1643
Can hybrid ASL-tagged ZTE MRA be an effective candidate in the evaluation of intracranial artery diseases? A clinical feasibility study1Nanjing First Hospital, Nanjing Medical University, Nanjing, China, 2GE Healthcare, MR Research China, Beijing, China, 3Northern Jiangsu People’s Hospital, Yangzhou, China
Synopsis
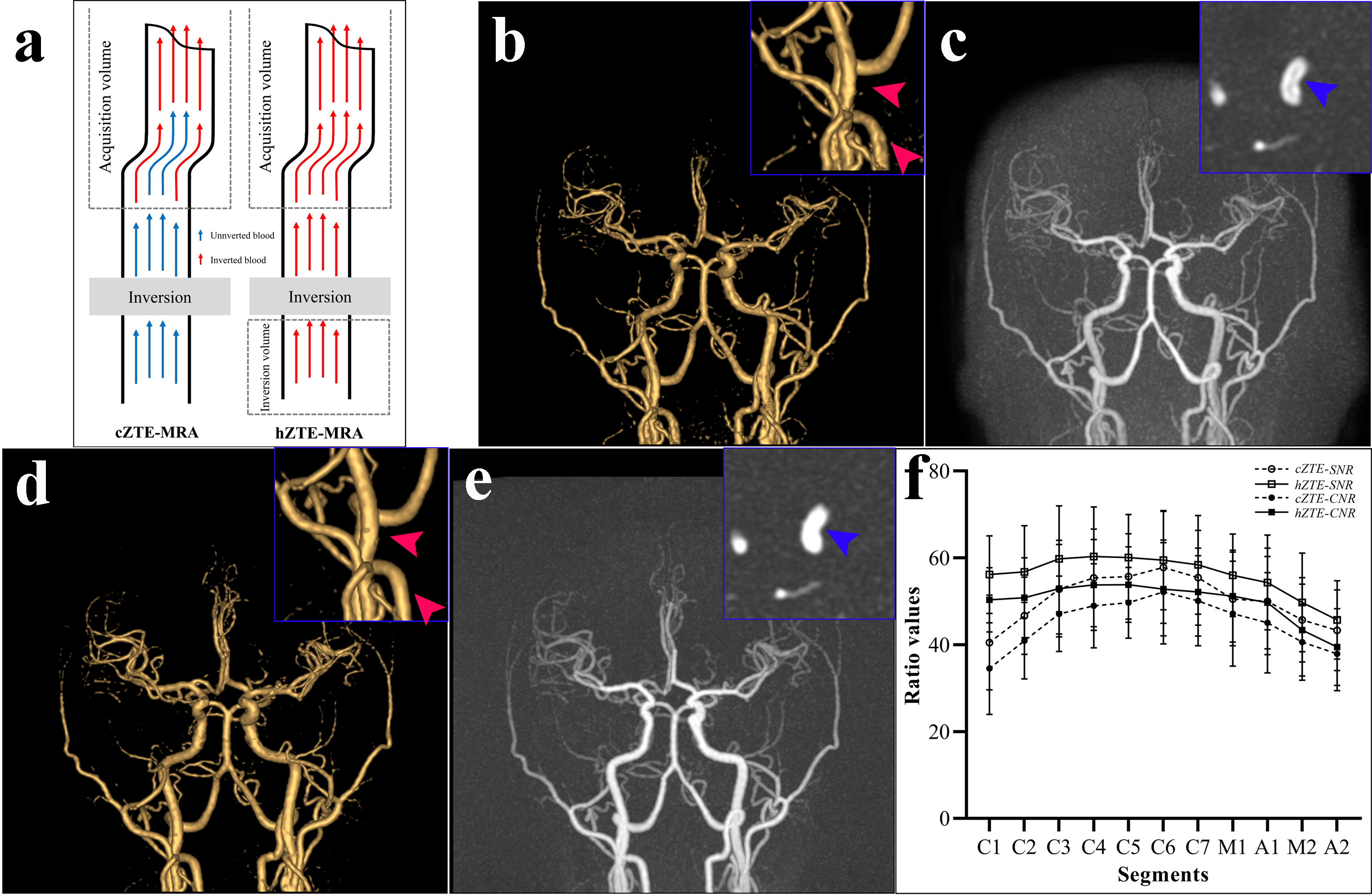
Flow related artifacts in continuous arterial spin labeling (cASL) zero-echo-time (ZTE) magnetic resonance angiography (MRA) could influence the visualization of vasculature. This study aimed to investigate the clinical feasibility of ZTE-MRA with hybrid arterial-spin-labeling (hASL) tagged for assessing the intracranial artery diseases assessment. Our clinical results indicated that relative to conventional ZTE-MRA, hASL-ZTE-MRA was more robust and superior in the depiction of intracranial artery diseases and follow-up assessment in a clinical population while maintaining a ZTE-derived nature.
