1630
Quantitative MRI to compare vascular health in nonsmokers, smokers, and vapers.
Alessandra Caporale1, Michael Langham1, and Felix W Wehrli1
1Radiology, Laboratory for Structural, Physiologic and Functional Imaging, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, United States
1Radiology, Laboratory for Structural, Physiologic and Functional Imaging, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, United States
Synopsis
To investigate the effects of chronic exposure to cigarette smoke or electronic cigarette aerosol on the vascular endothelium, various MRI parameters were examined in an ongoing study involving healthy young people (mean age<30y). Peripheral, cerebrovascular reactivity, and central aortic stiffness were evaluated comparing smokers (N=11) and vapers (N=15) to their nonsmoking-peers (N=31). There were no significant differences between groups, but hyperemic blood flow acceleration trended lower in smokers/vapers while arterial stiffness trended higher in smokers, relative to nonsmokers. The findings may suggest that exposure in these young subjects was not be sufficient to cause measurable adverse effects on the endothelium.
Background and Motivation
Electronic cigarettes (e-cig) are now in widespread use, typically comprising tobacco smokers desirous to quit smoking, but increasingly also by previously nonsmoking adolescents[1]. E-cigs generate a flavored aerosol which, although free of tar, contains harmful substances[2-4], which in addition to nicotine, adversely affect the vascular endothelium acutely[5-6]. Repeated exposure to e-cig aerosol, similar to tobacco smoke, may set the stage for endothelial dysfunction, eventually leading to cardiovascular disease. Therefore, studying the impact of long-term use of e-cig and tobacco cigarette (t-cig) on vascular health is important, given that vaping is promoted as a safer alternative to smoking, and considering that studies on chronic vascular effects of e-cig use are limited and controversial[7]. To investigate possible vascular alterations caused by t-cig or e-cig use in young adults, we compared various MRI parameters of vascular health in young healthy subjects (regular tobacco-cig users, regular e-cig users - vapers - and never smokers), in an ongoing study targeting three vascular territories (lower extremities, central arteries, and brain) with a single, 50-min MRI protocol.Methods
