1641
Quantitative evaluation of thrombus length and its relationship with the severity and prognosis of acute cerebral infarction using CUBE imaging1The First Affiliated Hospital of Shandong First Medical University, Jinan, China, 2GE Healthcare, MR Research China, Beijing, China
Synopsis
This study aimed to quantitatively evaluate thrombus length and its relationship with the severity and prognosis of acute cerebral infarction using high resolution CUBE imaging. National institute of health stroke scale (NIHSS) score and modified rankin scale (mRS) score were used to quantify the degree of neurological impairment and the prognosis of patients. The length of cerebral artery thrombosis was measured with CUBE imaging. Strong relationship was revealed between the thrombus length and NIHSS or mRS score. We therefore demonstrated that thrombus length measurement based on CUBE MRI can effectively evaluate the severity and prognosis of acute cerebral infarction.
INTRODUCTION
Most ischemic cerebral infarction is caused by cerebral artery thrombosis. Quantitative evaluation of thrombus has prognostic and therapeutic significance in patients with acute stroke1. Traditional imaging techniques showed the stenosis or filling defect of the vascular lumen to indirectly explain the existence of intravascular thrombosis. It thus remains challenging to accurately measure thrombosis length2.CUBE magnetic resonance imaging (MRI), as a three dimensional (3D) high resolution imaging technique, has been widely applied in the diagnosis of intracranial arterial wall lesions3. With CUBE imaging, intracranial arterial thrombosis has been accurately detected and measured4.Based on these studies,we assumed CUBE imaging might hold the potential to measure thrombus length quantitatively. Therefore, the main goals of this study were to investigate the feasibility of high resolution CUBE imaging for measuring the length of intravascular thrombus, and to further explore the relationship of thrombus length with the severity and also the prognosis of acute cerebral infarction.
MATERIALS AND METHODS
SubjectsSixty-four patients (50 males and 14 females, mean age:57 years old, onset time 8hr to 14d) with cerebral artery thrombosis diagnosed by digital subtraction angiography(DSA). Each patient was measured with MRI experiment after written informed consents were obtained.
