1623
Planning-less REACT-MD: Fast and simple run-off exam of the total legs with simultaneous non-contrast MRA and black-blood imaging
Yutaka Hamatani1, Kayoko Abe2, Masami Yoneyama3, Christoph Katemann4, Shuo Zhang4, Yasuhiro Goto1, Michinobu Nagao2, Isao Shiina1, Kazuo Kodaira1, Takumi Ogawa1, Mamoru Takeyama1, Isao Tanaka1, and Shuji Sakai2
1Department of Radioligical Services, Tokyo Women's Medical University Hospital, Tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Tokyo Women's Medical University Hospital, Tokyo, Japan, 3Philips Japan, Tokyo, Japan, 4Philips Healthcare, Hamburg, Germany
1Department of Radioligical Services, Tokyo Women's Medical University Hospital, Tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Tokyo Women's Medical University Hospital, Tokyo, Japan, 3Philips Japan, Tokyo, Japan, 4Philips Healthcare, Hamburg, Germany
Synopsis
Magnetic resonance angiography (MRA) is essential to characterize luminal changes and detect abnormalities in peripheral vascular diseases. However, clear depiction of the vascular structures without contrast within a short scan time remains challenging and is often limited by complicated exam and long procedure time. In this study, we employ planning-less REACT-MD (Relaxation-Enhanced Angiography without Contrast and Triggering with Multiple Delays) with simultaneous non-contrast MRA and black-blood imaging for fast and simple run-off exams of the lower extremities without additional scout acquisition and volume planning, aiming to provide multi-contrast images with diagnostic quality and simplified clinical workflow.
Introduction
Depiction of vascular diseases throughout the lower limbs by MRI is useful for diagnosing both arterial and venous disease, such as arteriosclerosis of the lower limbs (ASO) and deep vein thrombosis (DVT). 1,2,3 Contrast-enhanced MRA is commonly used for evaluating arteries in the lower extremities, but non-contrast MRA is attracting attention instead of contrast-enhanced MRA recently.4,5,6 The recently introduced REACT-MD (Relaxation-Enhanced Angiography without Contrast and Triggering with Multiple Delays) technique provides the possibility of simultaneous non-contrast MRA and black-blood imaging. While the REACT part allows for flow-independent depiction of the vasculature with a large anatomical coverage without contrast, a multi-delay acquisition offers fat-suppressed MPRAGE-type images for detection of the vessel wall lesions in the same scan.7,8,9 In this study, we investigated the feasibility of using REACT-MD in run-off total leg imaging without additional scout acquisitions or volume planning for fast and simple clinical workflow.Methods
