1618
Contrast enhancement DISCO magnetic resonance angiography in preoperative assessment of anterolateral thigh flap1shandong university, Jinan, China, 2GE Healthcare, Beijing, China
Synopsis
Anterolateral thigh (ALT) flap has been widely used in reconstructive surgery for head and neck region and the extremities. However, the difficulties during the dissection of this flap were often associated with various vascular anatomies and frequent intramuscular course of perforators [1]. In this study, using a novel differential subsampling with cartesian ordering (DISCO) contrast enhancement magnetic resonance angiography, the patterns of lateral circumflex femoral artery and its branches were clearly identified, and were consistent with operative findings. Therefore, DISCO imaging can be an accurate and compatible method for perforators imaging preoperatively prior to ALT flaps.
Introducion
Various preoperative imaging modalities have been studied to assess the relevant vascular anatomic structures, including Color Doppler ultrasonography, computed tomographic angiography (CTA) and magnetic resonance angiography (MRA)[2-4]. CTA and MRA can display the blood supply of transplanted skin flaps and accurately evaluate the course of blood vessels, which is essential to ensure the success of flap transplantation[5]. MRA traditionally lags behind CTA with respect to spatial resolution. However,CTA imaging requested the injection of contrast agent which often caused nephrotoxicity. Due to large radiation dose required, Only CTA imaging for artery phase was performed.Contrast enhanced (CE) differential subsampling with cartesian ordering (DISCO) was an ultra-fast dynamic enhanced angiography technique, featured by a dual echo spoiled gradient echo acquisition for water-fat separation, a pseudo-random variable density κ-space segmentation and κ-space shared reconstruction technology. It is a high temporal and spatial resolution imaging technique, allowing multi-phase dynamic contrast enhancement.
So far, DISCO has been applied in multi-phase abdominal, breast and intracranial aneurysm measurement, demonstrating that DISCO could shorten the scan time and reduce image artifacts [6-8]. Therefore, the main goal of this study was to evaluate the clinical value of DISCO imaging in preoperative assessment of anterolateral thigh flap by using operative findings as a reference.
Materials and Methods
SubjectsA total of 15 patients who underwent anterolateral femoral flap transplantation were included, containing 12 males and 3 females, ranging from 14 years old to 72 years old.
MRI Experiment
All MRI experiments were performed on a 3T MRI (SIGNA Pioneer, GE, USA) with an abdominal coil employed.
Coronal DISCO imaging was acquired with field of view of 42cm×42cm, covering pelvis and patella. Other scan parameters were of TR=3.1ms, TE=1.1ms, flip angle=25°, slice thickness=2.6-3.0mm and matrix=320×256. The scan time was 5 seconds per single phase.
Before scanning, Gadoteric Acid Meglumine Salt (0.4ml/kg) was used as a contrast agent and injected using test contrast agent bolus injection technique at a rate of 3ml/s.
Data analysis
The acquired DISCO images were analysed using Maximum Intensity Projection (MIP), Multi-Plane Projection (MPR) and Volume Roaming Technology (VRT) methods in GE ADW4.7 workstation.
Two experienced radiologists analysed the CE DISCO MRA images, respectively. When the conclusions were inconsistent, both radiologists reached an agreement after discussion. The following information were recorded, including the origin, course, and distribution of the lateral femoral circumflex artery (LFCA), the surface measurement signs of the perforator superficial point of the descending branch of LFCA. The vertical and horizontal distance from the perforator superficial point to the outer upper edge of the patella were considered as the major and transverse diameters, respectively.
