1622
Non-contrast high-resolution 4D-peripheral MRA using Retrospective EPI
Yasuhiro Goto1, Michinobu Nagao1, Masami Yoneyama2, Yasutomo Katsumata2, Isao Shiina1, Kazuo Kodaira1, Yutaka Hamatani1, Takumi Ogawa1, Mamoru Takeyama1, Isao Tanaka1, and Shuji Sakai1
1Women's Medical University Hospital, tokyo, Japan, 2Philips Japan, tokyo, Japan
1Women's Medical University Hospital, tokyo, Japan, 2Philips Japan, tokyo, Japan
Synopsis
We investigated whether non-contrast, high resolution PPU-triggered 4D-peripheral MRA using Retrospective EPI (REPI). REPI 4D-peripheral MRA with VENC of 10 cm/s showed higher vascular conspicuity compared with the conventional methods.
Introduction
Peripheral Arterial Disease (PAD) is a painful disease due to poor blood flow in the peripheral arteries of the feet and hands. Early detection and early diagnosis are important to prevent complications without aggravating PAD. It is very important to determine the level of occlusion of peripheral arteries, especially to preserve the toes and ankles.MR Digital Subtraction Angiography (MR-DSA) using contrast media is the most established method [1]. However, it is difficult to use contrast media because diabetics often have renal impairment. Non-contrast MRA techniques have some limitations in its application to foot MRA in terms of image quality and acquisition time [2]. Recently, we have introduced the usefulness of REACT in visualization of peripheral blood vessels [3]. However, since REACT takes advantage of the difference in relaxation time, it depicts not only arterial signals but also venous signals. Other current existing non-contrast MRA methods such as TOF and phase contrast (PC) MRA in visualization of peripheral arteries; for instance, PC-MRA has complicated procedure for operators because the we must find the exact trigger delay in advance for obtaining artery images, and acquisition time is often long. To solve these problems, we focused on the peripheral pulse (PPU) triggered Retrospective EPI (REPI) 4D-FLOW based on quantitative flow sequence [4] (Figure 1). Since REPI sequence is based on EPI, it allows shorter scan time compared with conventional 4D FLOW sequence. Also this sequence utilizes the acquisitions during all cardiac cycles, complicated procedure is not needed. We investigated the feasibility of high-resolution peripheral angiographic non-contrast MRA using this pulse wave-gated REPI 4D-MRA.Methods