In short, the REACT-MD technique basically consists of two signal readouts by 3D Dixon dual-echo turbo field-echo (TFE) preceded by a T2prep pulse and a non-selective IR pulse. Magnetization preparation pulses were implemented to suppress signal from tissues such as muscles, nerves and organs, according to their difference in relaxation times. In detail, immediately after the T2prep pulse, an IR pulse was applied with a short inversion time (TI) to suppress tissues with short-to-intermediate T1 and T2, thus enhancing the blood-to-tissue contrast during the first signal readout for MRA. Thereafter, at the time of the blood null point, the second signal readout was carried out additionally to obtain the MPRAGE images. Consequently, REACT-MD provides MRA (phase-1) and MPRAGE (phase-2) images in one single scan without prolonging the total acquisition time. Scheme of the REACT-MD sequence is shown in Figure 1. Furthermore, we also applied 3D non-selective excitation pulses, which has already been demonstrated to improve the image quality of 3.0T bSSFP coronary MRA, and balanced-TFE DIXON.10,11 For feasibility test in volunteers, a fast planning-less run-off concept was used. The proposed approach is as follows: once the operator centers the laser indicator at the distal fibula of the patient on the scanner table, a run-off exam of the total leg automatically starts in the caudal to cranial direction with 4-station anatomical coverage. Each station has a 400 mm FOV with 120 mm overlap between the adjacent stations. In this manner, any survey or localization or scout scans and plans of the volume placement for the total legs prior to the run-off exam are no longer needed. In addition to this simple workflow, a rapid acquisition time of 1 minute per one station further accelerates the examination time. A comparison of the procedural time scheme using the proposed approach to the conventional method in the practice is shown in Figure 2. All scans were performed on a clinical 3.0T MRI system (Ingenia, Philips Healthcare). A total of five volunteers (4 men, 1 woman, age range 30 to 45) were examined. The study was approved by the local IRB, and written informed consent was obtained from all subjects. The acquired images were evaluated via visual inspection. Imaging parameters for planning-less total legs REACT-MD are shown in Table 1. [Table 1]Results and Discussion
Figure 3 shows representative total leg non-contrast MRA images from REACT-MD sequence from two volunteers using planning-less procedure. The visualization of blood vessels was stable overall from the pelvis to the foot in different volunteers. Representative full MIP and partial MIP of REACT MRA and MPRAGE images from the REACT-MD dataset using planning-less procedure are shown in Figure 4. REACT MRA clearly depicted the blood vessels from the pelvis to the foot with higher vessel-background contrast, and small vessels are also can be clearly seen. On the other hand, MPRAGE from REACT-MD provided black-blood images with uniform fat suppression from pelvis to foot as well. It is noteworthy that REACT-MD provided MRA and MPRAGE images in one single scan and allowed for imaging over a large FOV at 3.0T.Conclusion
