean scores of dDLR-BH tended to be higher than Resp and BH, while the mean BH scores were almost equivalent to Resp. The dDLR-BH scores for overall image quality, RHD, and LHD were significantly higher than BH (P = 0.0477, 0.0197, and 0.0197, respectively).Discussion
The mean dDLR-BH scores tended to be higher than those of BH, and significant differences were detected for the overall image quality, RHD, and LHD scores. A denoising approach to MRCP improves global image quality, and may improve the visibility of relatively small biliary tracts.The mean overall image quality scores of Resp and BH were both approximately 4 (good). Therefore, breath-hold 3D MRCP using Fast 3D mode provides almost equivalent image quality to conventional respiratory-gated 3D MRCP at 1.5T. Breath-hold MRCP is useful clinically because of the shorter acquisition time. These findings are similar to those reported at 3T MRI.
Nevertheless, the duct visibility scores of MPD were relatively low in all groups. A possible reason is that several patients had a non-dilated, normal main pancreatic duct barely visible on MRCP.
Conclusion
Breath-hold 3D MRCP using Fast 3D mode and a denoising approach with deep learning-based reconstruction is useful for rapid image acquisition and improving the image quality of MRCP at 1.5T.Acknowledgements
None.References
1. Yoon, J. H., Nickel, M. D., Peeters, J. M. & Lee, J. M. Rapid imaging: Recent advances in abdominal MRI for reducing acquisition time and its clinical applications. Korean J. Radiol. 2019;20(12):1597–1615.
2. Tokoro, H. et al. Usefulness of breath-hold compressed sensing accelerated three-dimensional magnetic resonance cholangiopancreatography (MRCP) added to respiratory-gating conventional MRCP. Eur. J. Radiol. 2020;122:108765.
3. Song, J. S., Kim, S. H., Kuehn, B. & Paek, M. Y. Optimized Breath-Hold Compressed-Sensing 3D MR Cholangiopancreatography at 3T: Image Quality Analysis and Clinical Feasibility Assessment. Diagnostics 2020;10(6):376.
4. Chen, Z. et al. Three-dimensional breath-hold MRCP using SPACE pulse sequence at 3 T: Comparison with conventional navigator-triggered technique. Am. J. Roentgenol. 2019;213(6):1247–1252.
5. Shinoda, K. et al. Deep Learning Based Adaptive Noise Reduction in Multi-Contrast MR Images. ISMRM 2019 #4701.
Figures