1621
Comparison of 2D and 3D Quiescent Interval Slice-Selective Non-Contrast MR Angiography in Patients with Peripheral Artery Disease1Department of Radiology and Radiological Science, Medical University of South Carolina, Charleston, SC, United States, 2Northwestern University, Chicago, IL, United States, 3Department of Medicine, Medical University of South Carolina, Charleston, SC, United States, 4Department of Radiology, Northshore University HealthSystem, Evanston, IL, United States
Synopsis
2D quiescent-interval slice-selective (QISS) MRA is an established technique in peripheral artery disease (PAD), however, its slice thickness is inferior to that used for computed tomography angiography (CTA). The prototype thin-slab stack-of-stars (tsSOS) QISS technique achieves CTA-like slice thickness. In this three-center study, we compared 2D-QISS and tsSOS-QISS MRA for the detection PAD in 23 patients. Overall image quality was not different between tsSOS-QISS and 2D-QISS. AUCs for PAD detection were not statistically different between the techniques (P=0.336). Our results indicate that 3D tsSOS-QISS provides similar accuracy in patients with PAD to a standard commercially available 2D-QISS technique.
Introduction
2D quiescent-interval slice-selective (QISS) MRA using a balanced steady-state free-precession readout1 is a commercially available non-contrast MRA technique that has been shown to provide diagnostic accuracy for peripheral artery disease (PAD) similar to that of computed tomography angiography (CTA).2-4 However, the 2D-QISS MRA technique uses a slice thickness on the order of 2 to 3mm that is thicker than that used for CTA (1 to 1.5mm). In order to obtain thinner slices while preserving image quality, a thin-slab stack-of-stars (tsSOS) 3D QISS MRA technique5 has been proposed that uses multiple thin slabs to ensure adequate inflow of unsaturated spins during the quiescent interval. However, it is unclear whether improved spatial resolution provides a significant benefit for the evaluation of PAD. Therefore, our aim was to compare 2D-QISS and tsSOS-QISS MRA for the detection of significant vascular stenosis in PAD patients, using CTA as the reference.Methods
Twenty-three patients (70±8 years, 18 men) who had previously undergone lower extremity CTA for the evaluation of PAD were prospectively enrolled between June 2019 and May 2020 in this IRB approved, three-center study. All patients underwent standard 2D-QISS MRA (field of view 400×260; voxel size 1.0×1.0×3.0; TE/TR 1.4/3.5ms; flip 90°; bandwidth 658Hz/pixel; and Cartesian K-space trajectory), and prototype 3D tsSOS-QISS MRA (field of view 334×334; voxel size 1.0×1.0×1.4; TE/TR 2.2/4.3ms; flip 60°; bandwidth 919Hz/pixel; and radial stack-of-stars K-space trajectory) on 1.5T MRI systems (MAGNETOM Avanto and Aera, Siemens). 