We have demonstrated the feasibility of a fast and simple run-off exam of the total legs with simultaneous non-contrast MRA and black-blood imaging without scout acquisition and volume planning based on the REACT-MD method. The obtained diagnostic quality with multiple image contrasts and short scan time may lead to simplified workflow in patients with peripheral vascular diseases. Further studies are needed to assess its clinical performance.Acknowledgements
No acknowledgement found.References
1. Cambria RP, et al. Magnetic resonance angiography in the management of lower extremity arterial occlusive disease : a prospective study. J Vasc Surg. 1997 Feb; 25(2):380-9. 2. Owada A, et al. MRA imaging of arterial patency in undialyzed uremic patients with arteriosclerosis obliterans. Ren Fail. 1995 Nov;17(6):743-50. 3. Weiss KJ, et al. Feasibility and Robustness of 3T Magnetic Resonance Angiography Using Modified Dixon Fat Suppression in Patients With Known or Suspected Peripheral Artery Disease. Front Cardiovasc Med. 2020 Oct 30;7:549392. doi: 10.3389/fcvm.2020.549392. eCollection 2020. 4. Yao-Kuang Huang, et al. Evaluation of venous pathology of the lower extremities with triggered angiography non-contrast-enhanced magnetic resonance imaging. BMC Med Imaging . 2019 Dec 17;19(1):96. 5. Schubert T, et al. Non-enhanced, ECG-gated MR angiography of the pedal vasculature: comparison with contrast-enhanced MR angiography and digital subtraction angiography in peripheral arterial occlusive disease. European Radiology August 2016, Volume 26, Issue 8, pp 2705–2713 6. Zhang L, et al. Non contrast MRA of pedal arteries in type II diabetes: effect of disease load on vessel visibility. Acad Radiol. 2015 Apr; 22(4):513-9. 7. Yoneyama M, et al. Free-breathing non-contrast-enhanced flow-independent MR angiography using magnetization-prepared 3D non-balanced dual-echo Dixon method: A feasibility study at 3 Tesla. Magnetic Resonance Imaging 2019 Aug 16;63:137-146 8. Yoneyama M, et al. REACT-MD: simultaneous non-contrast-enhanced subclavian MRA and fat suppressed direct thrombus imaging (MPRAGE) with a large field-of-view. Proc. ISMRM:2020.1320 9. Hamatani Y, et al. Improved visualization of non-contrast-enhanced MRA of the foot using REACT with balanced SSFP-DIXON (bREACT) at 1.5T. Proc. ISMRM:2020.2159 10. Kodaira K, et al. Acceleration of whole-heart coronary MR angiography using 3D non-selective bSSFP with Compressed SENSE. Proc. ISMRM:2019.2063 11. Shiina I, et al. Whole heart coronary MRA using non-selective balanced SSFP sequence at 3.0T: comparison of image quality. Proc. ISMRM:2019.2073Figures
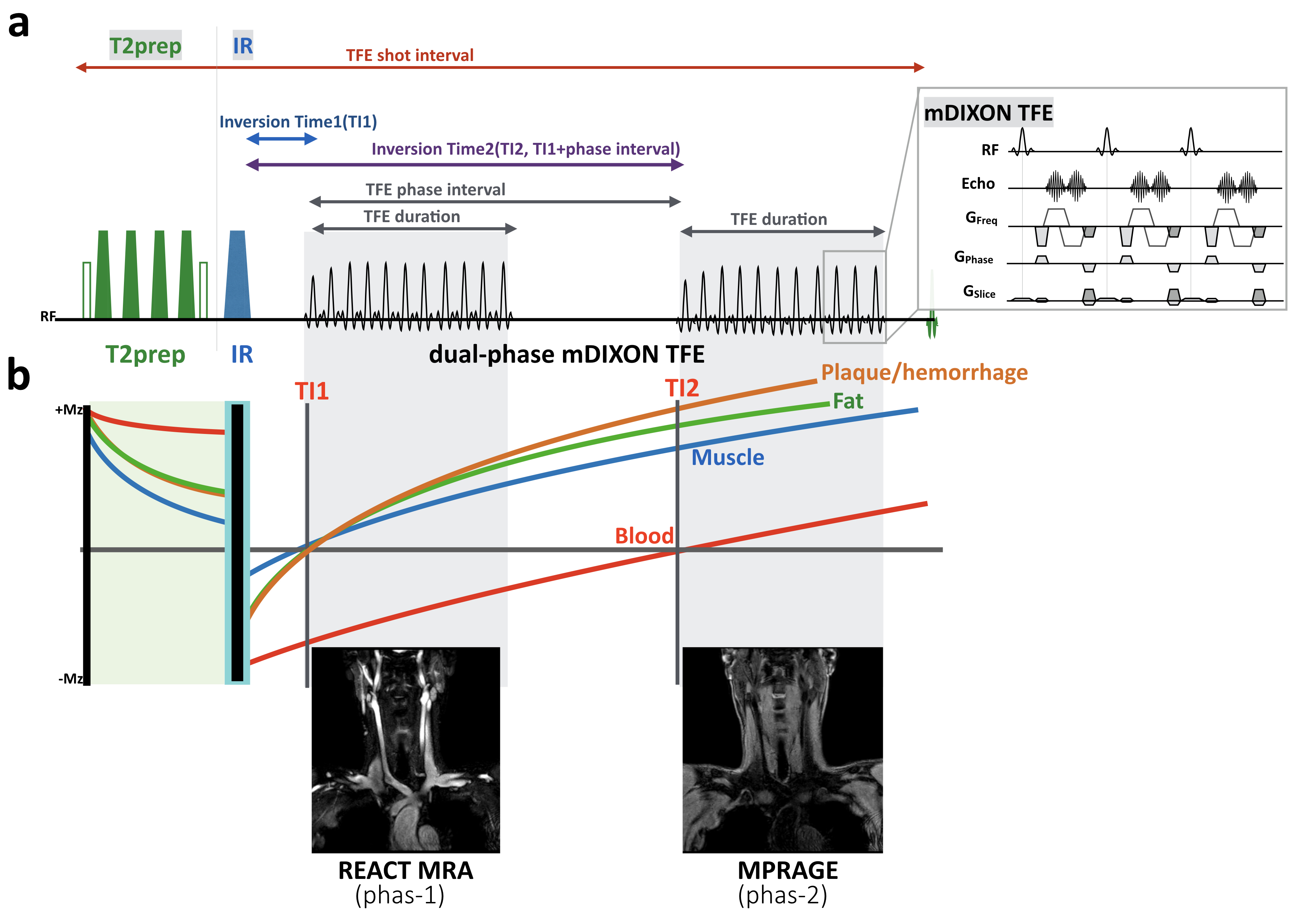
Figure 1. Scheme
overview of REACT-MD sequence.
