1631
Usefulness of 3D Radial Stack-of-stars Ultra-short TE MRA after Treatment of Cerebral Aneurysms with Metallic Devices1Radiology, Eastern Chiba Medical Center, Chiba, Japan, 2Philips Japan, Tokyo, Japan, 3Eastern Chiba Medical Center, Chiba, Japan
Synopsis
We combined 3D radial sequences using stack-of-stars acquisition with uTE sampling to enable short-time imaging of local areas. This study was to apply uTE sequences using 3D radial stack-of-stars collection to MRA to determine its usefulness as a follow-up MRA after treatment of cerebral aneurysms metallic devices. The range of signal reduction around the treated area was significantly smaller in the uTE-MRA than in the TOF-MRA. uTE-MRA improved the visualization of peri-aneurysm vessels and neck remnant in the metallic devices. uTE-MRA using 3D radial stack-of-stars collection is useful for follow-up MRA after treatment of cerebral aneurysms metallic devices.
Purpose
Ultrashort- or zero-TE (uTE) MRA based Arterial Spin Labeling (ASL)1) has limitations in terms of spatial resolution and number of imaging slices, because it requires koosh-ball sampling with whole brain coverage to minimize the aliasing artifacts. Such sequences are not suitable for fast and focal acquisition.In this study, we combined 3D radial sequences using stack-of-stars acquisition2) with