Results
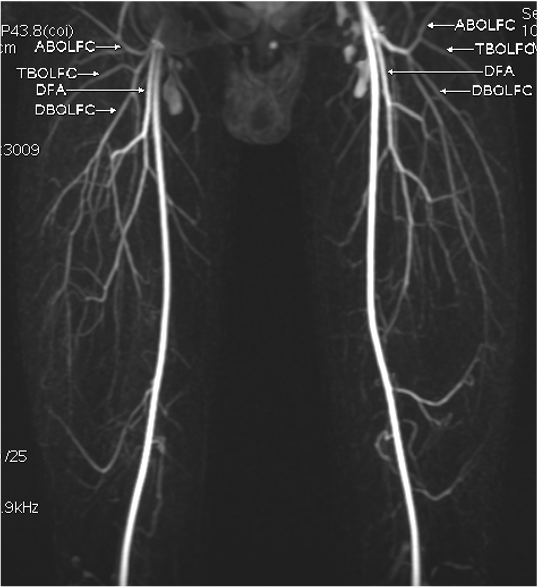
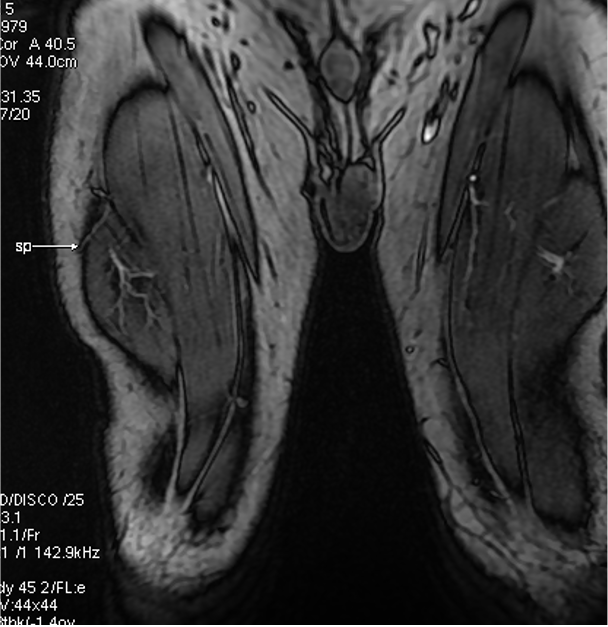
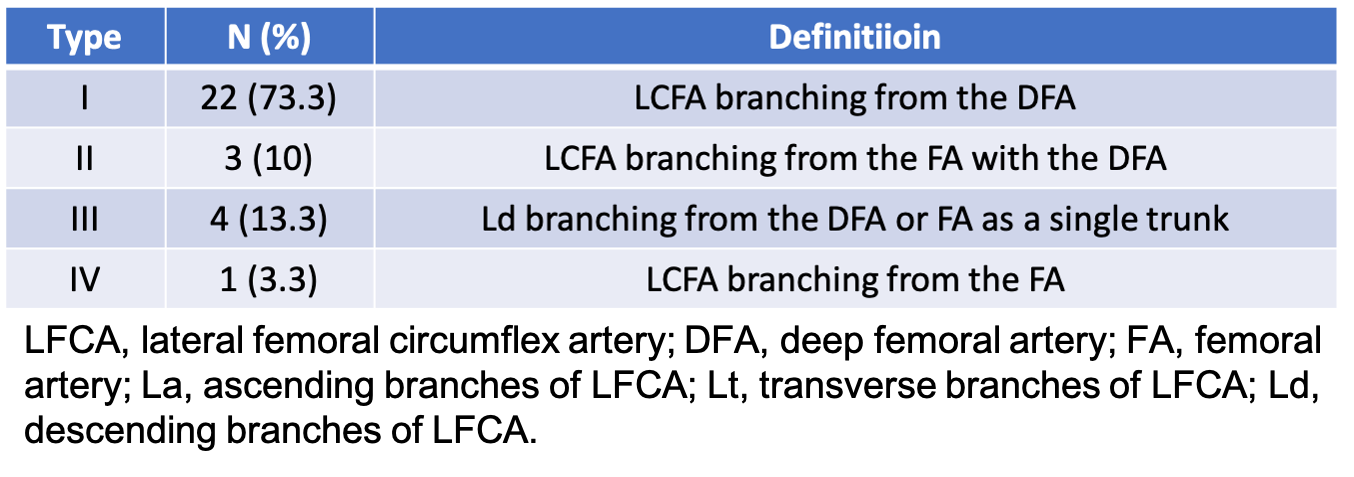
A total of 15 patients underwent DISCO measurement. 30 blood vessels were measured. Four different origins of lateral femoral circumflex artery (LCFA) were found in all patients (Table 1): Type I (73%) - LCFA originating from the deep femoral artery (DFA) (Figure 1); Type II (10%) - LCFA branching from the femoral artery (FA) with the DFA; Type III (14%) - the descending branches of the LCFA originating from the DFA or FA as a single trunk; Type IV(3%)- LCFA branching from the FA.In addition, the relationship between the perforator of the descending branches of LFCA and the muscle was clearly shown. Moreover, the surface signs of the perforator superficial point of the descending branch of the LFCA was also identified, which is crucial in designing the flaps (Figure 2).