REACT
consisting of a 3D DIXON-TFE with T2prep and IR pulse (a). Immediately after
the T2prep pulse, an IR pulse was applied with a short TI to suppress muscle
and fat (b). REACT-MD employs an additional DIXON-TFE shot at the timing with
the null point of the blood (a). REACT-MD provides MRA (phase-1) and MPRAGE
(phase-2) images in one single scan.
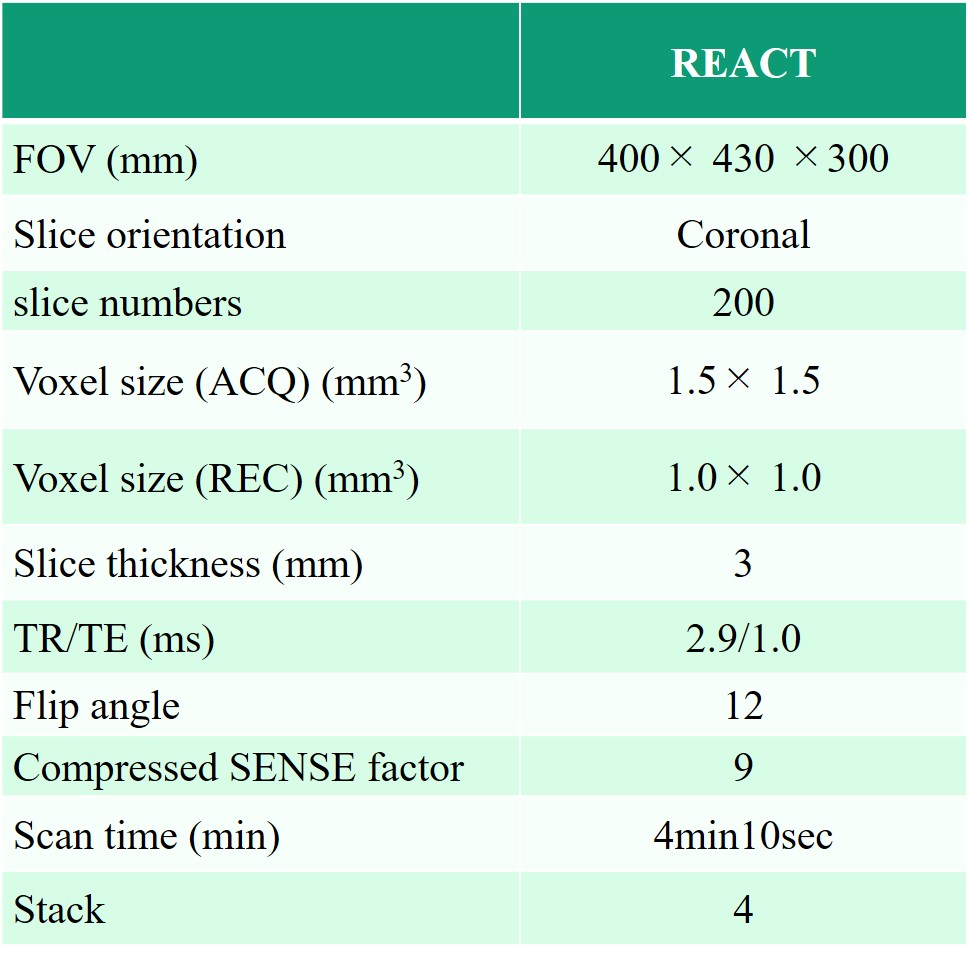
Table 1. The imaging parameter of Planning
less lower limb MRA with REACT
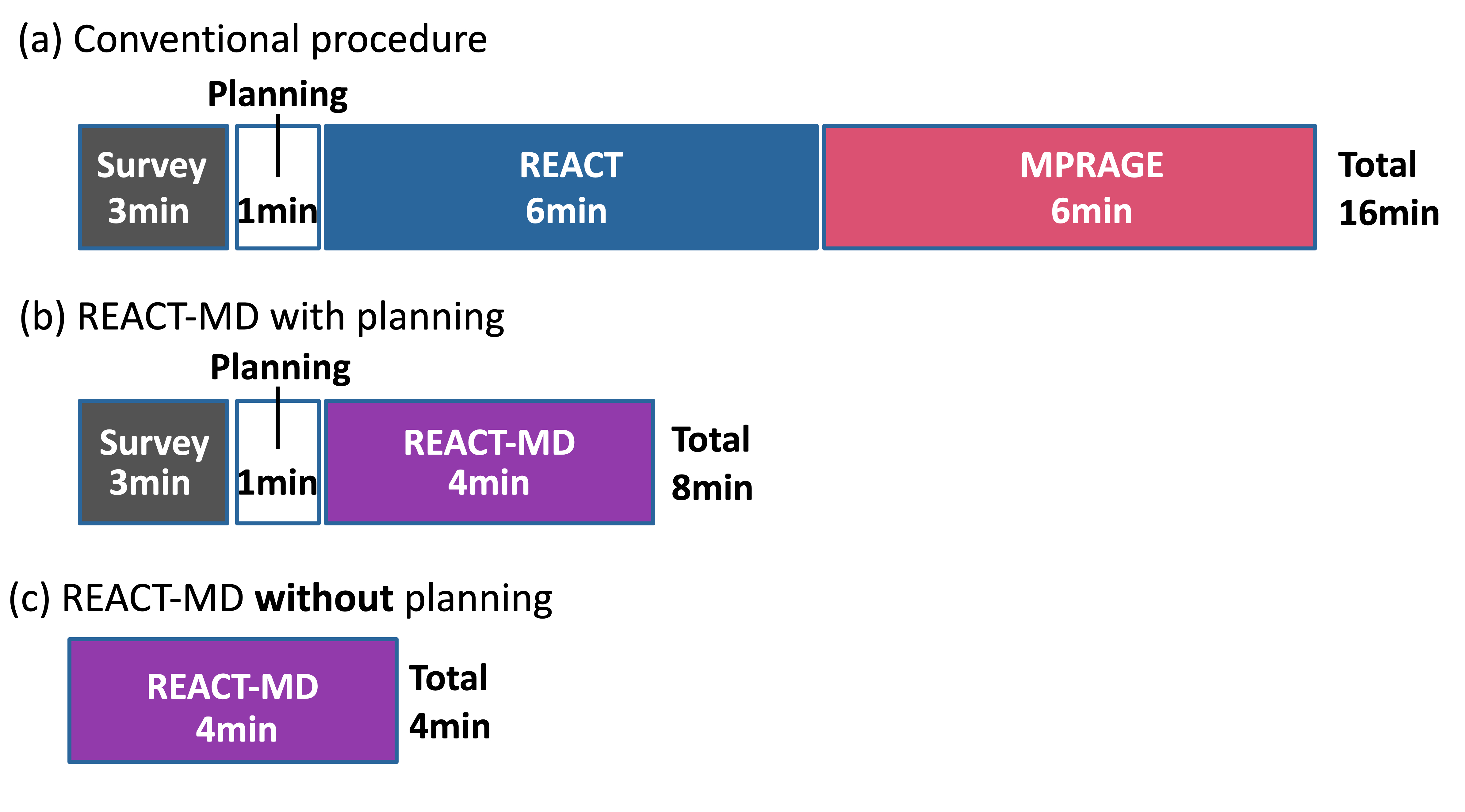
Figure 2.