[Subjects] A total of six volunteers (4 men, 2 woman, age range 22 to 46) were examined on a 3.0T MRI (Ingenia, Philips Healthcare). The study was approved by the local IRB, and written informed consent was obtained from all subjects. [Imaging quality assessment] To examine the usefulness of foot REPI, the evaluation of proximal to distal vessels was segmented with joints as the border. (Figure 2.)The blood vessels of the peripheral arteries of the foot were evaluated on a 5-point scale. Three radiologists visually evaluated the blood vessels in the foot. 1) Optimize the scan parameters of REPI 4D-MRA: The following parameters were evaluated; VENC: 10cm/s ,20cm/s ,30cm/s ,40cm/s ,50cm/s . 2) Image quality was compared for peripheral arterial visualization for 3D-PCA, TFE-4D-MRA, and REPI-4D-MRA. [Statistical analysis] Statistical analysis was performed on the VENC of REPI 4D-MRA by the Steel-Dwass test, and it was judged that there was a significant difference when p <0.05. [scan parameter] REPI: FOV (mm) = 180×180, spatial resolution (mm) = 1.2×1.2×1.5, TR/TE (ms) = 9.2/5.3, flip angle (° ) = 10, SENSE factor = 3, TFE-factor=3, EPI-factor=5, Recon heart phase = 15, acquisition time = 3m53s. TFE: FOV (mm) = 180×180, spatial resolution (mm) = 1.2×1.4×1.5, TR/TE (ms) = 9.8/6.2, flip angle (° ) = 10, SENSE factor = 3, TFE-factor=5, Recon heart phase = 8, acquisition time = 5m10s. 3D-PCA: FOV (mm) = 180×180, spatial resolution (mm) = 1.2×1.2×1.5, TR/TE (ms) = 9.6/5.7, flip angle (° ) = 15, SENSE factor = 3, acquisition time = 5m56s. 2D-TOF: FOV (mm) = 180×180, spatial resolution (mm) = 1.2×1.2×4.0, TR/TE (ms) = 16/3.5, flip angle (° ) = 15, SENSE factor = 3, acquisition time = 5m19s.Results & Discussion
