1616
Accelerated 3D whole-heart angiography using Compressed SENSE in patients with Congenital Heart Disease1Pediatric Cardiology, University of Texas Southwestern, Dallas, TX, United States, 2Kafrelsheikh univeristy, Kafr El Sheikh, Egypt
Synopsis
3D whole-heart bSSFP (3DWH) is the clinical standard in the evaluation of anatomy in congenital heart disease (CHD), but can be time consuming to acquire. A compressed sense (CS-SENSE) algorithm to accelerate standard SENSE technique recently became commercially available, and was shown to accelerate clinical protocols in adults. 3DWH accelerated by CS-SENSE factor of 3.5 provided visualization of all structures with no degradation in CNR or image quality while reducing scan time by approximately 25% in pediatric congenital heart disease.
Introduction
3D whole-heart bSSFP (3DWH) is the clinical standard in the evaluation of anatomy in congenital heart disease (CHD)(1), but can be time consuming to acquire. A compressed sense (CS-SENSE) algorithm to accelerate standard SENSE technique recently became commercially available, and was shown to accelerate clinical protocols by up to 20%(2). 3DWH accelerated by CS-SENSE was studied in adults(3), although factors such as patient motion and volume coverage may influence the degree of acceleration that can be achieved in pediatrics. The purpose of this study was to evaluate the performance of CS-SENSE at various acceleration factors in patients with CHD.Methods
3DWH images were acquired in 26 patients (3-23 years, MED 11) on a 1.5T Philips Ingenia. Coronal images were acquired following Gd administration, 1.4-1.8mm isotropic resolution, TE/TR = 1.8/3.6 ms, flip angle=60, and a T2 prep module. Scans were cardiac triggered to the end-systolic rest period(1), and a respiratory navigator was used for motion compensation. In each patient, a 3DWH dataset was acquired using conventional SENSE with a factor of 1.5 in both phase and slice directions, followed by a second volume using CS-SENSE factors of 2.5, 3.5, 5, or 6.5. Image quality was assessed by the number of visible cardiac structures(4), and right coronary artery (RCA) visibility was evaluated as described by McConnell et al (5). Anonymized and randomized images were scored by two experienced CMR readers. The reduction in the contrast to noise ratio (CNR) measured between the aorta and myocardium(5) was used to quantitatively assess the reduction in image quality with CS-SENSE relative to conventional SENSE. A Wilcoxon signed rank test was used to assess changes in image quality.Results and Discussion