A
comparison of the procedural time scheme using the proposed approach to the
conventional method in the practice. (a) conventional procedure included
survey, planning and separate scans for REACT and MPRAGE images. REACT-MD can
shorten the scan time for REACT and MPRAGE (b). Furthermore, fast planning-less
approach (c) further reducing the total examination time.
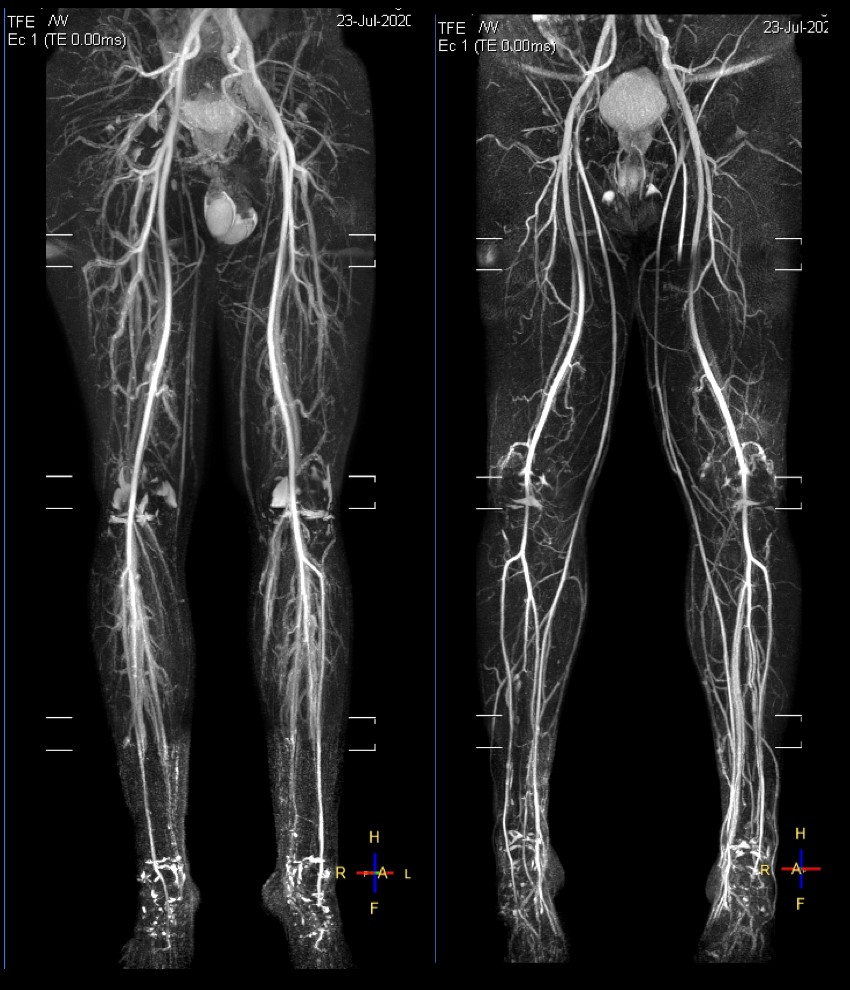
Figure 3.
Representative
total leg non-contrast MRA images from REACT-MD sequence from two volunteers.
The visualization of blood vessels was stable overall from the pelvis to the
foot.