1) Visual evaluation of VENC. REPI with VENC=10cm/s scored higher in all areas compared to other VENCs, clearly visualized peripheral vascular structures. Therefore, the optimal VENC for visualizing peripheral arteries in the REPI 4D-MRA sequence was 10cm/s. 2) Comparison of sequences methods. REACT, which can visualize peripheral arteries and veins to the periphery, was used as a reference for degree of blood vessel depiction. In AREA1, there was no significant difference in all the methods compared. In AREA2, 3 and 4, REPI significantly better visualized vascular structure compared to the other three methods. Compared with REPI and TFE, REPI shortened acquisition time and showed high vascular imaging ability. Compared with REPI and 3D-PCA, 3D-PCA images according to the systole of the cardiac cycle, so only one image during systole is imaged. REPI continuously images all cardiac cycles, it acquires 8 images with one R-R interval. Therefore, we have less time to search for systole for imaging, which makes it simpler. REPI can cumulate all images of the cardiac cycle (cumulation image). Compared with REPI, TOF strongly depends on the direction of flow, but REPI can depict blood vessels independently of the direction of flow.Conclusion
REPI with VENC 10 cm/s well depicted peripheral arteries clearly in a short time. It might be extended for other body parts such as abdominal MRA.Acknowledgements
No acknowledgement found.References
(1)Cambria RP, et al. Magnetic resonance angiography in the management of lower extremity arterial occlusive disease : a prospective study. J Vasc Surg. 1997 Feb;25(2):380-9. (2)Zhang L, et al. Non contrast MRA of pedal arteries in type II diabetes: effect of disease load on vessel visibility. Acad Radiol. 2015 Apr;22(4):513-9. (3) Hamatani Y ,et.al, ISMRM Virtual Conference & Exhibition, 2020.(Abstract2020). (4) Pankaj G, et al. Comparison of fast acquisition strategies in whole-heart four-dimensional flow cardiac MR: Two-center, 1.5 Tesla, phantom and in vivo validation study. J Magn Reson Imaging.2018 Jan;47(1):272-281.Figures
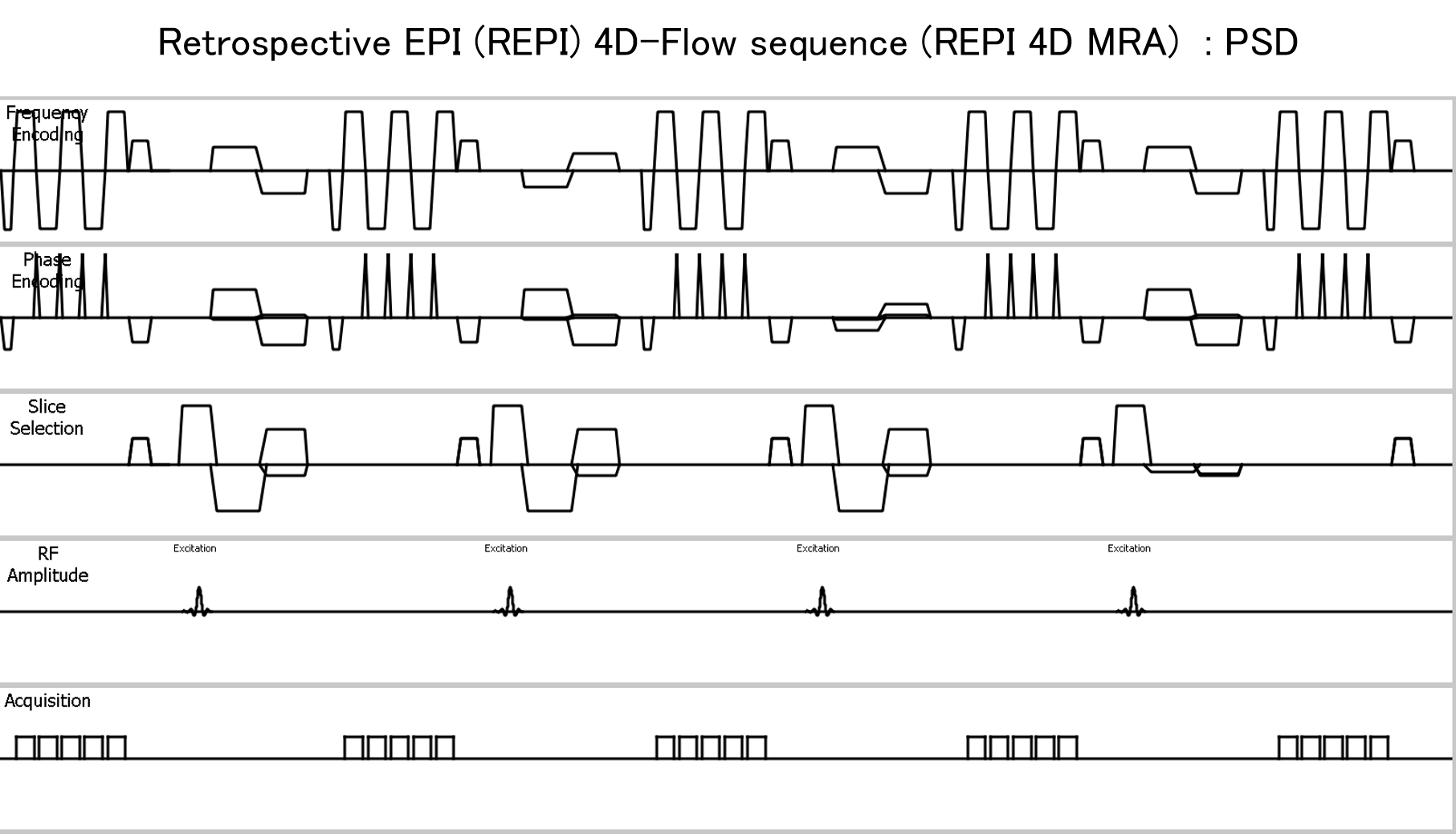
Figure 1. Scheme
of
the REPI 4D MRA sequence
TFEPI sequence is being combined with EPI
readout, it is capable of scan time acceleration and improves SNR.