MRI experiment
All MRI experiments were performed on a 3T clinical scanner (Discovery 750w, GE Healthcare, USA) equipped with a 32-channel coil. 3D fast-spin-echo based T1 weighted CUBE sequence was scanned with scan parameters of TR=600ms, TE=14.4ms, slice thickness=1mm, slice gap=0.5mm, FOV=200mm×200mm for whole brain coverage, matrix size=288x288 and echo chain length=24. Total scanning time was 4 minutes 16s.
Data analysis
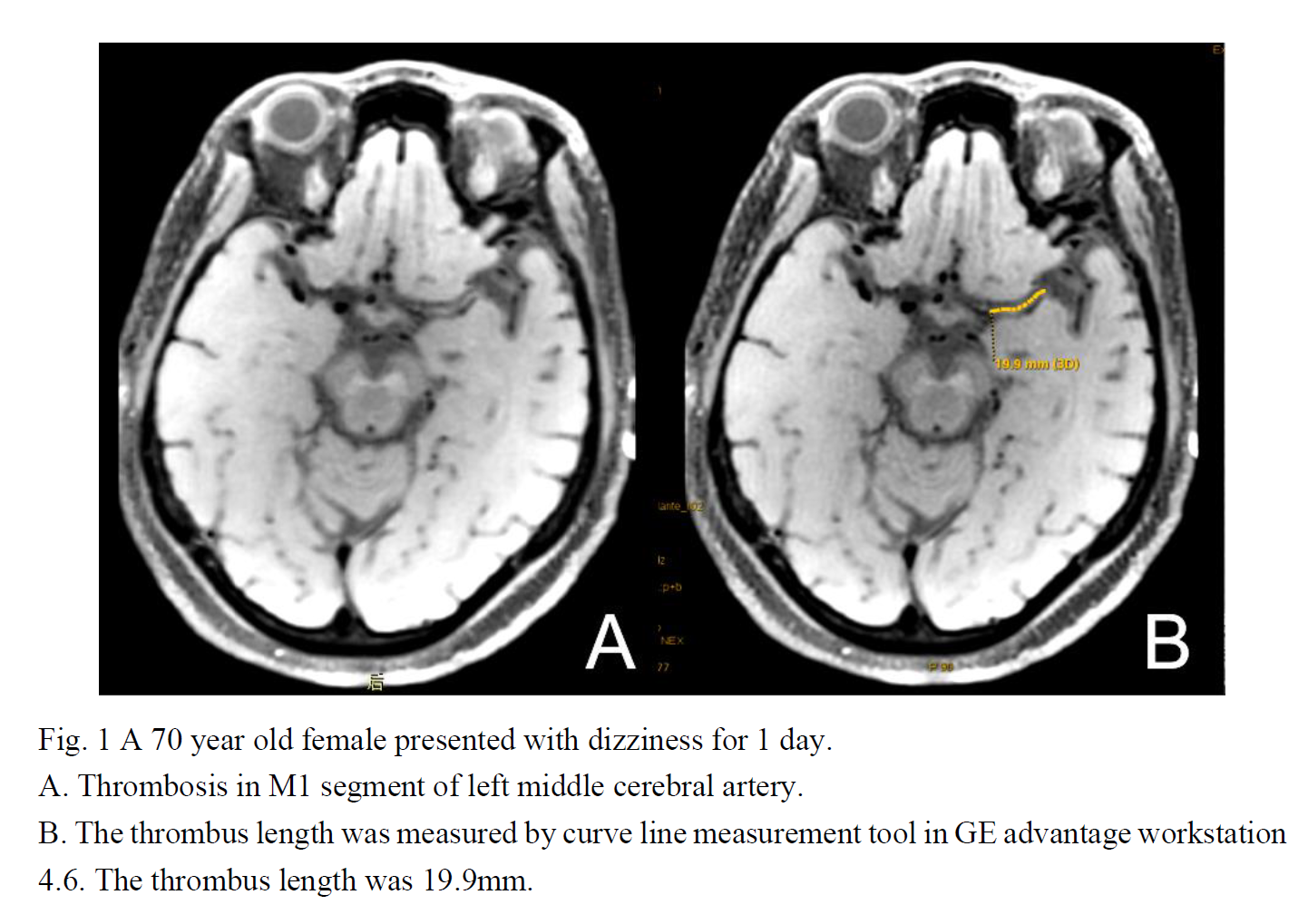
On the acquired CUBE images, intraluminal thrombus was defined as the presence of high signal or iso-signal filling in the lumen compared to normal vessel with low or no signal intensity. In addition, the length of cerebral artery thrombosis was measured based on CUBE images (Fig.1)
Each patient with thrombosis was applied by national institute of health stroke scale (NIHSS) score for neurological impairment evaluation, and modified rankin scale (mRS) score for prognosis assessment after 3 months follow-up. The relationship between the thrombus length and NIHSS score was explored by multiple linear regression model. According to mRS score, patients with cerebral artery thrombosis were divided into poor and good prognosis groups. Multivariate logistic regression model was used to explore the relationship between thrombus length and clinical prognosis. All statistical analyses were performed in R for Window v3.5.1 software and p<0.05 was considered statistical significance.
RESULTS
No significant difference was found in the mean age, thrombus length, NIHSS score, mRS score and the distribution of past history of five diseases between male and female (P>0.05; Table.1), except for male and female smokers (P<0.05).The distribution of thrombus lengths between different NIHSS scores was statistically significant (P<0.05; Table.2). No significant difference in age, gender, smoking history distribution and history of five diseases were found among different NIHSS scores (P>0.05). Using NIHSS score as dependent variable (y) and thrombus length as independent variable (x), multiple linear regression model was established using optimal subset method. The model form was y=0.46x-0.70sex-3.09, indicating that the average NIHSS score increases by 0.46 points for every 1 mm increase in thrombus length.