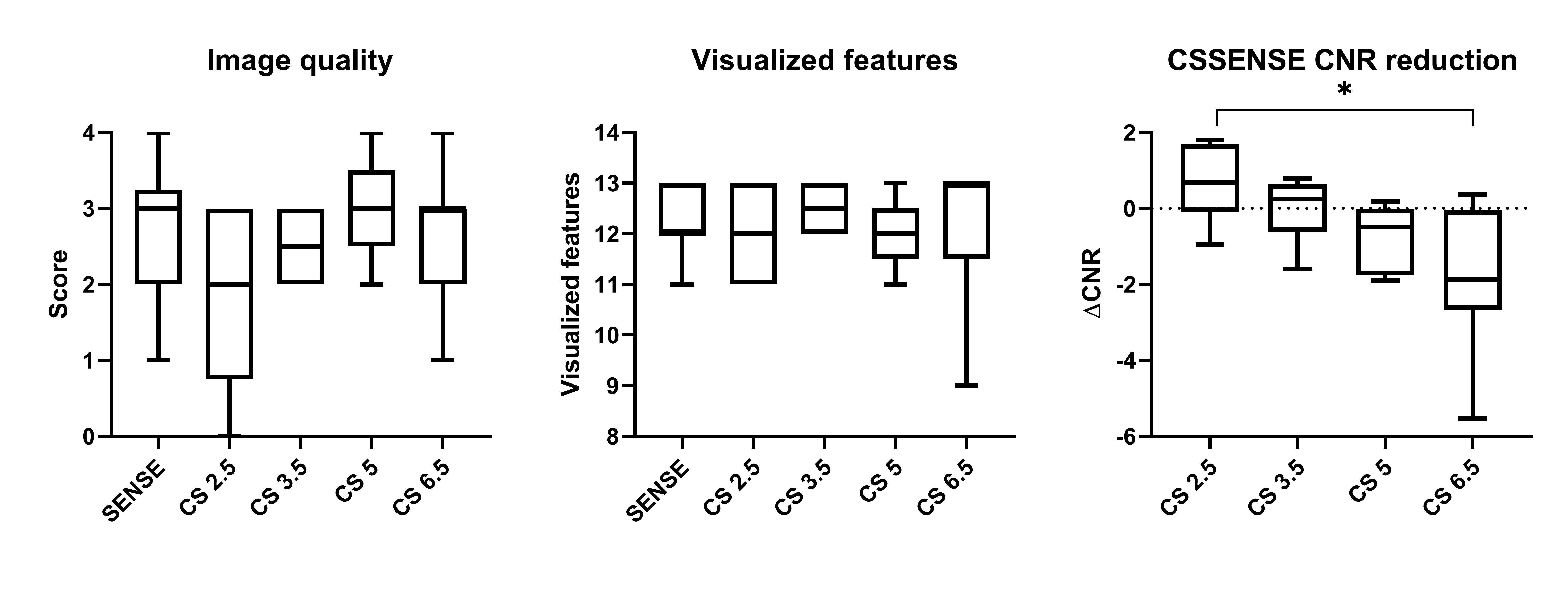
The average scan time for SENSE was 3:17 minutes, which was reduced to 2:48, 2:29, 1:25, and 1:15 using CS-SENSE factors of 2.5-6.5. Figure 1 shows the RCA in different patients with SENSE and CS-SENSE. There was no significant change in the visible structures or coronary artery visibility metrics (Fig 2A and 2B). A CS-SENSE factor of 6.5 caused a significant reduction in CNR compared to SENSE (Fig 2C). An average increase in CNR was also noted for CS-SENSE factors of 2.5 and 3, while there was a gradual decline in CNR with higher acceleration. This could be attributed to the moderate acceleration factors reducing the influence of patient motion without significantly degrading image quality. Additional patients are required to determine if a significant improvement in this metric can be achieved using CS-SENSE.Conclusion
Although the RCA visibility and number of visualized structures was not affected by higher acceleration factors, the gradual decline in CNR at higher acceleration factors could make clinical evaluation challenging. A CS-SENSE factor of 3.5 provided visualization of all structures with no degradation in CNR or image quality while reducing scan time by approximately 25% in pediatric congenital heart disease.Acknowledgements
No acknowledgement found.References
1. Greil, G., Tandon, A. A., Silva Vieira, M. & Hussain, T. 3D whole heart imaging for congenital heart disease. Frontiers in pediatrics 5, 36 (2017).
2. Sartoretti, E. et al. Reduction of procedure times in routine clinical practice with Compressed SENSE magnetic resonance imaging technique. PloS one 14, e0214887 (2019).
3. Ohmoto-Sekine, Y. et al. Clinical Performance of Non-contrast Whole-heart Magnetic Resonance Coronary Angiography with Compressed Sensing: Comparison with Conventional Sensitivity Encoding Imaging. Proceedings 27th annual meeting of the International Society for Magnetic Resonance in Medicine, Monreal, Canada, 2051 (2019).
4. Henningsson, M. et al. Feasibility of 3D black-blood variable refocusing angle fast spin echo cardiovascular magnetic resonance for visualization of the whole heart and great vessels in congenital heart disease. 20, 76 (2018).
5. Makowski, M. R. et al. Congenital heart disease: cardiovascular MR imaging by using an intravascular blood pool contrast agent. Radiology 260, 680-688 (2011).
Figures