Eleven smokers and 15 vapers have been examined so far, for comparison with data acquired previously in 31 nonsmokers[6]. Nonsmokers had no previous smoking/vaping history; smokers and vapers were single users (of either t-cig or e-cig), with a smoking/vaping history of at least 1 year. Subjects were asked to fast and avoid stimulants (smoking, vaping, caffeinated drinks) for 8 and 4 hours prior to the MRI exam, respectively. Figure 1 summarizes demographics and details on the smoking/vaping status. Each participant underwent a 50-min MRI protocol (described extensively in[6]), implemented in SequenceTree[8], and performed on a 3T Siemens Prisma scanner. Briefly, three vascular locations were targeted: superficial femoral artery and vein, aortic arch, and superior sagittal sinus (SSS), using an 8-channel knee coil, an 18-channel body matrix combined with spine coil and a 20-channel head-neck coil, respectively. First, a cuff (Hokanson, Bellevue, Wash) placed around the thigh was inflated at ~215 mmHg for 5 minutes, to suspend the femoral circulation, with the imaged vessels lying within the ischemic territory. Arterial blood flow velocity (BFV) and venous saturation (SvO2) were measured dynamically during the reactive and responsive phases of hyperemia (within 30s and 2min post-cuff release, respectively)[9]. A temporal resolution of 120ms was achieved in BFV-mapping by means of a projection technique that obviates cardiac gating[10]. Figure 2 illustrates the parameterization of SvO2 and BFV time-courses. Peak luminal flow mediated dilation (FMD) was evaluated by means of high spatial resolution vessel-wall imaging during responsive hyperemia (Figure 2). Subsequently, cerebrovascular reactivity was measured in the SSS via phase-contrast imaging during three 30s-post-expiratory breath-holds (Figure 3), expressed in the form of a breath-hold-index (BHI) computed as the slope of the velocity-time curve during the period of suspended respiration. Finally, aortic arch pulse wave velocity (PWV), surrogate marker of central arterial stiffness, was quantified by temporally resolving BFV-dependent signal with velocity-sensitized projections in the absence of cardiac gating[11]. A Multivariate Analysis of Variance was performed in SPSS v20.0 (Armonk, NY: IBM Corp) with the smoking status as a factor with three levels. The effect of gender was also examined, due to potential gender differences[12] in the endothelium’s response to smoke or e-cig aerosol exposure.Results and Discussion
While the groups were comparable for body mass index, smokers were somewhat older than the other two (Figure 1). Consequently, smokers had been exposed to tobacco longer than e-cig vapers (given that vaping is of more recent vintage). Diastolic blood pressure (BP) was higher in both smokers and vapers (P=0.01; P=0.029) than in nonsmokers, whereas systolic BP was similar. FMD in nonsmokers (FMDNS), smokers (FMDS) and vapers (FMDV) were 9.4%±5.6%, 7.0%±5.5%, and 