1672
Evaluation of White Matter Integrity via Fixel-Based Analysis in HIV Infection1Biomedical Engineering, University of Rochester, Rochester, NY, United States, 2Neurology, University of Rochester, Rochester, NY, United States, 3Imaging Sciences, University of Rochester, Rochester, NY, United States, 4Physics and Astronomy, University of Rochester, Rochester, NY, United States
Synopsis
Individuals with chronic HIV-infection suffer from neurocognitive impairment. These changes are thought to be mediated by atrophy and demyelination in the setting of chronic neuroinflammation. In this abstract, we used fixed-based analysis (FBA) to investigate the relationship between white matter integrity and cognitive function in the presence of HIV infection. Connectivity-based fixel ehancement and region-based statistics were performed to evaluate group differences at the fixel and tract level, respectively. Lower fixel-based metrics were observed in the HIV+ cohort. We also observed significant correlations between fixel-based metrics and cognitive scores derived from neuropsychological testing in the HIV+ cohort.
Purpose
Individuals with chronic HIV-infection suffer from neurocognitive impairment1,2. Inflammation and infection within the central nervous system is thought to compromise white matter (WM) integrity3. Previous studies have shown that imaging metrics derived from diffusion tensor imaging (DTI) are correlated with markers of blood brain barrier breakdown and the duration of HIV-infection4-6. Recently, fixel-based analysis (FBA) has emerged as tool to study WM integrity at the sub voxel scale7. FBA can resolve multiple fiber populations within a given voxel and helps elucidate pathological differences that cannot be resolved at the voxel level. Here we investigate WM integrity using FBA comparing HIV-infected and HIV-uninfected individuals. Additionally, we evaluate the relationship between FBA metrics and cognitive performance.Methods
As part of an ongoing study, 94 age-matched subjects [HIV+: N=42, M/F=40/2, age=34 ± 12.9; HIV-: 52, M/F 26/26, age = 37.13 ± 11.9) were evaluated. All subjects underwent comprehensive neurocognitive assessment and brain MRI. Cognitive domains evaluated included executive function, attention, memory, learning, speed of information processing, verbal reasoning and motor speed. A total summary Z score was calculated by summing all cognitive domain Z-score. All imaging was conducted on a 3T scanner (MAGNETOM Trio, Siemens, Erlangen, Germany) equipped with a 32-channel head coil. The T1-weighted images were acquired using a 3D MPRAGE sequence (TI = 1,100 ms, TR/TE = 2,530/3.44 ms; flip angle = 7˚; FOV = 256×256; voxel size = 1.0×1.0×1.0 mm3). Diffusion weighted images were acquired using a single shot SE-EPI sequence (60 diffusion-encoded images (b=1000 s/mm2), 10 non-diffusion weighted reference images (b=0 s/mm2); TR/TE = 8,900/ 86 ms; FOV = 256×256; voxel size = 2.0×2.0×2.0 mm3). In order to correct for EPI distortions, a double-echo gradient echo field map was also acquired.Preprocessing of diffusion images included susceptibility and eddy-current distortion correction. FBA was performed using the recommended pipeline7 in MRtrix38 (version 3.0.2). Briefly, the fiber orientation distribution (FOD) within each voxel was estimated using multi-tissue constrained spherical deconvolution9. A study-specific template was then created by spatial normalization of subjects using symmetric diffeomorphic non-linear transformation FOD-based registration10. One group-averaged FOD template, including 20 HIV-infected and 20 HIV-uninfected subjects , was generated for group comparisons. Fixel specific measures of fiber density (FD) and fiber bundle cross-section (FC) were calculated within each voxel. A combined measure, FDC, was also generated by multiplying FD and FC. Modified fixel-based metrics were also calculated for the major bundles using the Johns Hopkins (JHU) DTI-based white matter atlas.
Statistical analyses were performed using MRtrix3. Non-parametric permutation testing and connectivity based fixel enhancement11 (CFE) were used to identify significant differences in fixel-based metrics, using age and sex as covariates. Group comparisons were performed using a linear regression model with age as a covariate. Statistical analysis of demographic data and region-specific metrics were performed in R12. All p-values were adjusted for multiple comparisons using Benjamini-Hochberg.