Introduction
Hemodynamic information derived from magnetic resonance angiography (MRA) is essential for intracranial artery diseases diagnosis and follow-up assessment. zero-echo-time (ZTE) MRA has be demonstrated with promising superiority over time of flight MRA [1]. However, marginal blurring along the vessel walls and the presence of hollowing artifacts occurs in ZTE-MRA, which might introduce erroneous evaluation for vascular lesions or lead to a reduction in signal uniformity [2].Recently, Qu et al[3] modified ZTE-MRA with tagging hybrid arterial-spin-labeling (hASL) and described its technical potential in vessel depiction. However, no study to date has been conducted clinically to investigate the feasibility of this hASL-ZTE-MRA imaging intracranial artery diseases.
In this study, we thus aimed to implement hASL-ZTE-MRA in a clinical population, and verify the feasibility of this technique systematically for assessing various intracranial artery diseases by comparing with conventional ZTE-MRA. In addition, computed tomography angiography (CTA) imaging was also acquired and served as a reference.
Materials and Methods
SubjectsIn total, 67 participants (32 men and 35 women; mean age, 66.24±13.70 years of age, range, 20-83 years) with known or suspected intracranial artery diseases, were recruited in this study.
MRI experiment
All MRI experiments were performed at a 3T MR scanner (Discovery MR750w, GE, USA) with 24 channel coil. Straight inferior to the continuous RF pulse, pulsed labeling has been added followed by an inversion time. For fair comparison, the total length of ASL module was fixed to 1500ms between both MRAs, whereas the inversion pulse and inversion time were 1380 ms and 100 ms for cASL-ZTE-MRA and hASL-ZTE-MRA, respectively. Identical ZTE acquisition with 3D radial sampling was applied for both approaches showing as follows: FOV, 180 mm×180 mm; matrix, 150×150; spokes per segment, 512; TR, 862 ms; TE, 0.016 ms; flip angle, 3°; bandwidth, 31.25 kHz; NEX, 1; thickness, 1.2 mm; slices, 332; and total scan time, 344 seconds.
Data analysis