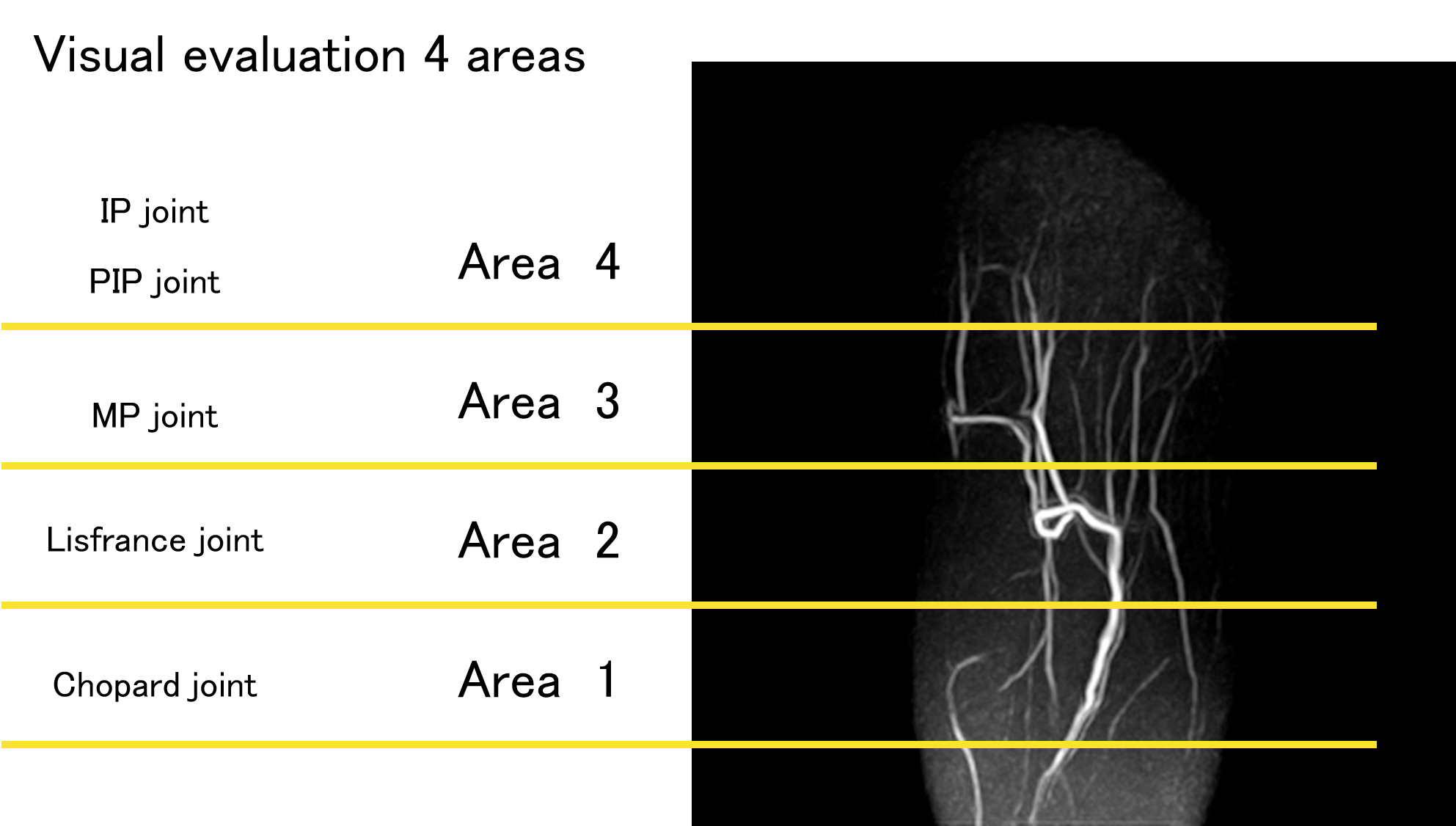
Figure 2. Visual assessment of peripheral vessels of the foot. The visual assessment was divided into four areas with the joint as a boundary, and each was
evaluated for the depiction of blood vessels. Area 1 : Chopard joint - Lisfranc joint, Area 2 : Lisfranc joint - MP joint, Area 3 : MP
joint - IP joint, PIP joint, Area 4 : IP joint, PIP joint - Distal.
