1638
MRA based on pointwise encoding time reduction with radial acquisition improves uniformity of cavernous segment of internal carotid artery1Radiology, First Central Clinical College, Tianjin Medical University, Tianjin, China, 2Radiology, China-Japan Friendship Hospital, Beijing, China, 3MR Collaboration, Siemens Healthcare, Beijing, China, 4MR Application, Siemens Healthcare, Beijing, China, 5Radiology, Tianjin First Central Hospital, Tianjin, China
Synopsis
This study compared the differences between PETRA-MRA and TOF-MRA on the imaging of the cavernous segment of the ICA with qualitative analysis (image quality) and quantitative analysis (SNR, CNR, CR, and uniformity). The results showed that PETRA-MRA significantly improved the uniformity and CR of the cavernous segment of ICA, although it is inferior in both SNR and CNR. This suggests that PETRA-MRA could provide a reasonable alternative to reduce the loss of signal from curved vessels.
Purpose
To assess the clinical value in the imaging of cavernous segment of internal carotid artery (ICA) between two magnetic resonance angiography (MRA) techniques, time-of-flight (TOF) and pointwise encoding time reduction with radial acquisition (PETRA).Methods
The study cohort included 37 healthy subjects who underwent both PETRA-MRA and TOF-MRA on a 3T system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany). PETRA-MRA was obtained by acquiring the labeled and the control data. A slice-selective saturation pulse was applied upstream to the carotid artery, which had the potential to darken the arterial inflow. The saturation pulse was also adopted in the control data and was only prescribed outside of the imaging volume for the MT effects while not interfering with the imaging volume. Then, these two data sets were subtracted to generate arterial MRA with background tissue and venous flow suppressed. We fixed the head by filling the coil with sponge to avoid the pixel dislocation caused by head displacement. The acquisition parameters of both MRA sequences were as follow. TOF-MRA: TR=21 ms; TE=3.69 ms; voxel size=0.5×0.5×0.8mm3; FOV=200×174mm2; 4 slabs; 44 slices per slab; flip