Due to different labeling preparations, sound assessment was conducted to ascertain the maintenance of acoustic noise reduction. Overall MRA image quality (including diagnostic confidence, image blurring, lesion conspicuity, and flow void artifacts) was scored qualitatively by referring to a 5-point Likert scale[1]. Signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) were calculated quantitatively. Stenotic grading and aneurysm measurement were recorded for further analysis. The CTA results were used as the reference.
Statistical analysis
All statistical analyses were performed using SPSS 19.0 software. The Wilcoxon signed-rank test was used to analyze sound experience and image quality ratings between both MRAs. The difference in the sound intensity among the ambient and both MRA conditions was analyzed using ANOVA analysis. The SNR and CNR obtained from both MRA methods were compared using the paired t test. Weighted kappa (κ) statistics were used to evaluate the agreement of stenosis assessment between cASL- or hASL-ZTE-MRA and CTA. Intraclass correlation coefficient (ICC) was used to test the consistency of measurements obtained using cASL- or hASL-ZTE-MRA and CTA. P value < 0.05 was considered statistically significant.
Results
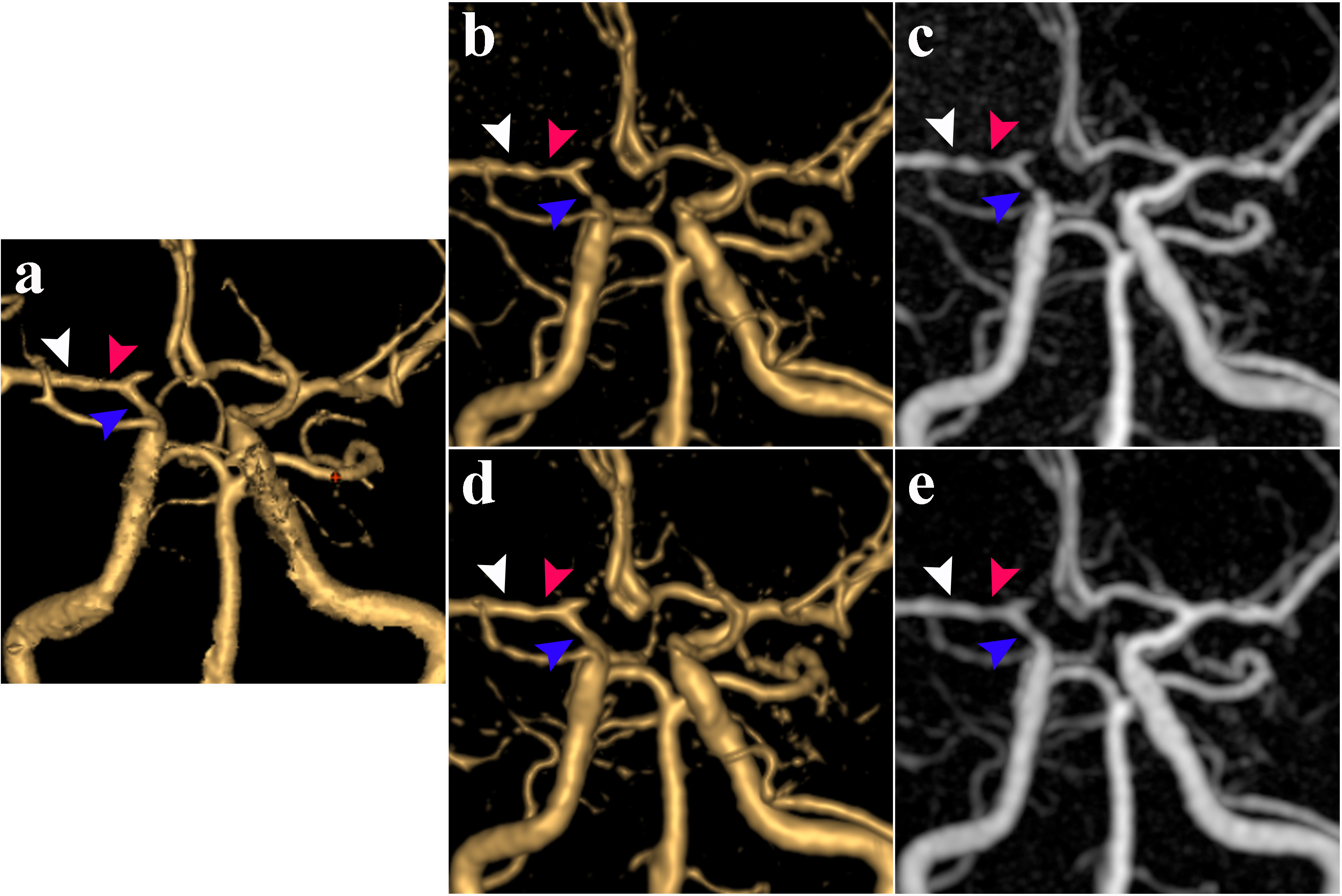
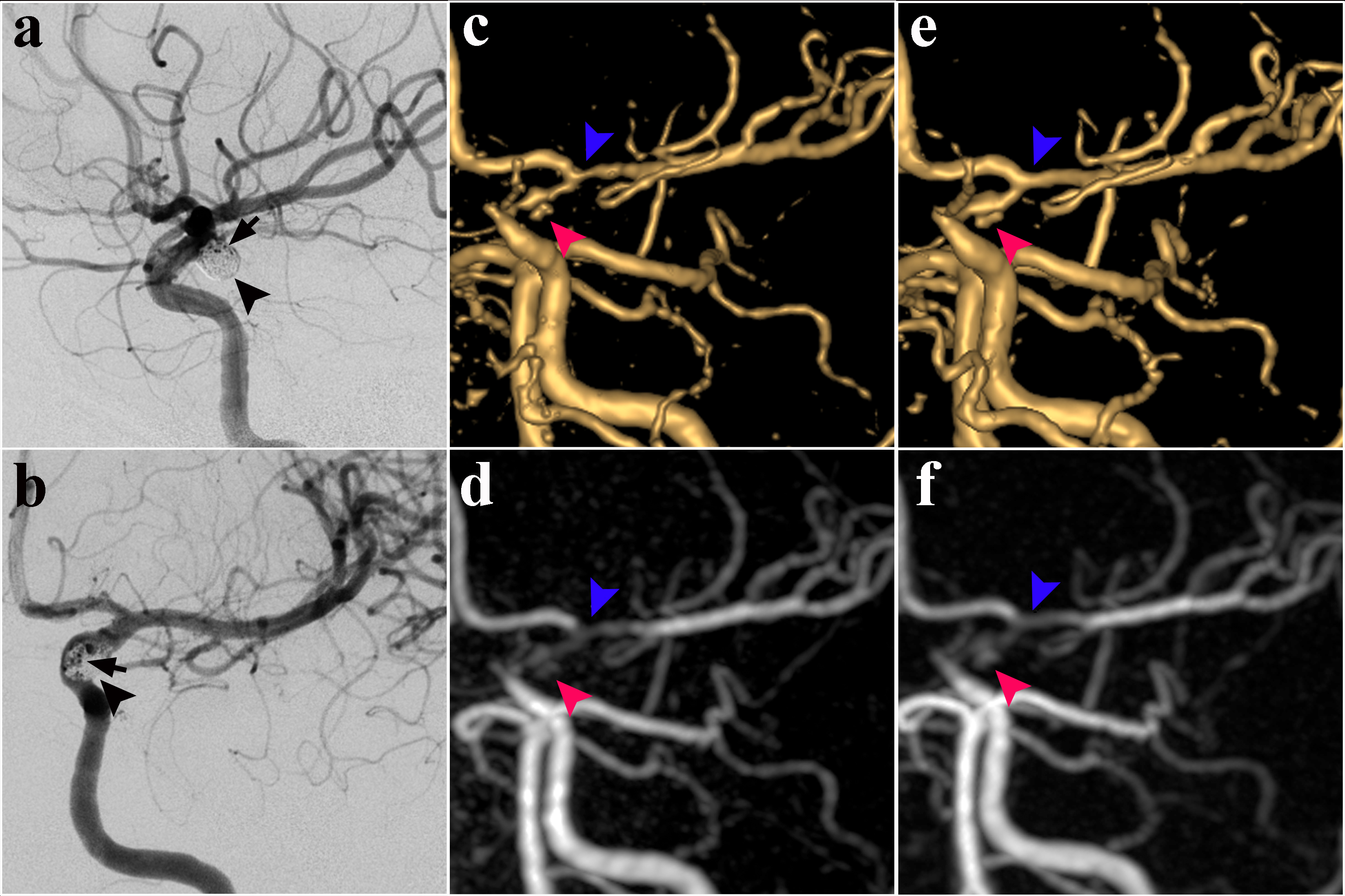
Based on CTA imaging, 36 steno-occlusive lesions, 29 cerebral aneurysms, 5 arteriovenous malformation (AVM) lesions, and 8 patients underwent endovascular procedures were diagnosed. Noise reduction and perception for hASL-ZTE-MRA was identical to cASL-ZTE-MRA. Mean IQ score for hASL-ZTE-MRA were slightly higher than that of cASL-ZTE-MRA (4.16 ± 0.62 versus 3.92 ± 0.64). More specifically, hASL-ZTE-MRA provided improved IQ scores with less image blurring and flow void artifacts. Moreover, hASL-ZTE-MRA provided higher SNR/CNR than that of cASL-ZTE-MRA (53.82±12.4 versus 47.89±11.96; 49.16±11.99 versus 43.67±11.49). Signal uniformity was improved on hASL-ZTE-MRA, particularly among the anterior circulation (Fig. 1).Comparing to cASL-ZTE-MRA, hASL-ZTE-MRA provided highly assessed stenotic lesions (Fig.2); better depicted flow in the stent or aneurysm remnant (Fig. 3); increased vessel contrast in AVM nidus. While comparable aneurysm measurements were found between both MRAs, slightly higher signal contrast was shown on hASL- than cASL-ZTE-MRA.