10.8%±6.2%, respectively. When corrected for artery caliber at rest as a covariate[13], adjusted values were FMDNS=10.1%, FMDS=8.9%, and FMDV=9.6% (Figure 4). In smokers, FMD showed a negative trend with the smoking exposure in terms of pack-years (r=-0.38, P>0.05). Reactive hyperemia peak velocity and blood acceleration (HI) trended lower (on average, -8% and -20%, respectively) in smokers and vapers, compared to nonsmokers, with HI difference in vapers vs nonsmokers approaching significance (P=0.05) only in males (Figure 5). No difference was found in pre-cuff occlusion SvO2 among the three groups, nor in washout time and overshoot, however, the upslope trended lower (-9%) in smokers, in agreement with an earlier study evaluating post-ischemic SvO2 in young and old smokers[14]. BHI was comparable between groups, however, in males only, BHI was higher in smokers than nonsmokers (P=0.03). Finally, aortic PWV trended higher (+10%) in smokers than in nonsmokers but did not differ between nonsmokers and vapers (Figure 4-5). Possible reasons for the absence of significant associations could be relatively low cumulative dose (especially for vapers), and possibly inadequate power. The results differ from those observed acutely comparing pre- and post-exposure[5-7]. Increased diastolic BP in vapers and smokers, compared to nonsmokers, might be associated with the smoking habits.Conclusions
Overall, the MRI metrics evaluating vascular function and tone did not differ significantly among the three groups in this limited study, likely because damage accumulation may take longer to elicit measurable effects on the endothelium.Acknowledgements
NIH Grant R01 HL139358References
[1]. Miech R, et al. N Engl J Med. 2019; 381:1490-1491. [2]. Wang P, et al. PloS one. 2017;12(1):e0169811. [3]. Williams M, et al. PloS one. 2017;12(4):e0175430. [4]. Goel R, et al. Chem Res Toxicol. 2015;28(9):1675-7. [5]. Carnevale R, et al. Chest. 2016;150(3):606-12. [6]. Caporale A, et al. Radiology. 2019;293(1):97-106. [7]. Münzel T, et al. Eur Heart J. 2020;41(41):4057-70. [8]. Magland JF, et al. Magn Res Med. 2016;75(1):257-65. [9]. Rosenberry R, Nelson MD. Am J Physiol-Reg Integr Comparat Physiol. 2020;318(3):R605-18. [10]. Langham MC, et al. Magn Reson Med. 2010;64:1599-606. [11]. Langham MC, et al. Magn Reson Med. 2011;65(3):750-5. [12]. Sader MA, Celermajer DS. Cardiovas research. 2002;53(3):597-604. [13]. Atkinson G, et al. J Hypertens. 2013;31(2):287-91. [14]. Langham MC, et al. J Cardiovasc Magn Reson. 2015;17(1):19.Figures
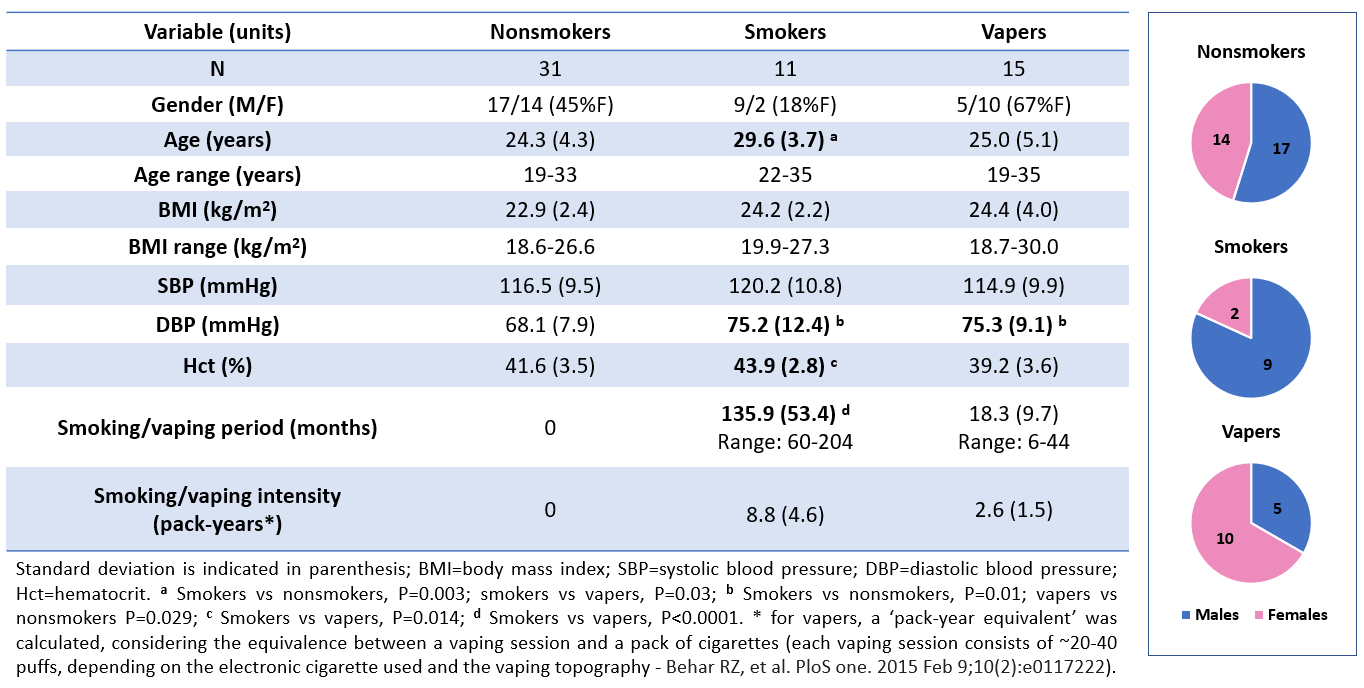
Figure 1 – Demographics, details on smoking/vaping history and exposure, and gender distribution in the three groups.
