1650
Clinical feasibility study of extracranial carotid arteries magnetic resonance angiography using PETRA-MRA1XIAN DAXING HOSPITAL, Xi'an, China, 2MR Scientific Marketing, Siemens Healthineers, Xi'an, China
Synopsis
Magnetic resonance angiography (MRA) is increasingly used as a non-invasive method to assess carotid arteries. TOF-MRA, because it is dependent on the flow of magnetized blood into the volume being imaged, is highly susceptible to conditions that disrupt laminar flow. Depiction of the carotid region using Silent imaging was often superior to that obtained with conventional techniques, where the ultrashort TE minimized flow-related signal dropout. This study aimed to evaluate the feasibility of PETRA-MRA in imaging the vascular structures of the extracranial carotid arteries. We found that PETRA-MRA showed significantly higher image quality and better visualized extracranial carotid arteries.
Introduction
Atherosclerosis affecting the cervical internal carotid artery (ICA) is an important cause of cerebral infarction, being responsible for 10% to 20% of cases of ischemic stroke[1]. TOF-MRA is a nonenhanced MRA technique which relies on the movement of magnetized blood through the volume being imaged. TOF-MRA is susceptible to degradation by turbulence and slow flow, which disrupt the smooth linear flow of blood through the vessel itself. Pointwise encoding time reduction with radial acquisition (PETRA)-MRA is a silent imaging method which using ultrashort TE technique, has good signal homogeneity , good signal to noise ratio (SNR), fewer susceptibility artifacts, and less acoustic noise[2-3]. Based on those intrinsic principles of PETRA sequence, our study aimed to evaluate and compare the imaging ability about extracranial carotid arteries vascular structure using PETRA-MRA and TOF-MRA.Subjects and methods
Twenty-six healthy participants (13 male, 13 female; mean age, 37 years; age range, 24–51 years) were recruited in this study. All the subjects underwent 3D-TOF-MRA and PETRA-MRA examination on a 3 T MR scanner (Magnetom Prisma, Siemens Healthcare, Erlangen, Germany) with a 64ch head-neck coil . 3D-TOF-MRA was performed in an axial orientation with the following parameters: repetition time (TR)/echo time (TE) = 20.00/3.60ms, flip angle = 18°,field of view (FOV) = 189 × 320 mm2, bandwidth = 279Hz/Px, slice thickness = 0.75 mm, slabs = 9, slices per slab = 44,acquired voxel size = 0.78 × 0.63 × 1.50 mm3 and acquisition time (TA) = 5 min 52 s, flow compensation was applied. PETRA-MRA was performed in the coronary orientation with the parameters as follows: TR/TE = 5.00/0.07ms, flip angle = 6°, FOV = 320 × 320 mm2, bandwidth = 395 Hz/Px, slice thickness = 0.91mm, slab = 1, slices per slab = 352, acquired voxel size = 0.91 × 0.91 × 0.91mm3 and radial views number = 66,000. As PETRA-MRA was subtracted from two imaging datasets with and without the slice-selective saturation slab, scanning time for PETRA-MRA was 5 min 51 s about data without the saturation band and 8 min 30 s about data with the saturation band, which was placed at the bottom of the imaging volume. Statistical analysis was performed using SPSS software (version 19.0, IBM Corp., Armonk, NY, USA). The measurement data were expressed as mean ± standard deviation (SD). The statistical differences in the subjective image quality scores between PETRA-MRA and 3D-TOF-MRA were analyzed and compared using the Wilcoxon signed rank test. The paired t-test was applied to analyze differences in SNR and CNR. P < 0.05 was considered statistically