1686
Altered global functional network connectivity and its relationship to cognitive dysfunction in rheumatoid arthritis1Peking Union Medical College Hospital, Beijing, China
Synopsis
Patients with rheumatoid arthritis (RA), a systemic autoimmune disease, had cognitive dysfunction. Resting-state functional MRI wasutilized to explore the whole-brain functional network connectivity in RA patients. The whole-brain functional connectivity strength in RA patients was altered and significantly correlated to cognitive performance.
INTRODUCTION
Rheumatoid arthritis (RA) is a systemic autoimmune disease primarily involves synovitis, which affects about 0.5-1% of the population[1]. Recent studies suggest that the prevalence of cognitive dysfunction in RA patients ranges from 30% to 50%[2-4]. However, it has not been clearly demonstrated so far that whether the whole-brain functional network connectivity is altered in RA. Therefore, the alterations of the whole-brain functional network connectivity in RA were investigated by functional connectivity strength (FCS). Further, its relation to cognitive dysfunction was examined to uncover the neuropathological mechanisms of cognitive dysfunction in RA.METHODS
Thirty RA patients fulfilling the 2010 ACR/EULAR classification criteria[5] and Thirty sex/age matched healthy controls (HC) were enrolled in the study. All the subjects underwent neuropsychological assessments, such as mini-mental state examination (MMSE) and Montreal cognitive assessment (MoCA).MRI was performed in all the patients on a 3.0 Tesla MR scanner with an 8-channel HEAD coil. Resting-state functional MRI (rs-fMRI) was acquired with EPI sequence (TR = 2000 ms, TE = 30 ms, FOV = 24 cm × 24 cm, matrix = 64 × 64, slice thickness = 4 mm, gap = 0, 36 slices, 240 phases). Structural T1 imaging was performed with BRAVO for normalization, an optimized 3D fast spoiled gradient echo sequence (1 mm × 1 mm × 1 mm isotropic, Prep Time = 400ms, flip angle = 12°, bandwidth = 27.78 Hz). Other conventional series such as T2WI, T2-FLAIR, DWI, SWI and MRA were acquired to exclude any brain abnormality. All images were reviewed to ensure imaging quality.The whole-brain FCS was established by calculating the sum of the connections for each voxel to capture its global functional integrity. The correlation between FCS and neuropsychological characteristics was further analyzed.RESULTS