The displayed origin, distribution and course of blood vessels were consistent with the operative findings. The fifteen flap’s locations were accurate and sizes were optimal. The anterolateral femoral flaps in all cases were successfully operated without re-selection of flaps during the operation. Total flap survival rate was 100%. All flaps showed good blood supply, and reached stage I healing without infection or delayed healing.
Discussion
MRA was a method without radiation. However, its spatial resolution was worse than CTA, along with long scanning time. DISCO is able to solve both problems. It is a high-temporal and high-spatial resolution imaging technique, allowing multi-phase dynamic contrast enhancement. Single-phase scanning only took 5 seconds, which not only provided detailed information of blood vessels in the grafted skin flap, but also assessed accurately the movement of blood vessels in the soft tissues of the flap. Multi-phase dynamic scanning also ensured the clarity of the distal blood vessels, but with no radiation hazard, which greatly facilitates clinical application. Due to the advantage of MRI in soft tissue display, it could accurately display the penetration point of the perforating artery in skin, which provided a precise position for the operation to be beneficial for blood vessel separation, reduced the incidence of intra-operative injuries and improved the survival rate.Conclusions
In conclusion, in this preliminary study, CE DISCO MRA has been demonstrated an accurate and compatible method for imaging perforators preoperatively prior to ALT flaps.Acknowledgements
No acknowledgement found.References
1. Rozen, W., et al., Anatomical variations in the harvest of anterolateral thigh flap perforators: a cadaveric and clinical study. Microsurgery, 2009. 29(1): p. 16-23.
2. Łuczewski, Ł., et al., Colour Doppler sonography in the preoperative assessment of the vascular pedicle from the anterolateral thigh flap: proposal for a mathematical formula to predict pedicle length. European archives of oto-rhino-laryngology 2019. 276(3): p. 815-819.
3. Shen, Y., et al., Application of Computed Tomography Angiography Mapping and Located Template for Accurate Location of Perforator in Head and Neck Reconstruction with Anterolateral Thigh Perforator Flap. Plastic reconstructive surgery, 2016. 137(6): p. 1875-85.
4. Chen, F., et al., Noncontrast Magnetic Resonance Imaging of Perforators for Preoperative Evaluation of Anterolateral Thigh Flaps. Plastic reconstructive surgery. Global open, 2020. 8(10): p. e3174.
5. Liu, S., et al., Comparison of surgical result of anterolateral thigh flap in reconstruction of through-and-through cheek defect with/without CT angiography guidance. cranio-maxillo-facial surgery, 2011. 39(8): p. 633-8.
6. Wei, Y., et al., Gadoxetate acid disodium-enhanced MRI: Multiple arterial phases using differential sub-sampling with cartesian ordering (DISCO) may achieve more optimal late arterial phases than the single arterial phase imaging. Magnetic resonance imaging, 2019. 61: p. 116-123.
7. Morrison, C., et al., Novel High Spatiotemporal Resolution Versus Standard-of-Care Dynamic Contrast-Enhanced Breast MRI: Comparison of Image Quality. Investigative radiology, 2017. 52(4): p. 198-205.
8. Nael, K., et al., Differential Subsampling with Cartesian Ordering for Ultrafast High-Resolution MRA in the Assessment of Intracranial Aneurysms. 2020. 30(1): p. 40-44.
Figures