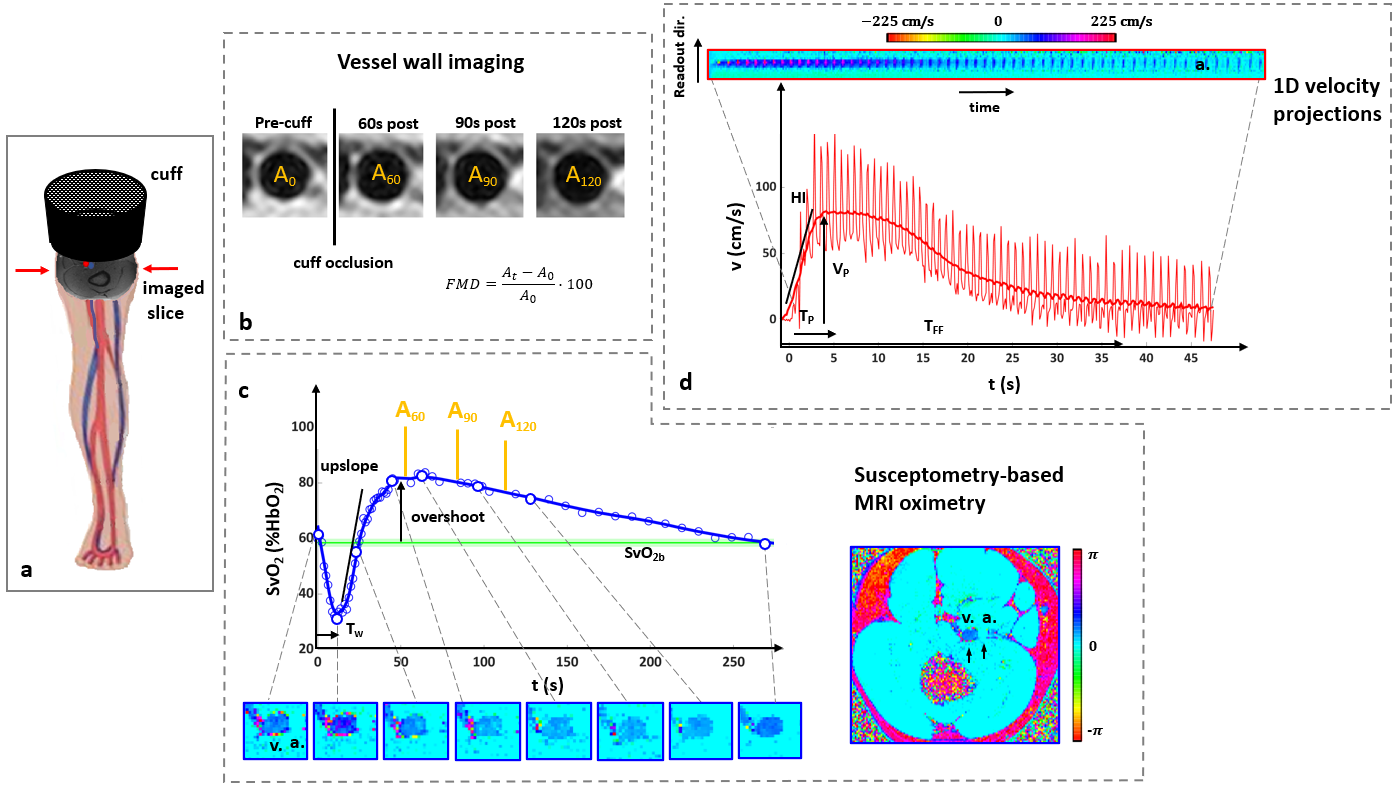
Figure 2 – A. The cuff is proximal to the superficial femoral artery and vein. B. Artery lumen (At) is measured before cuff-occlusion and post-cuff release, to evaluate flow mediated dilation. C. Venous saturation (SvO2) is measured continuously post-cuff release (acquisition is interrupted 3 times to measure At), using the phase difference between vein (v.) and artery (a.) (SvO2b=pre-cuff SvO2; Tw=washout time). D. Arterial blood flow velocity averaged across the artery lumen, plotted vs time. (VP=peak velocity; HI=blood acceleration; TP=time to peak; TFF=hyperemia duration).