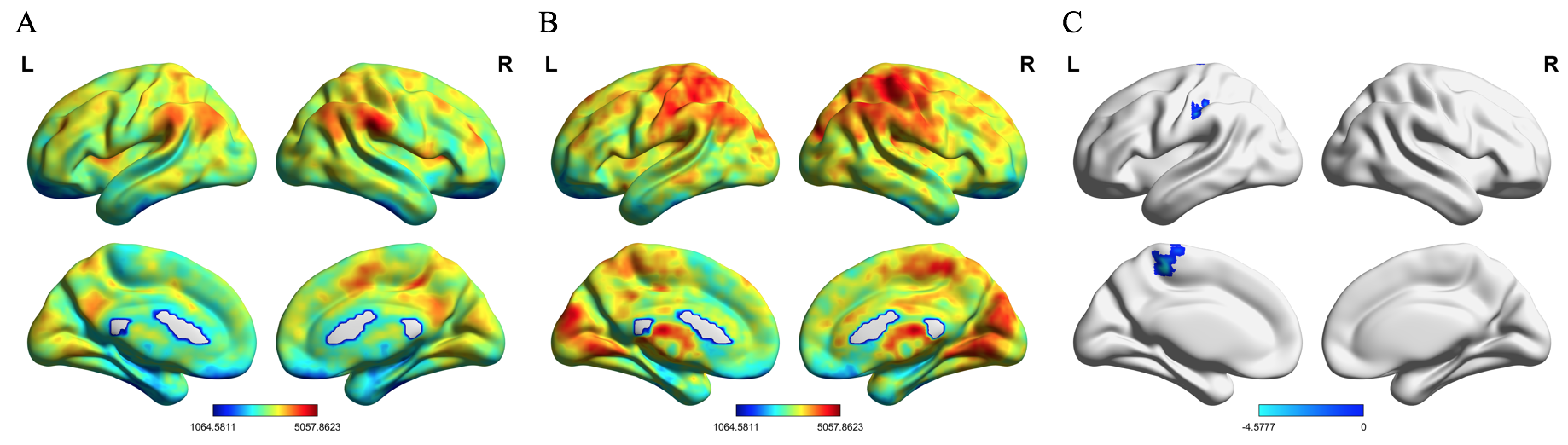
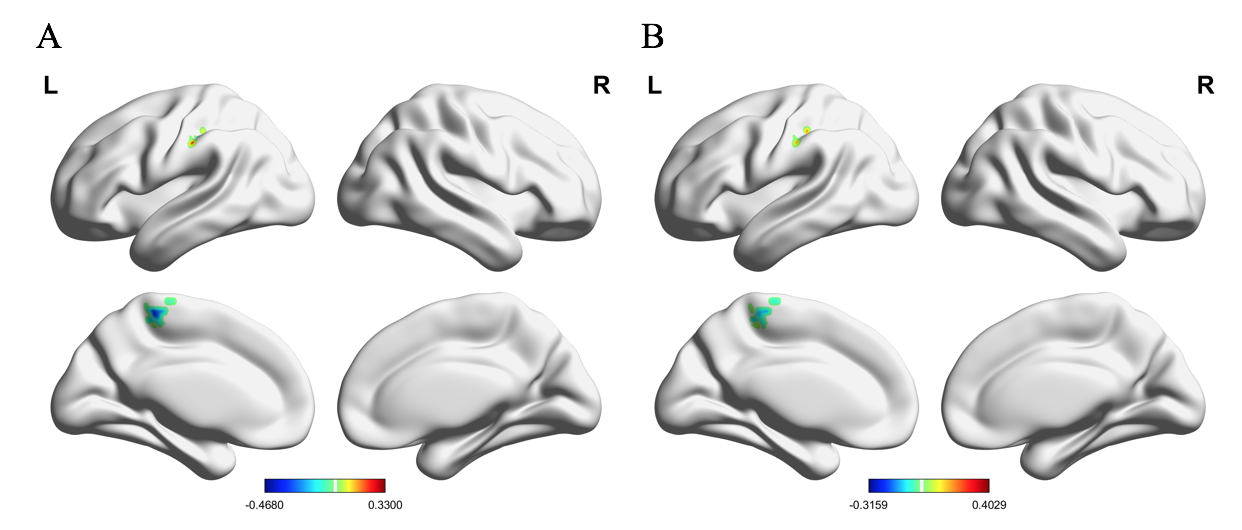
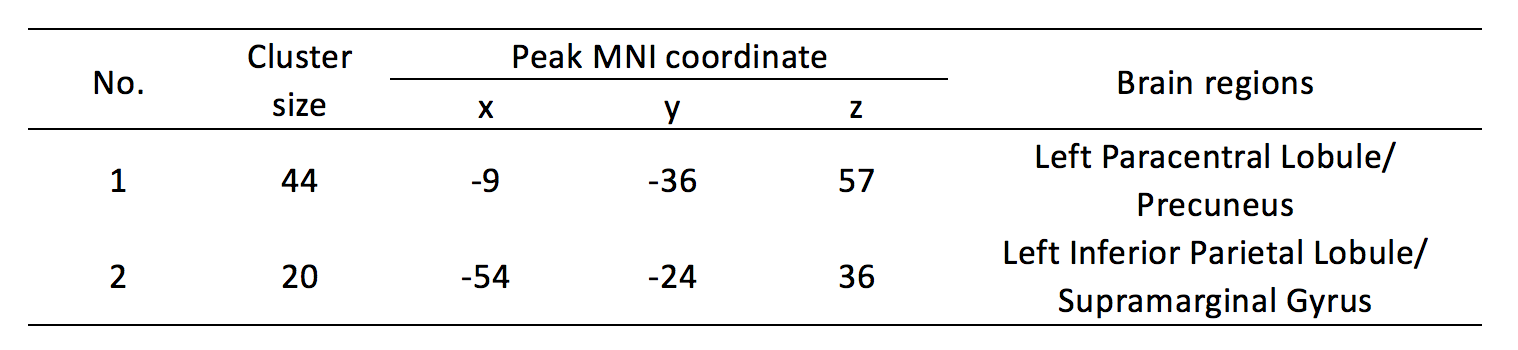
Figure 1 showed the FCS in RA, HC and the difference between RA and HC. Compared with HC, RA patients showed decreased FCS predominantly in left paracentral lobule and precuneus (Table 1). The FCS of the left inferior parietal lobule/ supramarginal gyrus was significant positive correlated to MMSE (Figure 2A). Significant negative correlation was found between the FCS of the left paracentral lobule/precuneus and MMSE (Figure 2A). the correlation MMSE was similar to MoCA (Figure 2B).DISCUSSION
This study demonstrated the altered FCS in RA patients using rs-fMRI. The decreased FCS was correlated to worsening performance in MMSE and MoCA. The increased FCS of the left inferior parietal lobule/supramarginal gyrus in RA may partially compensate for cognitive dysfunction in RA.CONCLUSION
Patients with rheumatoid arthritis (RA), a systemic autoimmune disease, had cognitive dysfunction. Resting-state functional MRI was utilized to explore the whole-brain functional network connectivity in RA patients. The whole-brain functional connectivity strength in RA patients was altered and significantly correlated to cognitive performance.Acknowledgements
No acknowledgement found.References
[1] Scott D L, Wolfe F, Huizinga T W. Rheumatoid arthritis[J]. Lancet, 2010, 376(9746): 1094-1108.
[2] Bartolini M, Candela M, Brugni M, et al. Are behaviour and motor performances of rheumatoid arthritis patients influenced by subclinical cognitive impairments? A clinical and neuroimaging study[J]. Clin Exp Rheumatol, 2002, 20(4): 491-497.
[3] Appenzeller S, Bertolo M B, Costallat L T. Cognitive impairment in rheumatoid arthritis[J]. Methods Find Exp Clin Pharmacol, 2004, 26(5): 339-343.
[4] Shin S Y, Julian L, Katz P. The relationship between cognitive function and physical function in rheumatoid arthritis[J]. J Rheumatol, 2013, 40(3): 236-243.
[5] Aletaha D, Neogi T, Silman A J, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative[J]. Ann Rheum Dis, 2010, 69(9): 1580-1588.
Figures