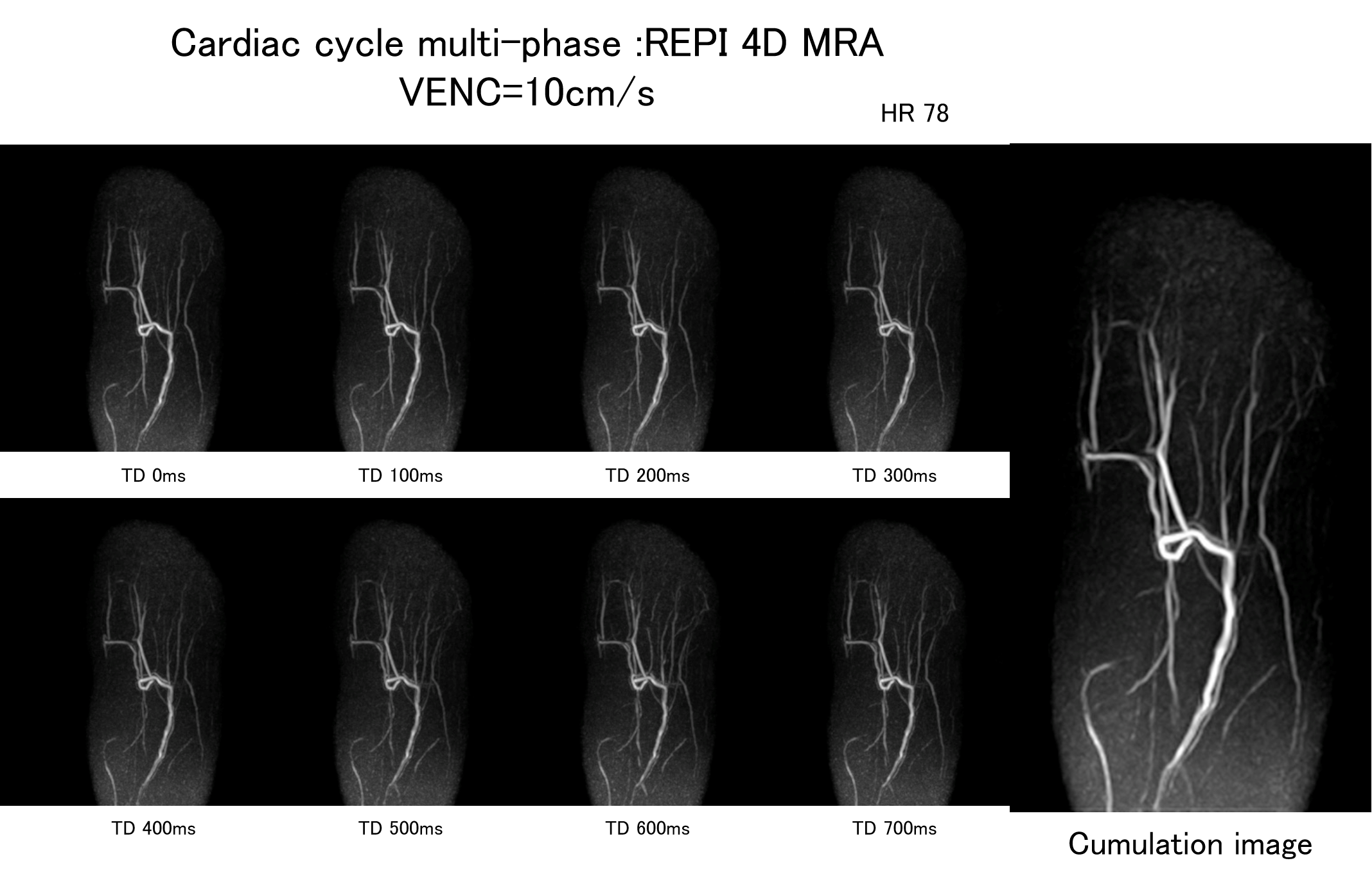
Figure 3. Peripheral vessels of the foot. REPI continuously images all cardiac
cycles, it collects 8 phases with 1R-R. REPI can cumulate all images throughout
the cardiac cycle. (Cumulation image)
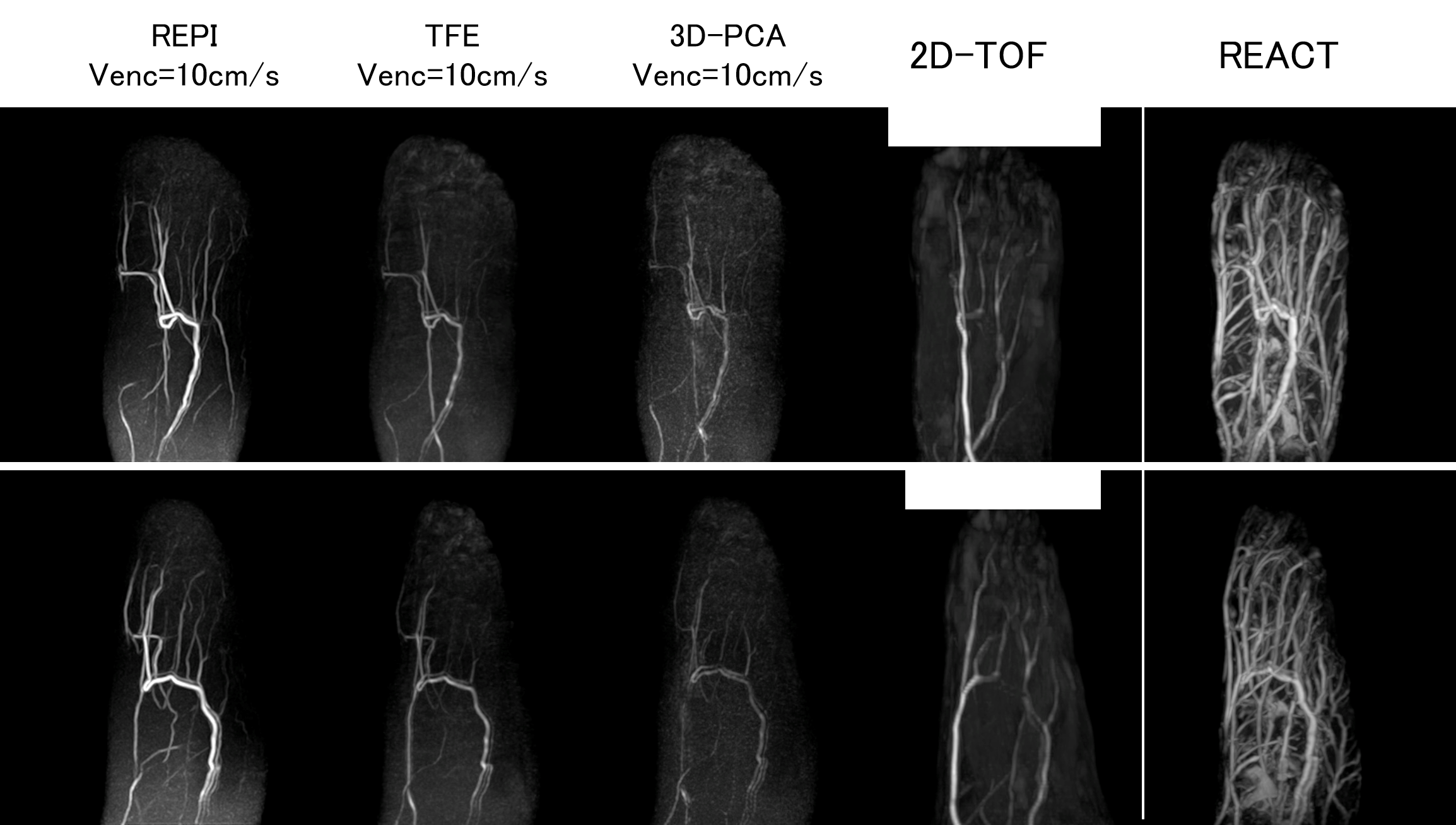
Figure 4. Peripheral vessels of the foot. REPI VENC=10cm/s, TFE VENC=10cm/s, 3D-PCA VENC=10cm/s, 2D-TOF used for comparison. REPI 4D-MRA significantly improves
vascular structure in AREA2,3,4, compared with the other three methods.
Visualized.