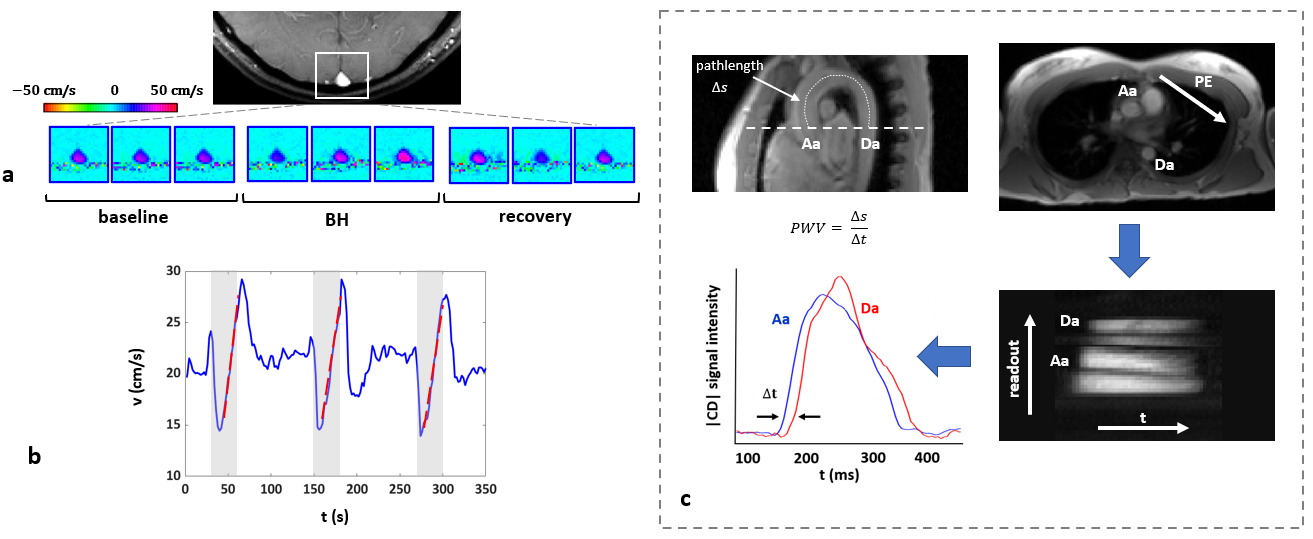
Figure 3 – A. Nine 2D velocity maps in the superior sagittal sinus are shown before, during and after the breath-hold (BH). B. The breath-hold index is the slope of the linear increase in velocity during BHs (gray areas). C. The pathlength of the pulse wave between ascending and descending aorta (Aa, Da) is indicated. Aa and Da are labeled in the axial image on the right (PE=phase encoding direction). From 1D velocity-sensitized projections the complex difference (CD) signal intensity is retrieved to determine the transit time (Δt). Pulse wave velocity (PWV) is then computed as Δs/Δt.
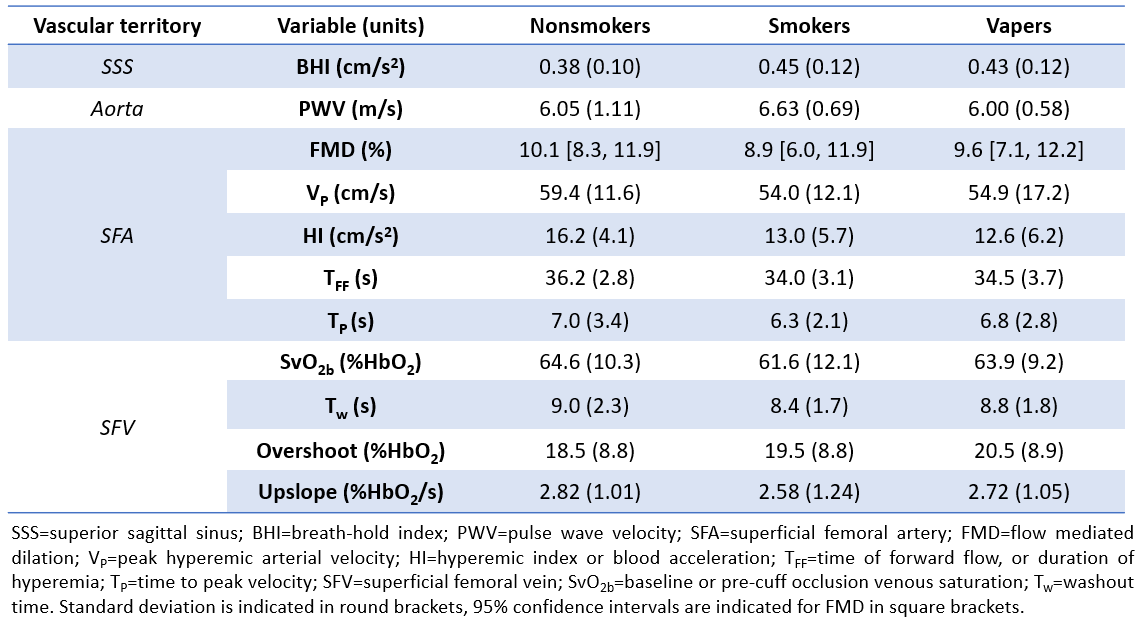
Figure 4 – MRI metrics quantified in each vascular territory for the three groups.