uTE sampling3) to achieve fast imaging with focal slice coverages. The aim of this study was to evaluate the feasibility of uTE MRA using 3D radial stack-of-stars and to determine its clinical usefulness in a follow-up MRA studies after treatment of cerebral aneurysms metallic devices.Methods
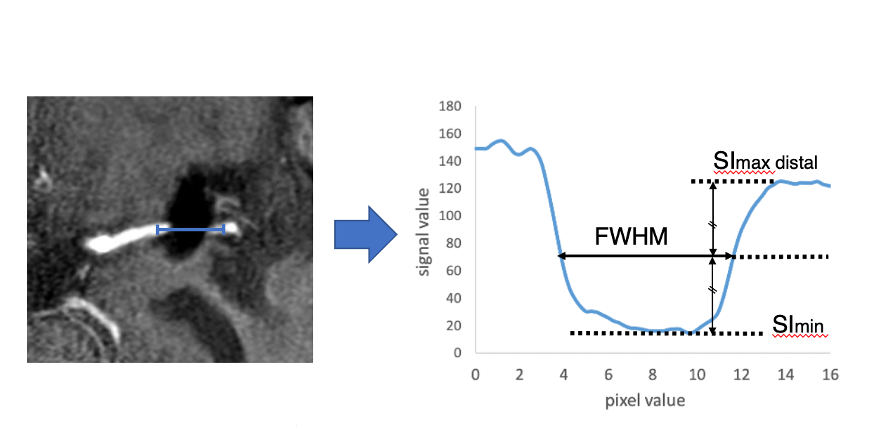
All subjects were examined with 3.0T whole-body clinical system (Ingenia CX, Philips Healthcare). We performed conventional TOF-MRA and uTE-MRA scans in patients who treatment of cerebral aneurysms with metallic devices (clipping: 10 patients, coil embolization: 10 patients). We evaluated the image quality of the clip and coil perimeter and statistically compared the image quality of these two methods to the parent vessel delineation around the treated area of MRA. To assess image quality, multi planer reconstruction (MPR) was performed so that the cerebral vessels around the treated area were visible on the long axis, and analysis was performed using profile curves. In order to evaluate the extent of signal reduction, the full width at half maximum (FWHM) was calculated based on the maximum value (SImax distal) of the outflow side and the minimum value (SImin) of the reduced signal region (Fig.1).Results
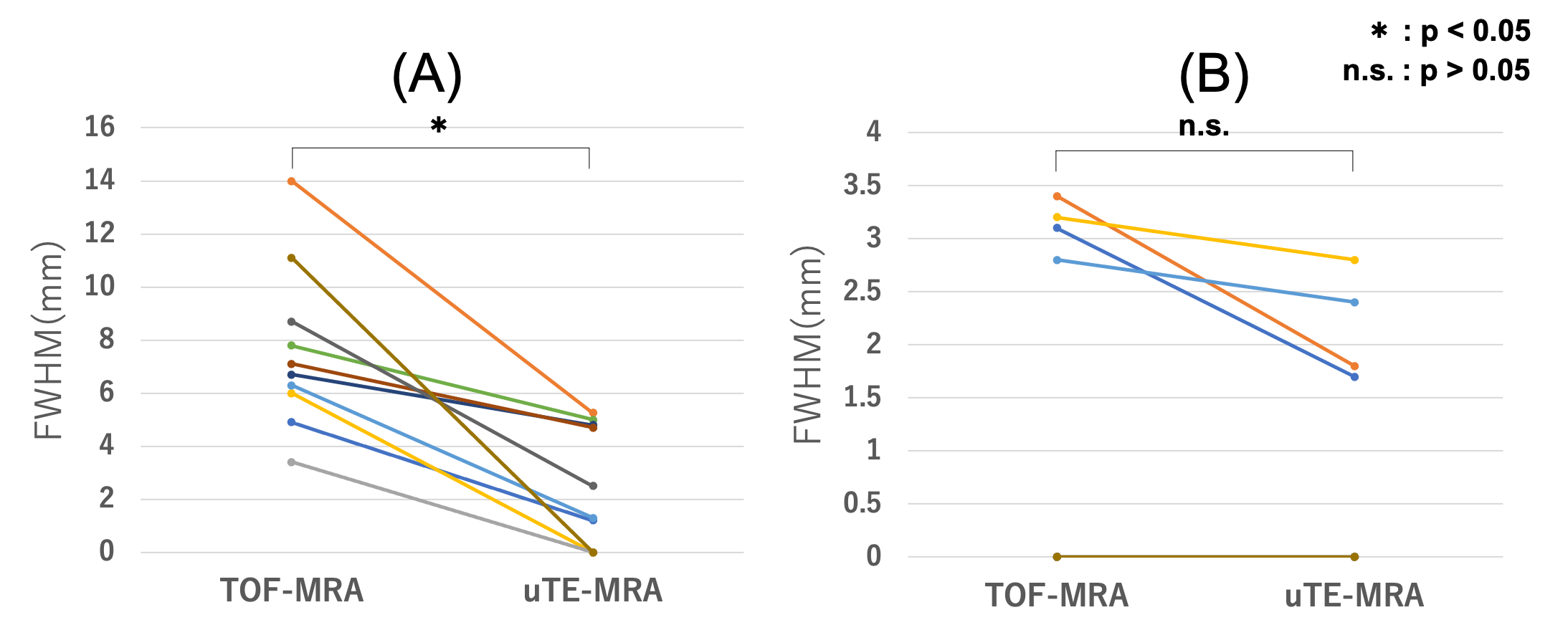
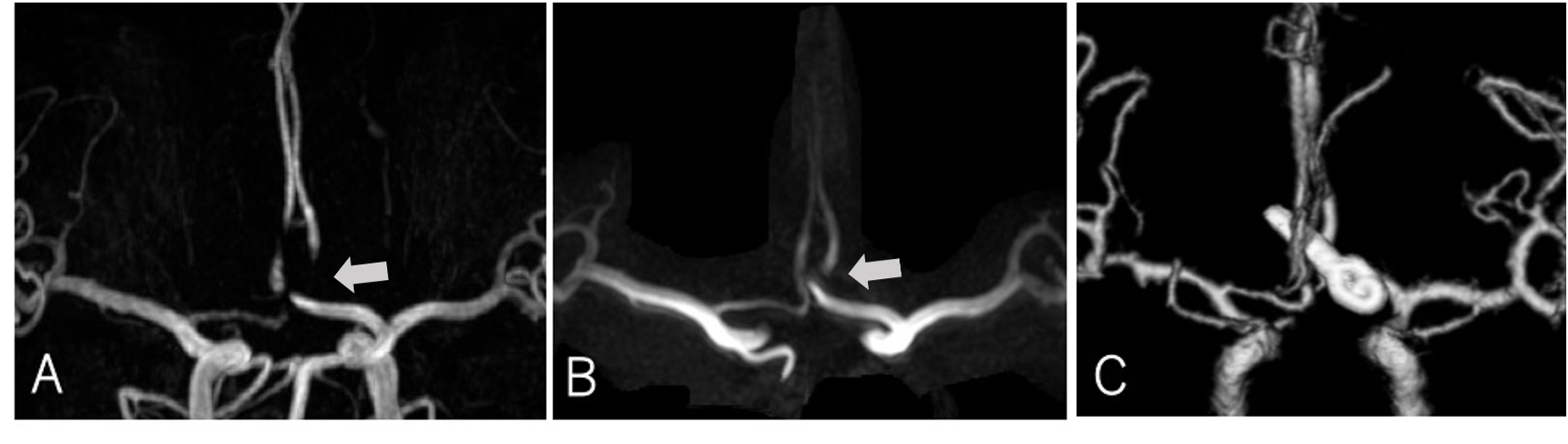