angle=20°; bandwidth=186 Hz/Px; parallel acceleration factor=2 ; acquisition time=5 min 28 s. PETRA-MRA: TR=3.31 ms; TE=0.07 ms; Radial views=45,000; voxel size=1×1×1mm3; FOV=250×250mm2; 1 slab; 256 slices per slab; flip angle=3°; bandwidth=403 Hz/Px; total acquisition time for the labeled and the control data=6min 52s.Two neuroradiologists reviewed the images blindly and evaluated the image quality about delineation of the cavernous segment of ICA on a 5-point scale independently. Quantitative measurements of signal-to-noise ratio (SNR), contrast-to-noise ratio (CNR), contrast ratio (CR), and uniformity were also performed. Weighted KAPPA (for grading of image quality) and intraclass correlation coefficient (ICC, for quantitative measurements) were used to assess inter-reader agreement. Wilcoxon signed-rank tests were used to identify the difference between these two MRA images. GraphPad Prism (version 8.0; GraphPad Software Inc., San Diego, CA, USA) and SPSS (version 23.0, IBM Corp., Armonk, NY, USA) were used for all analyses. A P-value less than 0.05 indicated statistical significance.
Results
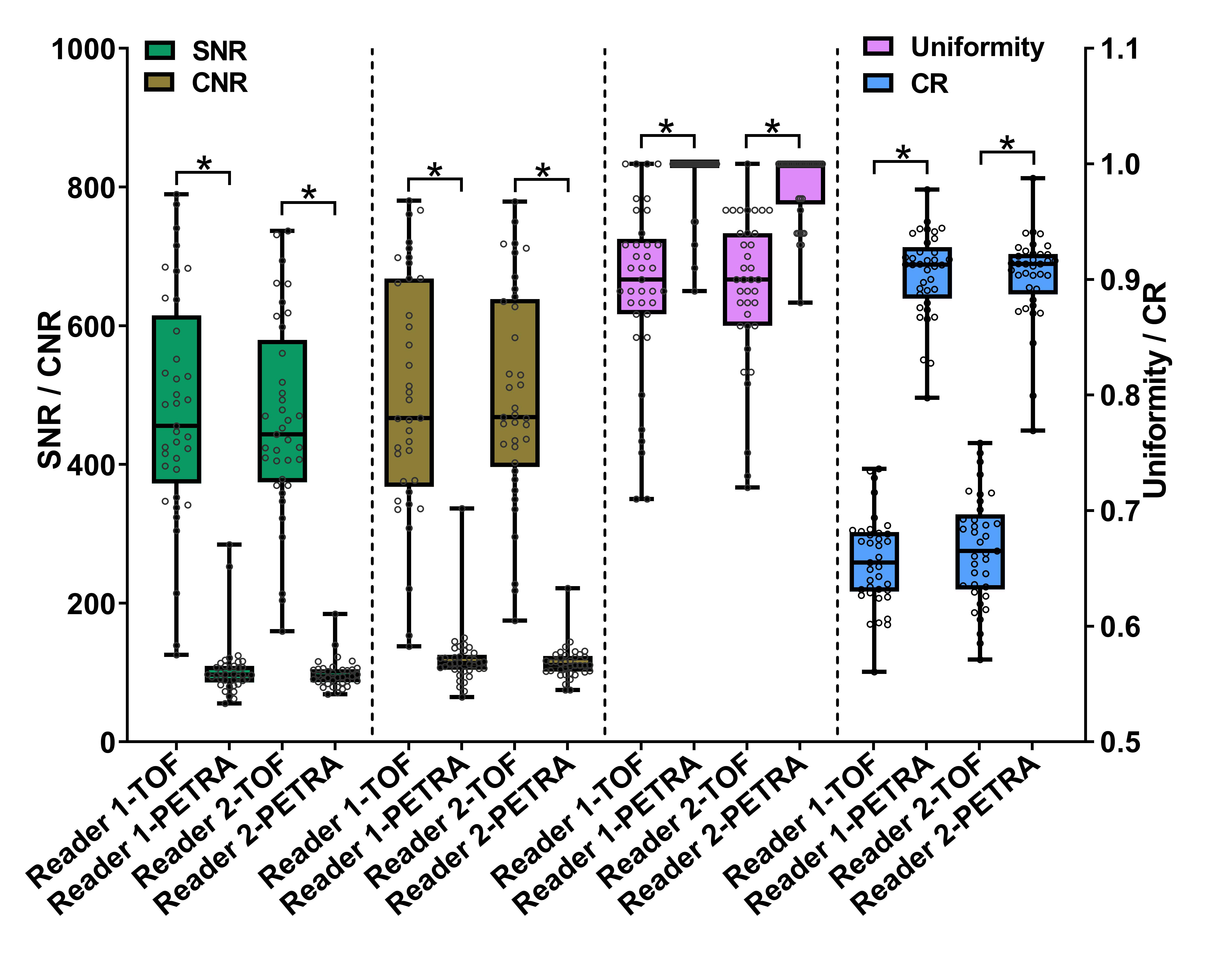
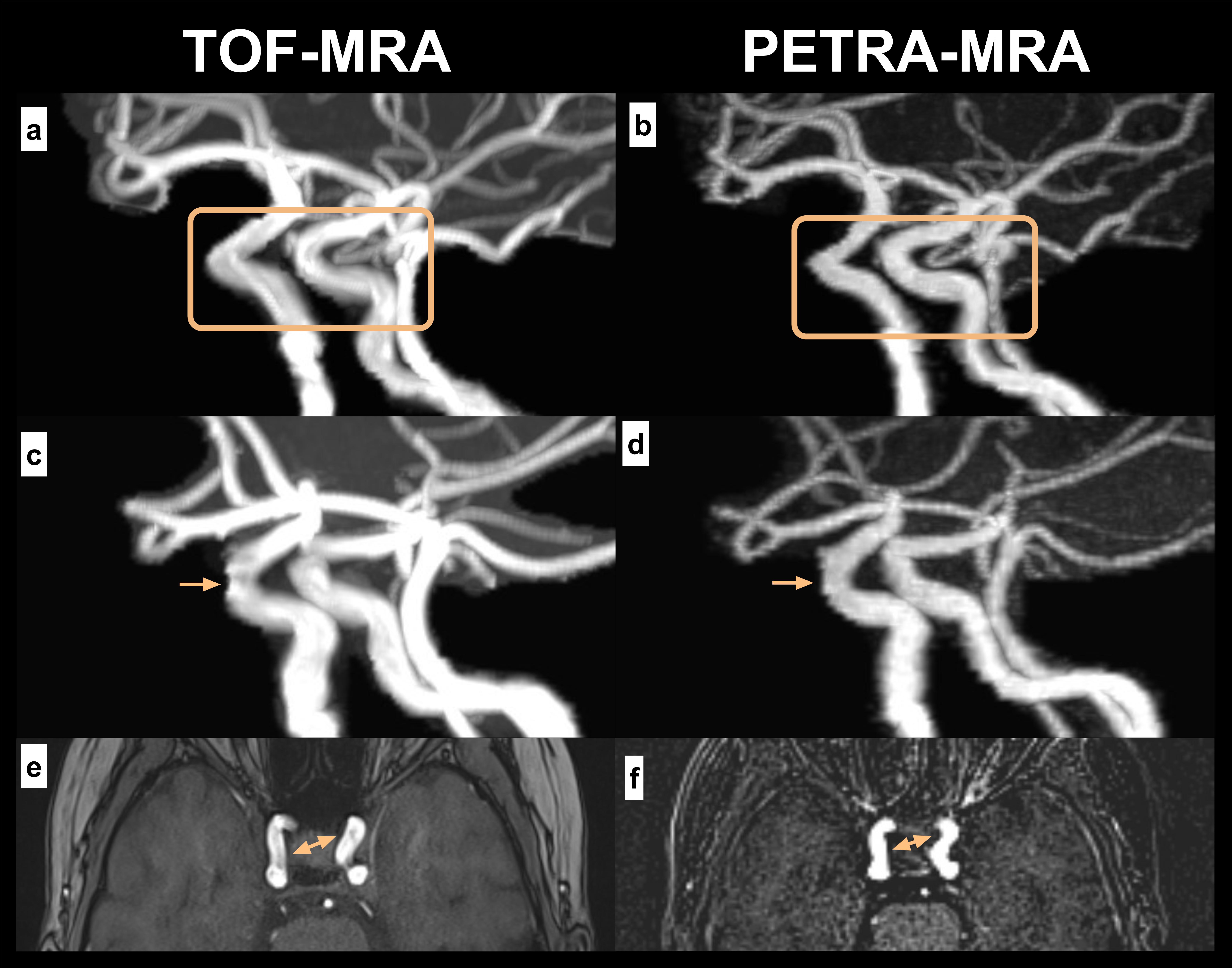
The mean score for delineation of the cavernous segment of the ICA was significantly higher in PETRA-MRA than in TOF-MRA (P< .001 for both readers), and good inter-reader agreement was reported. For the SNR and CNR, TOF-MRA was significantly better than PETRA-MRA, but CR and uniformity of PETRA-MRA were significantly higher than of TOF-MRA (P< .001 for both readers). The results are shown in Fig.1. The inter-reader agreement was excellent (SNR of TOF-MRA and PETRA-MRA, CNR of TOF-MRA, CR of TOF-MRA and PETRA-MRA) or good (CNR of PETRA-MRA, uniformity of TOF-MRA and PETRA-MRA). Higher uniformity of the cavernous segment of the ICA on PETRA-MRA images compared to TOF-MRA images is also shown in Fig.2.Discussion