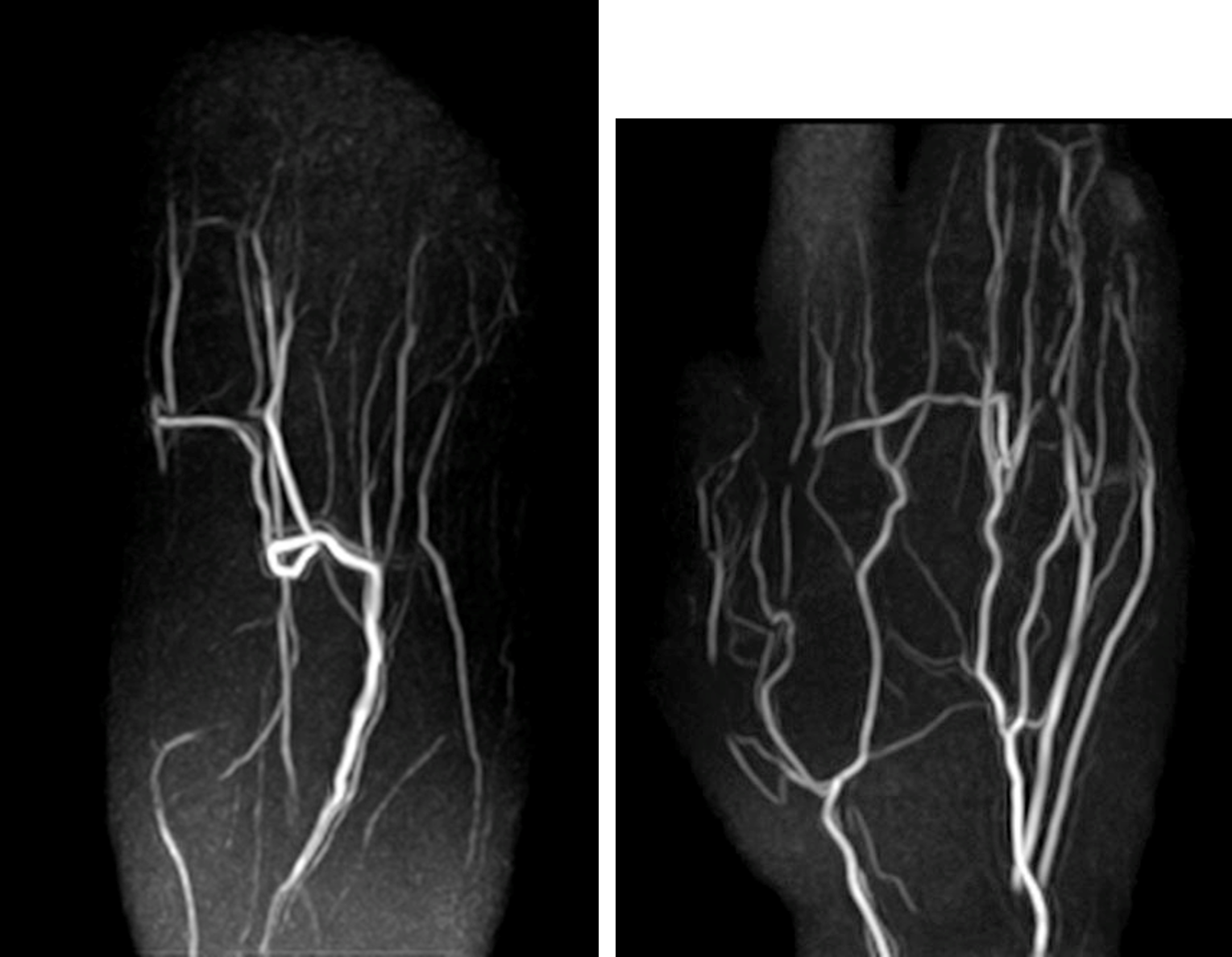
Figure 5. Representative REPI 4D MRA of the foot (left) and the hand (right). REPI 4D MRA could visualize blood vessels from proximal to distal with high
robustness. The optimal VENC for visualizing peripheral blood vessels was 10cm/s.