2D-QISS MRA was acquired in 10 consecutive stations, 40×3mm-thick sections each, withinspiratory breath-holds at the upper pelvis and abdominal regions. Using 3D tsSOS-QISS MRA, the same z-axis length was covered by 10 stations with 14 thin slabs that consisted of 18×1.4mm-thick (interpolated to 36×0.7mm-thick) slice for each. tsSOS-QISS images were collected without breath-holds. Subjective image quality assessment of QISS MRA datasets was performed by three independent readers. Per-segment image quality was rated by each reader on a 4-point Likert-scale according to an 18-segment model. To determine the impact of acquiring thin slices on visualization of small vessels, a single observer performed a qualitative analysis of primary branch vessels sharpness on a 4-point scale. MRA and CTA datasets were evaluated for the detection of ≥50% intraluminal diameter stenosis on a per-segment basis using the same 18-segment model. Sensitivity, specificity and accuracy were calculated per segment.Results
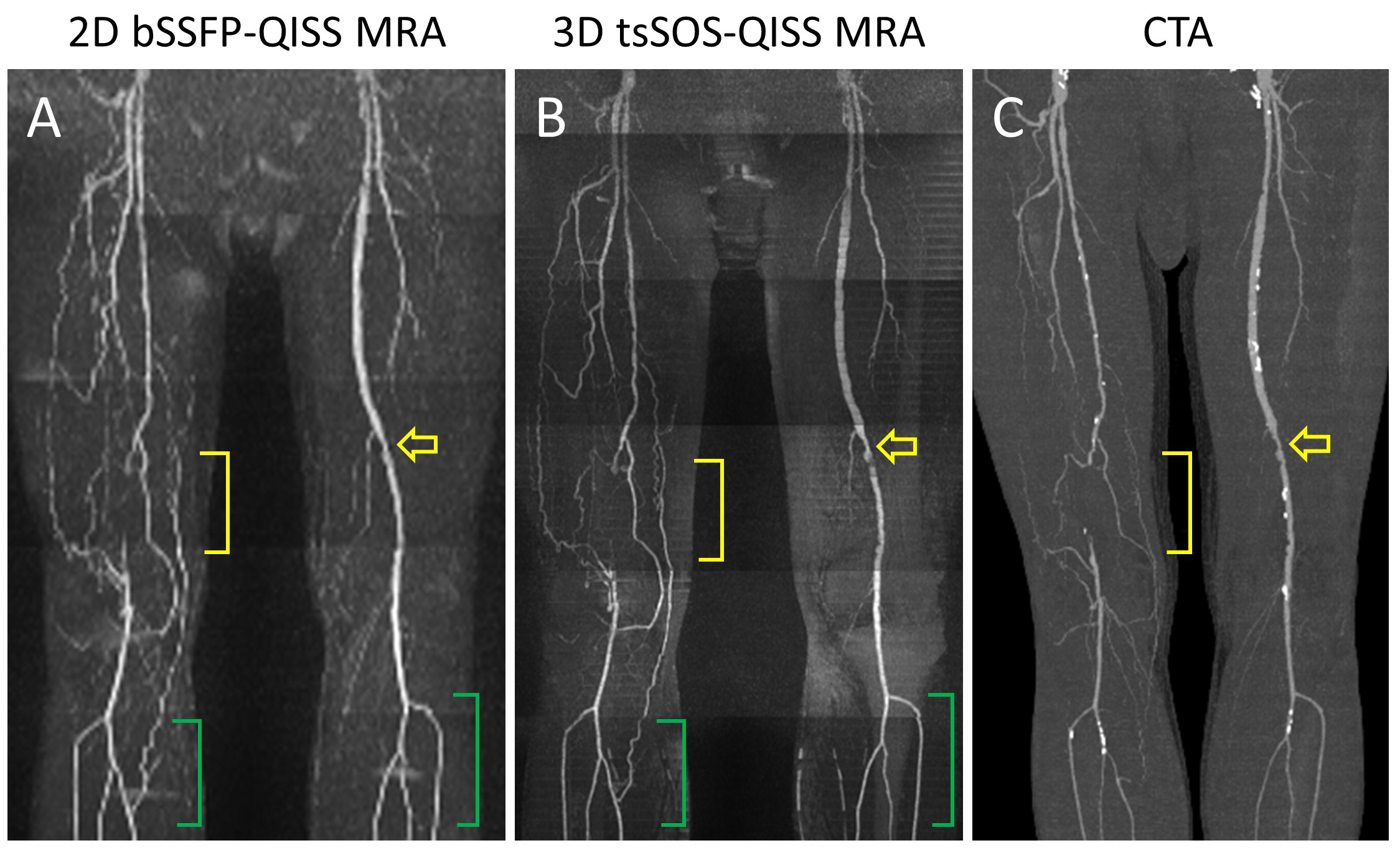
A total of 378 segments were evaluated. Overall subjective image quality ratings were not different between 2D and tsSOS-QISS MRA (4.0 [3.0; 4.0] vs 3.0 [3.0; 4.0], respectively; P=0.813). Good to excellent inter-reader agreement was observed for all regions and for the entire run-off (κ 0.62–0.83). Inter-modality agreement for image quality ratings was good (all κ>0.66) between the MRA techniques. Qualitative evaluation of the primary branch vessels demonstrated that tsSOS-QISS showed significantly improved image quality compared with standard 2D-QISS (4.0 [3.0; 4.0] vs 3.0 [2.0; 3.0], P=0.008). Stair-step artifacts were minimal or absent and vessel margins were better delineated with tsSOS-QISS (Figure 1). Overall sensitivity, specificity and AUC for the detection of significant vascular stenosis by 2D-QISS (83.0%, 88.2%, and 0.856, respectively) and tsSOS-QISS MRA (86.5%, 88.7%, and 0.877, respectively) were similar with no statistical difference between the AUCs (P=0.336).Discussion
This study provides the first validation that a multiple overlapping thin-slab 3D QISS technique can accurately evaluate peripheral vasculature in patients with PAD. Overall sensitivity, specificity and AUC for the detection of significant vascular stenosis were similar for the standard 2D-QISS and prototype 3D tsSOS-QISS approaches. Whereas diagnostic performance for the two techniques was similar for the main trunks of the peripheral arteries, qualitative analysis demonstrated that stair-step artifacts were reduced, and vessel margins more sharply demonstrated in the primary branch vessels using the thin-slice 3D tsSOS-QISS approach. Our study suggests that the clinical benefit of the improved through-plane spatial resolution is insignificant for the larger main trunks of the peripheral arteries, which predominantly have a cephalo-caudal orientation. Moreover, the use of thin slices is not likely to be of great benefit for long-segment stenoses or occlusions that are commonly present in PAD. On the other hand, for