TOF-MRA uses the blood flow–related enhancement of unsaturated spins entering into an imaging slice as means to generate a contrast between the stationary tissue and the moving blood [1]. PETRA-MRA is based on the principle of ASL strategy, which involves arterial blood signal with high intensity in control images, and negative or small blood signal in labeled images, the difference between these two states constituting arterial blood signal and background suppression in the subtracted angiographic image [2]. Therefore, TOF-MRA is sensitive to flow with diminution of velocity, which remains in the imaging volume for a long time and is repeatedly stimulated by RF pulses, resulting in saturation effect and signal attenuation or loss [3-5]. In PETRA-MRA, arterial signal intensity depends more on the longitudinal relaxation time of the labeled spins and signal acquisition time than on the vessel curvature and flow status. Although PETRA-MRA was inferior in both the SNR and CNR, it demonstrated better contrast and uniformity in delineation of the cavernous segment of the ICA compared to TOF-MRA.Conclusions
In conclusion, PETRA-MRA showed promising image quality without dephasing and saturation artifact, as well as better background suppression. And it can be used to improve the certainty of diagnosis.Acknowledgements
No acknowledgement found.References
1. Bosmans H, Marchal G, Lukito G, et al. Time-of-flight MR angiography of the brain: comparison of acquisition techniques in healthy volunteers. AJR Am J Roentgenol 1995; 164(1):161-167. DOI: https://doi.org/10.2214/ajr.164.1.7998531
2. Suzuki Y, Fujima N, van Osch MJP. Intracranial 3D and 4D MR Angiography Using Arterial Spin Labeling: Technical Considerations. Magn Reson Med Sci 2019 Nov 22. [Epub ahead of print]
3. Wilcock DJ, Jaspan T, Worthington BS. Problems and pitfalls of 3-D TOF magnetic resonance angiography of the intracranial circulation. Clin Radiol 1995; 50(8):526-532. DOI: https://doi.org/10.1016/s0009-9260(05)83186-1
4. Oshinski JN, Ku DN, Pettigrew RI. Turbulent fluctuation velocity: the most significant determinant of signal loss in stenotic vessels. Magn Reson Med 1995; 33(2):193-199. DOI: https://doi.org/10.1002/mrm.1910330208
5. Furst G, Hofer M, Sitzer M, et al. Factors influencing flow-induced signal loss in MR angiography: an in vitro study. J Comput Assist Tomogr 1995; 19(5):692-699. DOI: https://doi.org/10.1097/00004728-199509000-00002
Figures