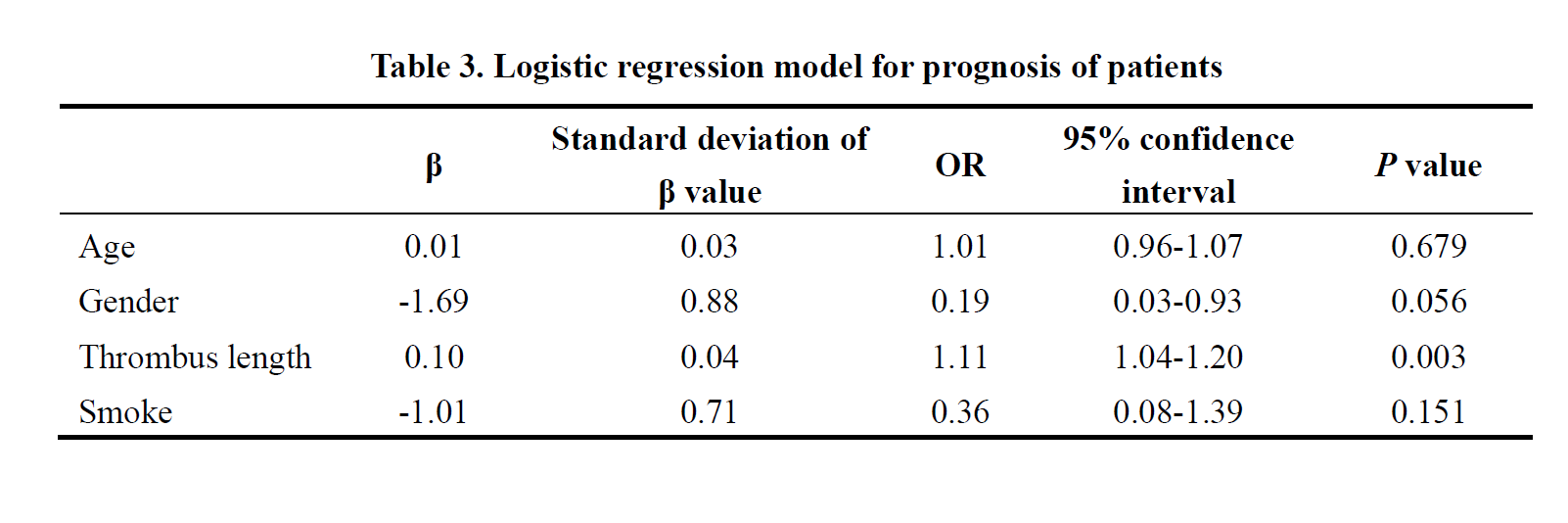
According to mRS score (Table.3), thrombus length was an independent risk factor for the prognosis of cerebral infarction, odds ratio (OR)=1.11>1, and the confidence interval was 1.04-1.20, P<0.05. It means that the risk of poor prognosis increases by 1.11 times for every 1 mm increase of thrombus length.
DISCUSSION
In this study, thrombus lengths over patients with different NIHSS scores were statistically different. NIHSS score reflects the degree of nervous system damage, indicating a relationship with the thrombus length. Through the multiple linear regression model, we found that the average NIHSS score is proportional to the thrombus length, indicating that longer thrombus may introduce more serious damage of nervous system. A possible reason is that when the main stem of cerebral artery is blocked by thrombus, multiple collateral branches from the main stem are blocked at different degrees. Longer thrombus involves more branches, therefore the collateral circulation cannot be established effectively, resulting in increased degree of nervous system damage.In addition, the thrombus length was also found as a risk factor for poor prognosis of cerebral infarction in this study. This may also attribute to the effect of long thrombus on the establishment of collateral circulation.
CONCLUSION
In conclusion, the measured thrombus length using high resolution CUBE imaging has demonstrated a strong correlation with NIHSS and mRS score, revealing clinical potential in evaluating the severity and prognosis of acute cerebral infarction.Acknowledgements
No acknowledgement found.References
[1] Riedel C H, Zimmermann P, Jensen-Kondering U, et al. The Importance of Size: Successful Recanalization by Intravenous Thrombolysis in Acute Anterior Stroke Depends on Thrombus Length[J]. Stroke, 2011, 42(6):1775-1777.
[2] Ishimaru H, Ochi M, Morikawa M, et al. Accuracy of pre-and postcontrast 3D time- of-flight MR angiography in patients with acute ischemic stroke:correlation with cath- eter angiography[J]. AJNR.American journal of neuroradiology, 2007, 28(5): 923- 926.