obliquely directed small-caliber vessels such as the renal arteries, one can anticipate that the 3D approach should offer significant benefits.5 In addition to providing validation for the 3D tsSOS-QISS technique, our results suggest that the use of relatively thick slices for 2D-QISS, while theoretically undesirable, does not represent a clinically significant limitation of the technique for the evaluation of PAD. Consequently, given the longer scan time of tsSOS-QISS5, our results suggest that 2D-QISS should remain a preferred approach for non-contrast MRA. tsSOS-QISS may have potential utility as a supplementary technique, e.g., for targeting specific vessel segments when improved slice resolution is needed, or to allow the free-breathing evaluation of vessel segments in the abdomen and upper pelvis in patients who cannot adequately breath-hold for 2D-QISS.Conclusion
The prototype 3D tsSOS-QISS technique provides similar accuracy in patients with PAD to a standard commercially available 2D-QISS technique. However, image quality for branch vessel depiction is improved using the 3D approach.Acknowledgements
N/AReferences
1. Edelman RR, Sheehan JJ, Dunkle E, Schindler N, Carr J and Koktzoglou I. Quiescent-interval single-shot unenhanced magnetic resonance angiography of peripheral vascular disease: Technical considerations and clinical feasibility. Magnetic resonance in medicine : official journal of the Society of Magnetic Resonance in Medicine / Society of Magnetic Resonance in Medicine. 2010;63:951-8.
2. Varga-Szemes A, Wichmann JL, Schoepf UJ, Suranyi P, De Cecco CN, Muscogiuri G, Caruso D, Yamada RT, Litwin SE, Tesche C, Duguay TM, Giri S, Vliegenthart R and Todoran TM. Accuracy of Noncontrast Quiescent-Interval Single-Shot Lower Extremity MR Angiography Versus CT Angiography for Diagnosis of Peripheral Artery Disease: Comparison With Digital Subtraction Angiography. JACC Cardiovasc Imaging. 2017;10:1116-1124.
3. Wu G, Yang J, Zhang T, Morelli JN, Giri S, Li X and Tang W. The diagnostic value of non-contrast enhanced quiescent interval single shot (QISS) magnetic resonance angiography at 3T for lower extremity peripheral arterial disease, in comparison to CT angiography. J Cardiovasc Magn Reson. 2016;18:71.
4. Varga-Szemes A, Aherne EA, Schoepf UJ, Todoran TM, Koktzoglou I and Edelman RR. Free-Breathing Fast Low-Angle Shot Quiescent-Interval Slice-Selective Magnetic Resonance Angiography for Improved Detection of Vascular Stenoses in the Pelvis and Abdomen: Technical Development. Investigative radiology. 2019;54:752-756.
5. Edelman RR, Aherne E, Leloudas N, Pang J and Koktzoglou I. Near-isotropic noncontrast MRA of the renal and peripheral arteries using a thin-slab stack-of-stars quiescent interval slice-selective acquisition. Magnetic resonance in medicine : official journal of the Society of Magnetic Resonance in Medicine / Society of Magnetic Resonance in Medicine. 2020;83:1711-1720.
Figures