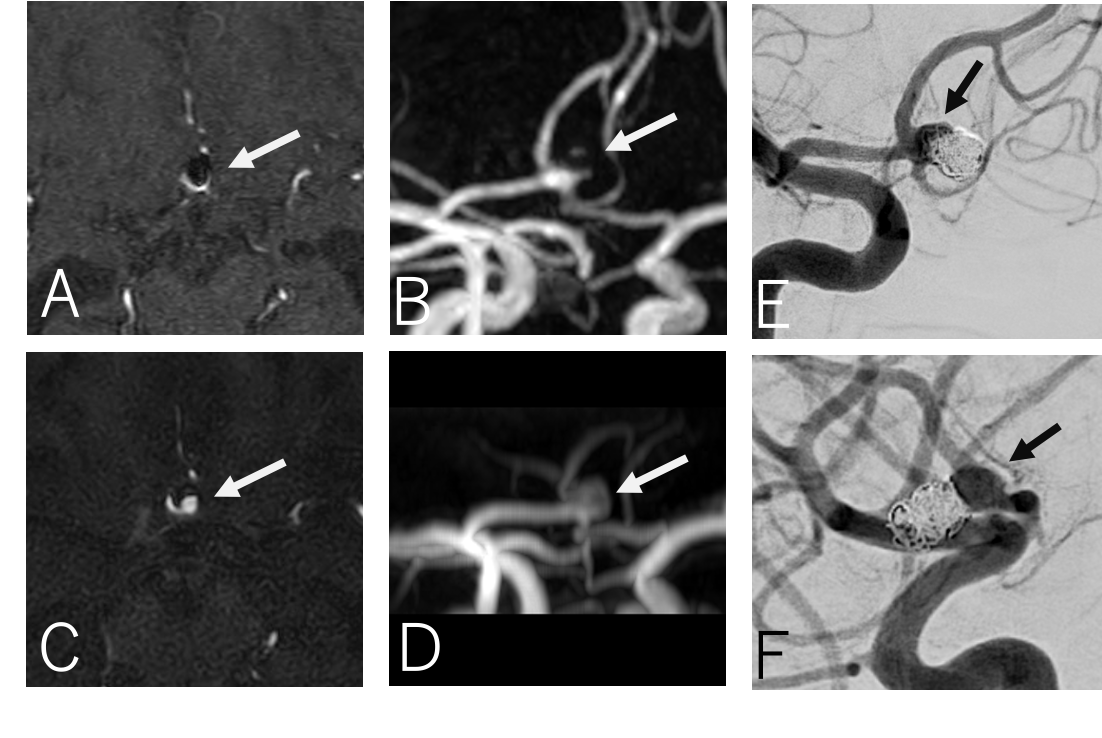
In the clip cases, FWHM was significantly smaller in uTE-MRA than in TOF-MRA. However, there was no significant difference between uTE-MRA and TOF-MRA in the coil cases (Fig.2). In the clinical images, uTE-MRA significantly improved the visualization ability compared to TOF-MRA (Fig.3,4). This is because shortening the TE to 0.38 ms reduced the magnetic susceptibility artifacts around the metal and improved the ability to visualize the peri-aneurysm and residual blood flow around the metal device.Conclusion
uTE-MRA using 3D radial stack-of-stars sampling is useful for follow-up MRA after treatment of cerebral aneurysms metallic devices.Acknowledgements
No acknowledgement found.References
1) Saki Takubo, et al. Clinical Usefulness of Ultra-short TE MRA for Follow-up Imaging after Cerebral Aneurysm Clipping. Nihon Hoshasen Gijutsu Gakkai Zasshi 2020;76(2):177-184.
2) Kai Tobias Block, Hersh Chandarana, Sarah Milla et al. Towards Routine Clinical Use of Radial Stack-of-Stars 3D Gradient-Echo Sequences for Reducing Motion Sensitivity. JKSMRM 2014;18(2):87-106.
3) Jurgen Rahmer, Peter Bornert, Jan Groen, and Clemens Bos. Three-Dimensional Radial Ultrashort Echo-Time Imaging with T2 Adapted Sampling. Magnetic Resonance in Medicine 2006;55(5):1075–1082.
Figures