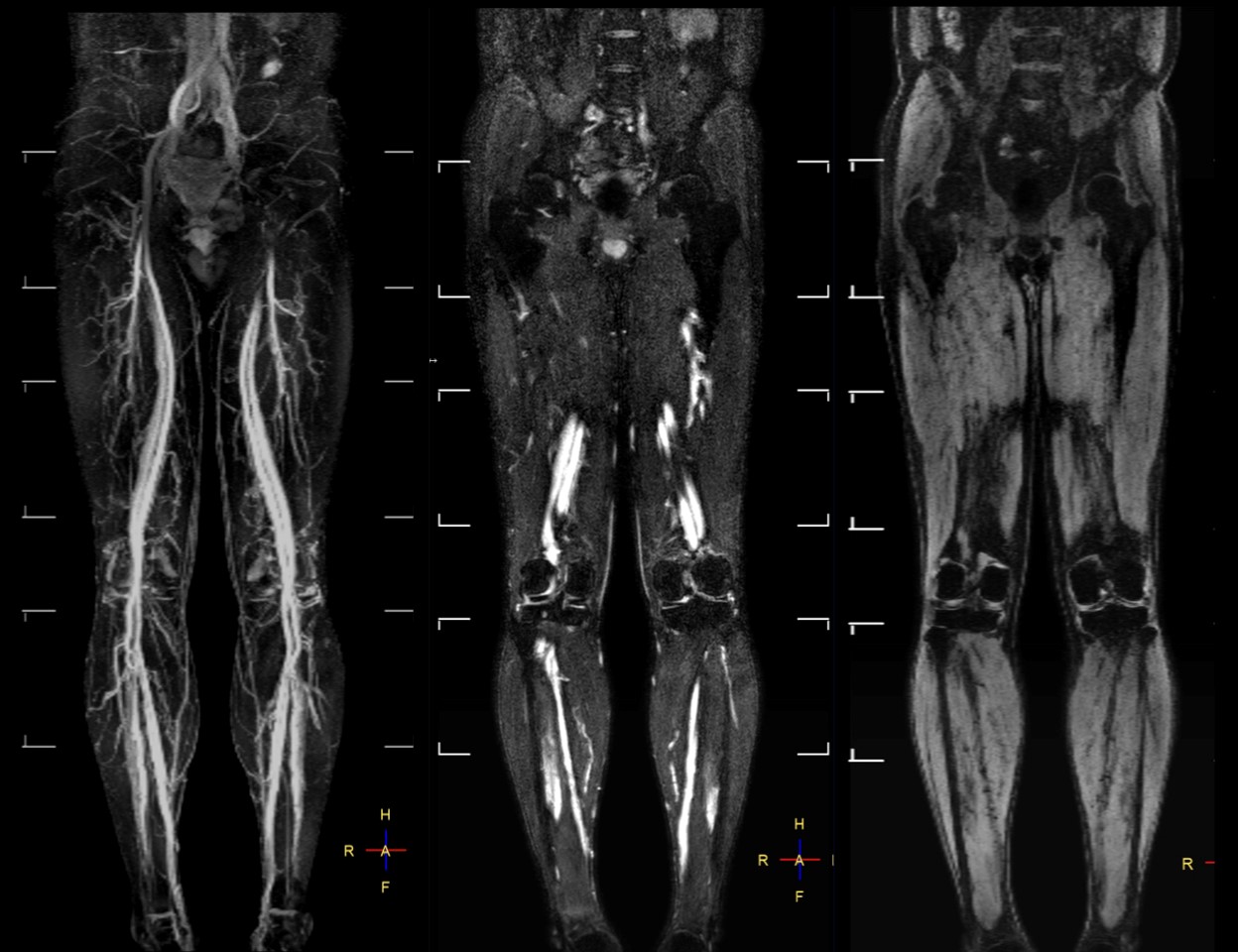
Figure 4.
Representative full MIP (left) partial MIP (center) of
REACT-MRA and MPRAGE (right) images from the same REACT-MD dataset. It is
noteworthy that REACT-MD provided both MRA and MPRAGE images in one single scan
and allowed for imaging over a large FOV at 3.0T.