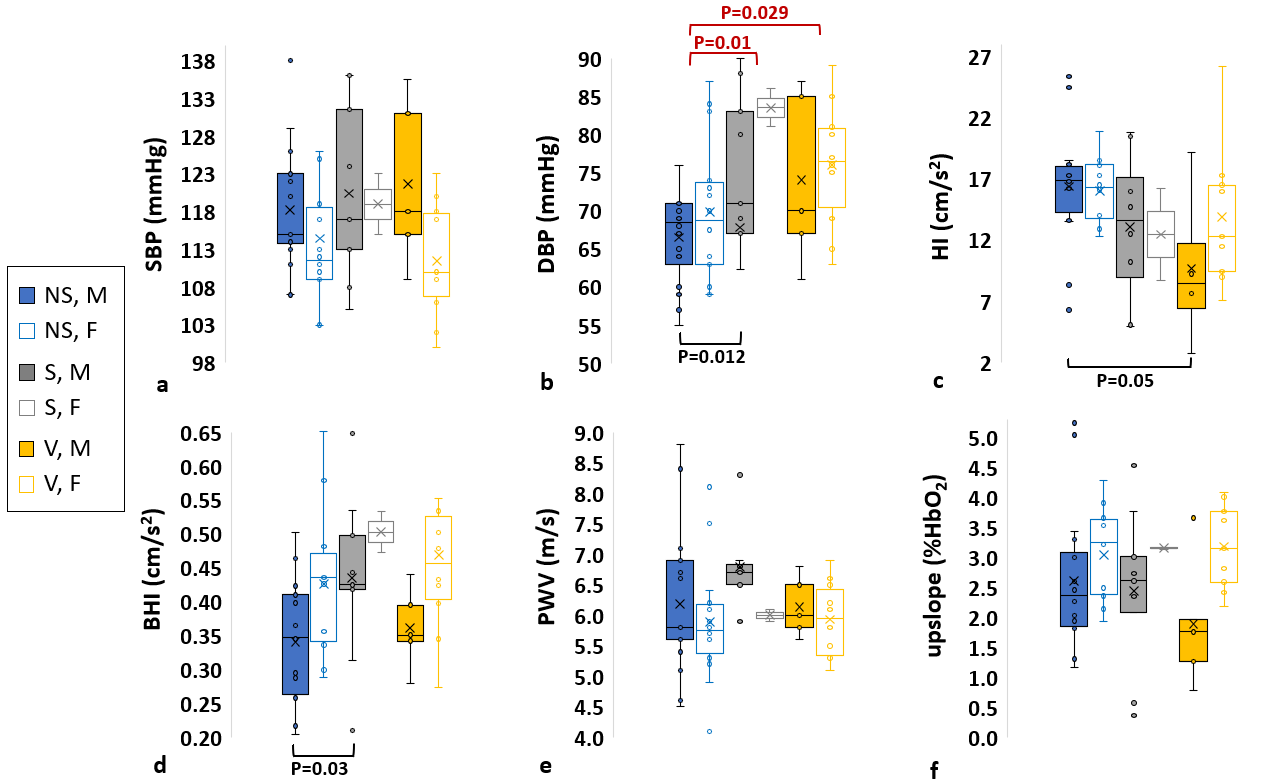
Figure 5 – Box and whisker plots showing the distributions of various parameters in nonsmokers (NS, control group), smokers (S) and vapers (V), differentiated by gender (M=males, F=females). P value is indicated for P≤0.05. Black horizontal bars denote significant associations between subgroups (for instance, male nonsmokers and smokers); red denotes significant associations between groups, pooling males, and females. SBP=systolic blood pressure; DBP=diastolic blood pressure; HI=hyperemic index; BHI=breath-hold index; PWV=pulse wave velocity.