significant. Interobserver agreement was assessed by calculating the Cohen kappa statistic. The original source images and MIP images were all reviewed by two radiologists who assessed image quality affected by flow dephasing artifacts in the extracranial carotid arteries segments by using a 4-point scale[4]: 1, no signal loss; 2, mild signal loss; 3, moderate signal loss that could meet diagnostic demand; and 4, severe signal loss that could not meet the diagnostic requirement. Meanwhile signal-to-noise ratio (SNR, SNR=SIArtery/SDAir) and contrast-to-noise-ratio (CNR, CNR= (SIArtery/SITissue)/SDAir) were also calculated. Inter-observer agreement between the two radiologists was assessed.Results
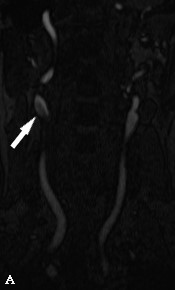
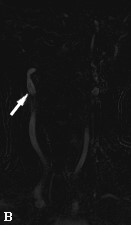
The image quality was higher in PETRA-MRA compared with 3D-TOF-MRA with significant difference (the mean scores for PETRA-MRA of readers 1, 2 were 4.82±0.44, 4.86±0.35, respectively; for 3D-TOF-MRA were 4.61±0.53, 4.51±0.58, respectively) (P < 0.01). The paired t-test showed significant variance results between 3D-TOF-MRA and PETRA-MRA. The SNRs of right CCA comparison were: (12.3±5.2) of TOF-MRA and (27.6±7.9) of PETRA-MRA (P < 0.001). The SNRs of right ICA comparison were: (26.5± 5.9) of TOF-MRA and (38±9.5) of PETRA-MRA (P < 0.001). The SNRs of right ECA comparison were: (18.9± 7.2) of TOF-MRA and (40.9±8.6) of PETRA-MRA (P < 0.001). The CNRs of right CCA comparison were: (10±4.5) of TOF-MRA and (26.8±7.3) of PETRA-MRA (P < 0.001). The CNRs of right ICA comparison were: (22.2± 7.6) of TOF-MRA and (41.7±11.5) of PETRA-MRA (P < 0.001). The CNRs of right ECA comparison were: (15.8± 6.2) of TOF-MRA and (40.3±12.6) of PETRA-MRA (P < 0.001). The SNR and CNR of both side of extracranial carotid arteries showed significantly higher in PETRA-MRA than TOF-MRA.Discussion and Conclusion
In this study we investigated the clinical feasibility of PETRA-MRA by evaluating image quality and compared that with routine 3D-TOF-MRA. We found that PETRA-MRA showed significantly higher image quality and better visualized extracranial carotid arteries. Atherosclerotic plaque formation at the carotid bifurcation can be greatly attributed to hemodynamic forces. Our study showed that the image quality of PETRA-MRA was preferable than those of TOF-MRA. From our results, PETRA-MRA techniques also can reduce the flow dephasing artifacts in the blood vessel. In conclusion, extracranial carotid arteries MRA using PETRA technique could be clinically valuable for improving the image quality with higher diagnostic performance compared with TOF-MRA. PETRA MRA is a feasible protocol in extracranial MRA imaging .Acknowledgements
We thank Shaoyu Wang of Siemens Healthcare, Ltd., Xi’an, China, for technical support.References
[1] Del Brutto VJ, Gornik HL, Rundek T. Why are we still debating criteria for carotid artery stenosis? Ann Transl Med. 2020;8(19):1270.
[2] Heo YJ, Jeong HW, Baek JW, et al. Pointwise encoding time reduction with radial acquisition with subtraction-based MRA during the follow-up of stent-assisted coil embolization of anterior circulation aneurysms. AJNR Am J Neuroradiol 2019;40:815–819.
[3] Grodzki DM, Jakob PM, Heismann B. Ultrashort echo time imaging using pointwise encoding time reduction with radial acquisition (PETRA). Magn Reson Med 2012;67:510–518.
[4] Aida N, Niwa T, Fujii Y, et al. Quiet T1-weighted pointwise encoding time reduction with radial acquisition for assessing myelination in the pediatric brain. Am J Neuroradiol 2016;37:1528–1534.
Figures