Discussion and conclusion
In the present study, we validated hASL-ZTE-MRA clinically in the evaluation of intracranial artery diseases by comparing with previously proposed cASL-ZTE-MRA. Our results revealed that the IQ score of hASL-ZTE-MRA had diagnostic value and was improved relative to cASL-ZTE-MRA, including fewer flow-related artifacts and higher flow signal uniformity, particularly in the proximal segments of anterior circulation. Both hASL- and cASL- ZTE-MRA were excellent in the steno-occlusive grading and aneurysm measurements. Additionally, the flow in the stenosis, stent and AVM was better portrayed on hASL- than cASL-ZTE-MRA.In conclusion, hASL-ZTE-MRA has been demonstrated a feasible method for assessing intracranial artery diseases clinically, especially steno-occlusive lesions. While maintaining ZTE readout features, hASL-ZTE-MRA is robust with diagnostic IQ scores and improved signal homogeneity over cASL-ZTE-MRA. This modified ZTE-MRA offers an appealing noncontrast-enhanced alternative for clinical cerebrovascular evaluation and follow-up assessment.
Acknowledgements
No acknowledgement found.References
[1] Arai N, Akiyama T, Fujiwara K, et al. Silent MRA: arterial spin labeling magnetic resonant angiography with ultra-short time echo assessing cerebral arteriovenous malformation[J]. Neuroradiology, 2020,62:455-461.
[2] Holdsworth SJ, Macpherson SJ, Yeom KW, et al. Clinical Evaluation of Silent T1-Weighted MRI and Silent MR Angiography of the Brain[J]. AJR Am J Roentgenol, 2018,210:404-411
[3] Qu J, Wu B, Zhou Z. Silent magnetic resonance angiography with hybrid arterial spin labeling techniques. In: Proceedings of the An-nual Meeting of the International Society for Magnetic Resonance in Medicine, Singapore. May 7–13, 2016
Figures