Results
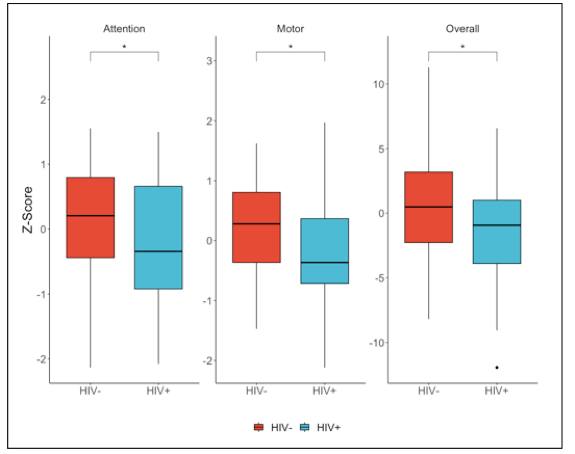
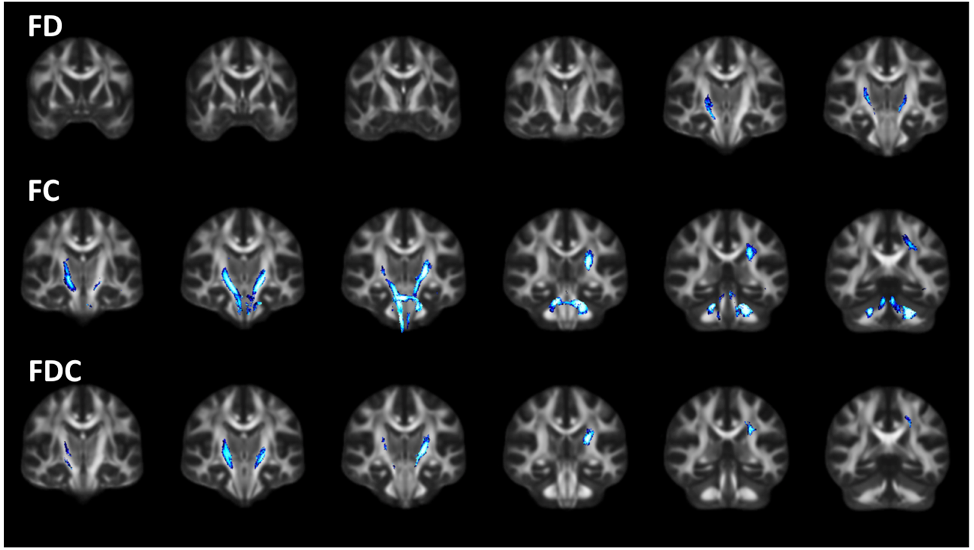
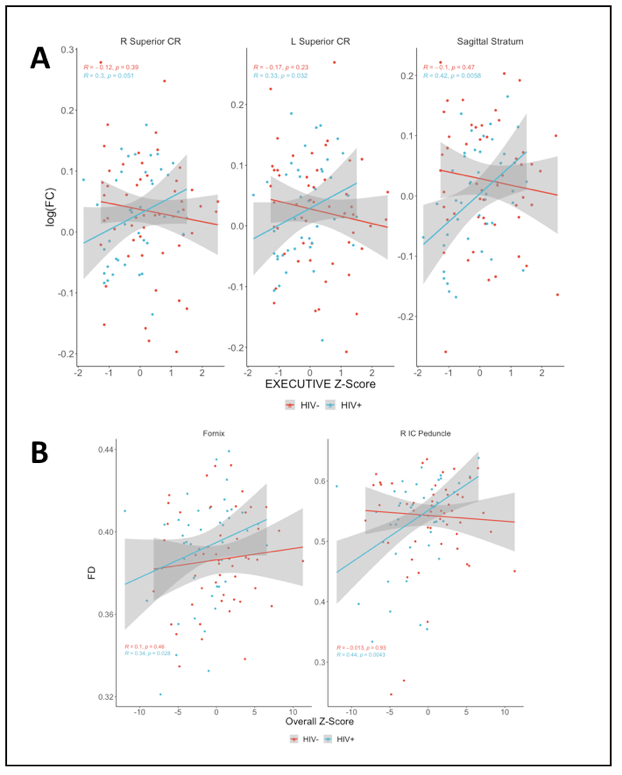
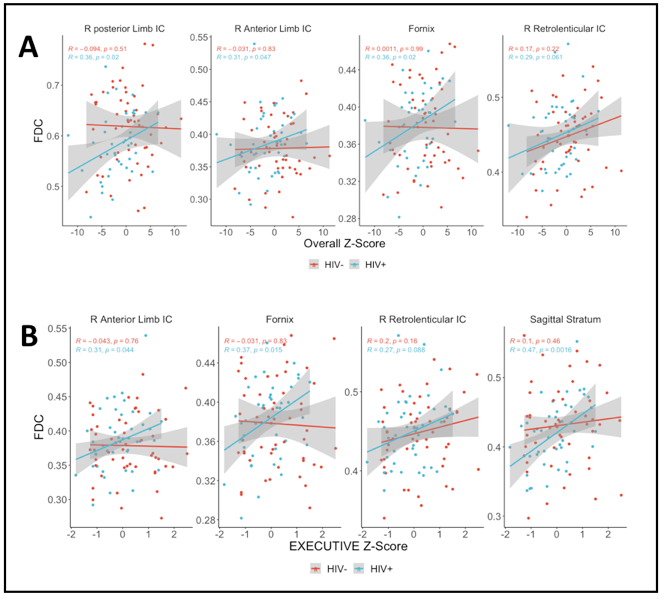
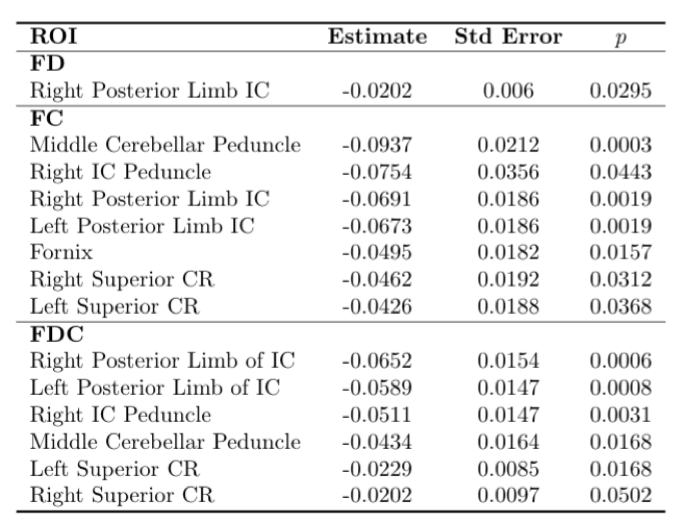
Worse scores (negative Z scores) for attention, memory and overall cognitive summary score were observed in the HIV+ group compared to controls (Figure 1). Figure 2 shows significant differences (family wise error-corrected p < 0.05) for each fixel-based metrics between HIV+ and HIV- individuals. Reductions in FC are most pronounced in the posterior limb of the internal capsule. Figure 3A shows marginal correlations between log(FC) and the executive score. Figure 3B shows marginal correlations between FD and the cognitive summary score. In all cases, the correlation between cognitive score and imaging metrics were significant for HIV+ individuals but not for HIV-, and exhibited a positive correlation. Figure 4 illustrates a similar relationship between FDC and the cognitive summary score, and the executive score. Again, significant positive correlations between cognitive score and FDC was only seen in the HIV+ cohort. Table 1 shows the results of a multivariate regression model for specific ROIs. For all significant ROIs the average difference for HIV+ is lower than that for HIV-.Discussion
Here we showed that fixel based metrics are consistently lower in HIV-infected individuals, which we previously did not observe using voxel-based metrics13. These reduced fixel metrics suggest less efficient information transfer in the setting of HIV-infection, possibly due to atrophy and demyelination triggered by neuroinflammation. We also showed that fixel based metrics are correlated with the cognitive summary and executive scores. These findings suggest that white matter integrity, as measured using FBA is reflective of cognitive changes in HIV. Accordingly, fixel based metrics may serve as an in vivo substrate marker of brain injury.Conclusion
In this preliminary analysis we show that fixel based metrics are sensitive to changes between HIV+ and HIV- individuals. Additionally, we showed that in HIV+ individuals these metrics are correlated with cognitive measures. Future studies will look at longitudinal changes to evaluate how WM integrity is affected in the setting of chronic HIV-infection.Acknowledgements