[3] Mandell D M, Mossabasha M, Qiao Y, et al.Intracranial Vessel Wall MRI:Principles and Expert Consensus Recommendations of the American Society of Neuroradiology[J].Ajnr Am J Neuroradiol, 2017, 38(2): 218-229.
[4] Zhang C, Wang X Y,Dou W Q,et al.The feasibility of High resolution MRI in Length Measurement of Cerebral Arterial Thrombosis:a correlation study with Catheter Angiography.Proceedings of the 28th Annual Scientific Meeting ISMRM, Paris, France, 2020; 4479.
Figures
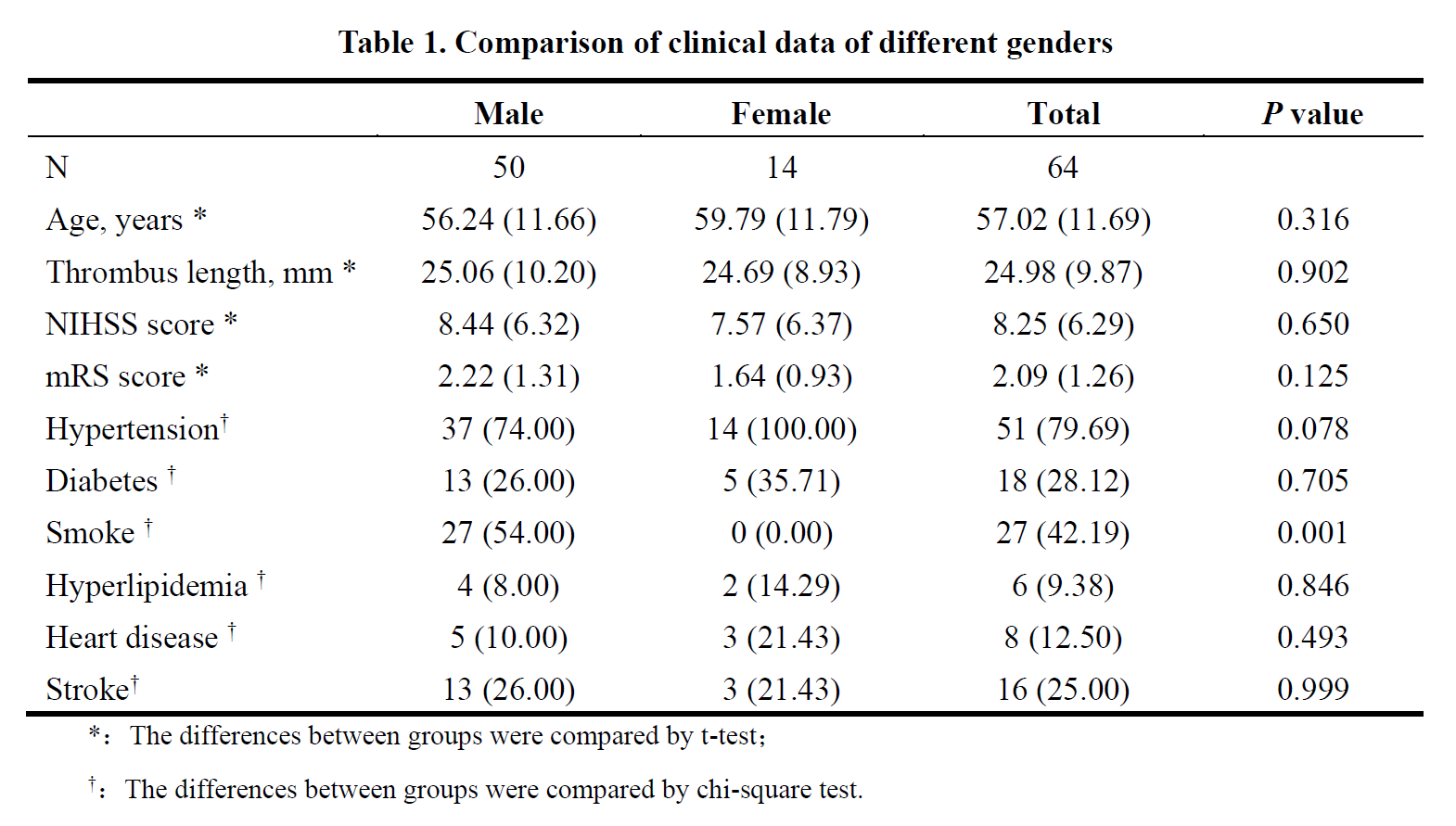
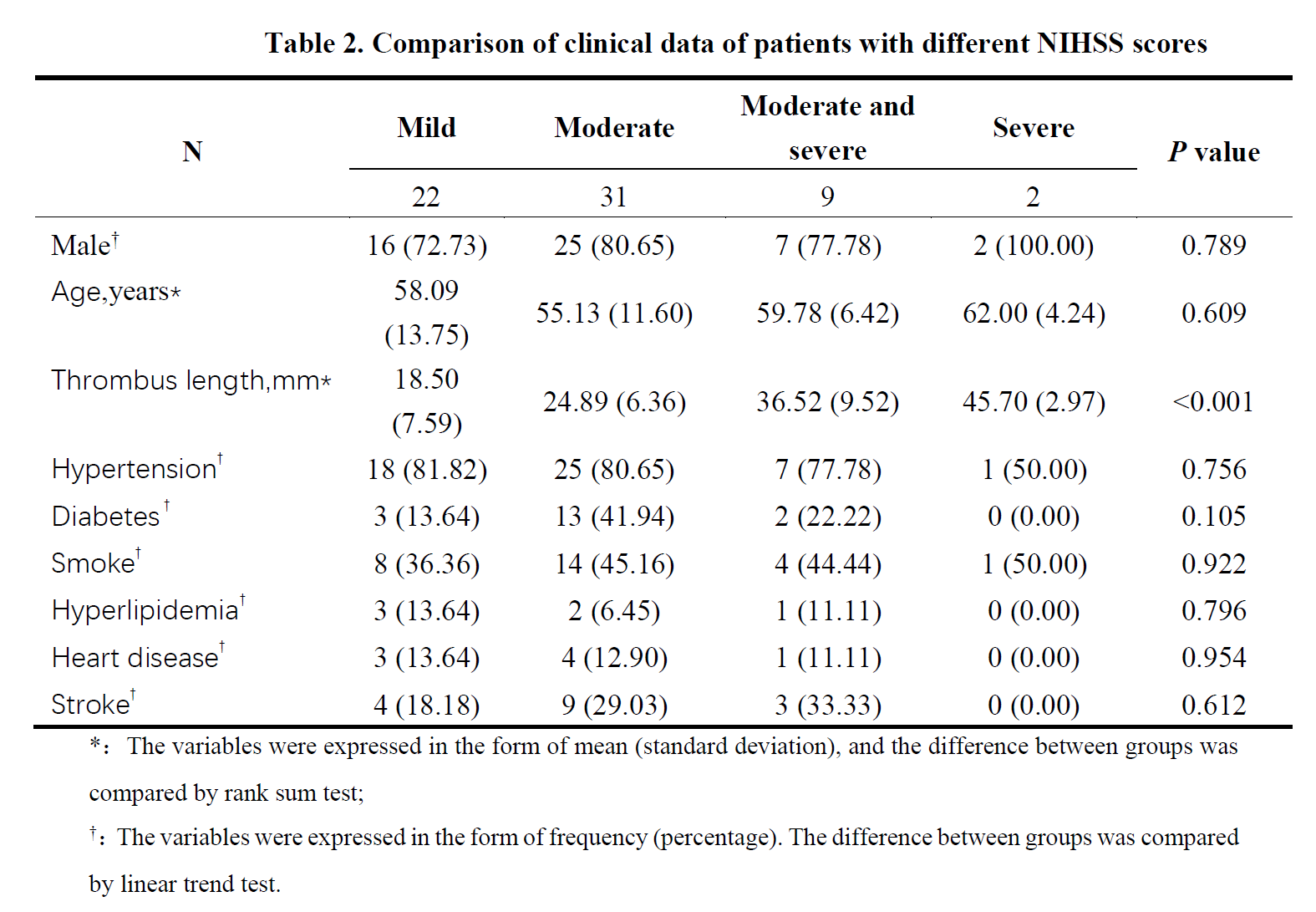
Table 2