This study was supported by the NIH grant R01-MH099921References
1. Clifford DB, Ances BM. HIV-associated neurocognitive disorder. Lancet Infect Dis. 2013;13(11):976-986.
2. Anand P, Springer SA, Copenhaver MM, Altice FL. Neurocognitive impairment and HIV risk factors: a reciprocal relationship. AIDS Behav. 2010;14(6):1213-1226.
3. Alakkas A, Ellis RJ, Watson CW, et al. White matter damage, neuroinflammation, and neuronal integrity in HAND. J Neurovirol. 2019;25(1):32-41.
4. Wright PW, Vaida FF, Fernandez RJ, et al. Cerebral white matter integrity during primary HIV infection. AIDS. 2015;29(4):433-442.
5. Atluri VS, Hidalgo M, Samikkannu T, et al. Effect of human immunodeficiency virus on blood-brain barrier integrity and function: an update. Front Cell Neurosci. 2015;9:212.
6. Resnick L, Berger JR, Shapshak P, Tourtellotte WW. Early penetration of the blood-brain-barrier by HIV. Neurology. 1988;38(1):9-14.
7. Raffelt DA, Tournier JD, Smith RE, et al. Investigating white matter fibre density and morphology using fixel-based analysis. Neuroimage. 2017;144(Pt A):58-73.
8. Tournier JD, Smith R, Raffelt D, et al. MRtrix3: A fast, flexible and open software framework for medical image processing and visualisation. Neuroimage. 2019;202:116137.
9. Jeurissen B, Tournier JD, Dhollander T, Connelly A, Sijbers J. Multi-tissue constrained spherical deconvolution for improved analysis of multi-shell diffusion MRI data. Neuroimage. 2014;103:411-426.
10. Raffelt D, Tournier JD, Fripp J, Crozier S, Connelly A, Salvado O. Symmetric diffeomorphic registration of fibre orientation distributions. Neuroimage. 2011;56(3):1171-1180.
11. Raffelt DA, Smith RE, Ridgway GR, et al. Connectivity-based fixel enhancement: Whole-brain statistical analysis of diffusion MRI measures in the presence of crossing fibres. Neuroimage. 2015;117:40-55.
12. R Core Team (2020). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria.
13. Zhuang Y, Qiu X, Wang L, et al. Combination antiretroviral therapy improves cognitive performance and functional connectivity in treatment-naive HIV-infected individuals. J Neurovirol. 2017;23(5):704-712.
Figures