1614
Differentiating cardiac function and hemodynamics in treated and untreated models of aortic coarctation1Medical College of Wisconsin, Milwaukee, WI, United States, 2Marquette University, Milwaukee, WI, United States, 3Jean-Monnet University, Lyon, France, 4University of Michigan, Ann Arbor, MI, United States
Synopsis
Aortic coarctation (CoA) is a congenital vascular disease characterized by severe narrowing of the proximal descending thoracic aorta, which affects 5,000-8,000 births annually in USA. Patients with CoA can have altered hemodynamics and remodeled left ventricle from increased afterload. In this study, we investigate the impact of CoA on cardiovascular parameters using rabbit models of treated and untreated CoA. The results showed that cardiovascular parameters can normalize in treated CoA compared to untreated cases and that myocardial strain and aortic blood velocity are sensitive parameters for differentiating between treated and untreated CoA as well as the severity of coarctation.
Introduction
Coarctation of the aorta (CoA) is a congenital vascular disease characterized by severe narrowing of the proximal descending thoracic aorta with varying hemodynamic severity that impacts cardiac function. Although simple surgical correction has saved the lives of thousands, many of the long-term problems observed after treatments for CoA can be explained on the basis of abnormal cardiac function and hemodynamic patterns. Although remodeling of the left ventricle (LV) in response to pressure overload has been studied in numerous animal models, there is a paucity of data using a clinically representative blood pressure gradient (BPG) that resembles CoA in patients to investigate the impact on cardiac function and hemodynamics. In this study, we investigate the impact of CoA on cardiovascular parameters using rabbit models that resemble treated and untreated CoA in patients.Methods
New Zealand white rabbits underwent CoA of the proximal descending thoracic aorta when they were ~10-weeks of age to produce six rabbit models of CoA with stenosis pressures of 5mmHg, 10mmHg, and 20mmHg (permanent and dissolvable stitches to resemble untreated and treated CoA). An additional rabbit was included in the study as control. Anesthetized rabbits were scanned at 32 weeks in the supine, head-first position on a GE 3T MRI Premier scanner (GE Healthcare, Waukesha, WI) using an 18-channel knee coil and peripheral gating. Both cine and tagging images were acquired during free-breathing to obtain short-axis (SAX) and long-axis (LAX) slices covering the heart. Furthermore, phase-contrast images were acquired across the ascending aorta (AAo) and the proximal descending aorta (DAo). The cine images were analyzed using the cvi42 software to measure ejection fraction (EF) and mass. The tagged images were analyzed using Sinusoidal Modeling (SinMod) technique to measure circumferential (Ecc) and longitudinal (Ell) myocardial strains. The phase-contrast images were analyzed to measure velocity at the AAo and proximal DAo.Results
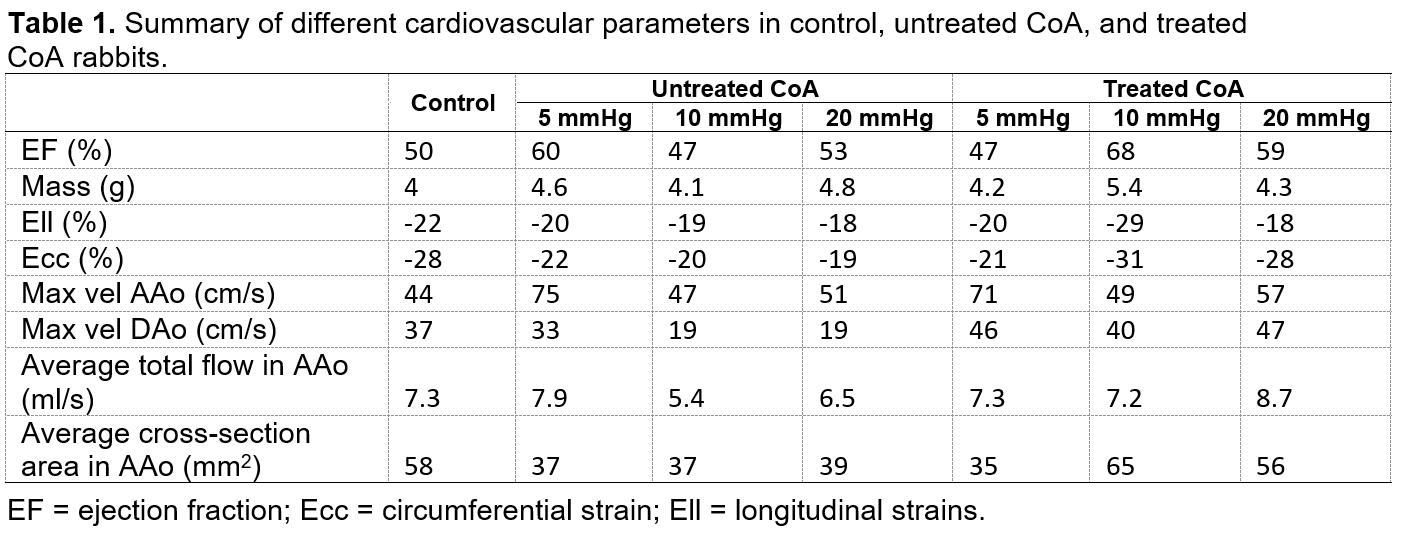
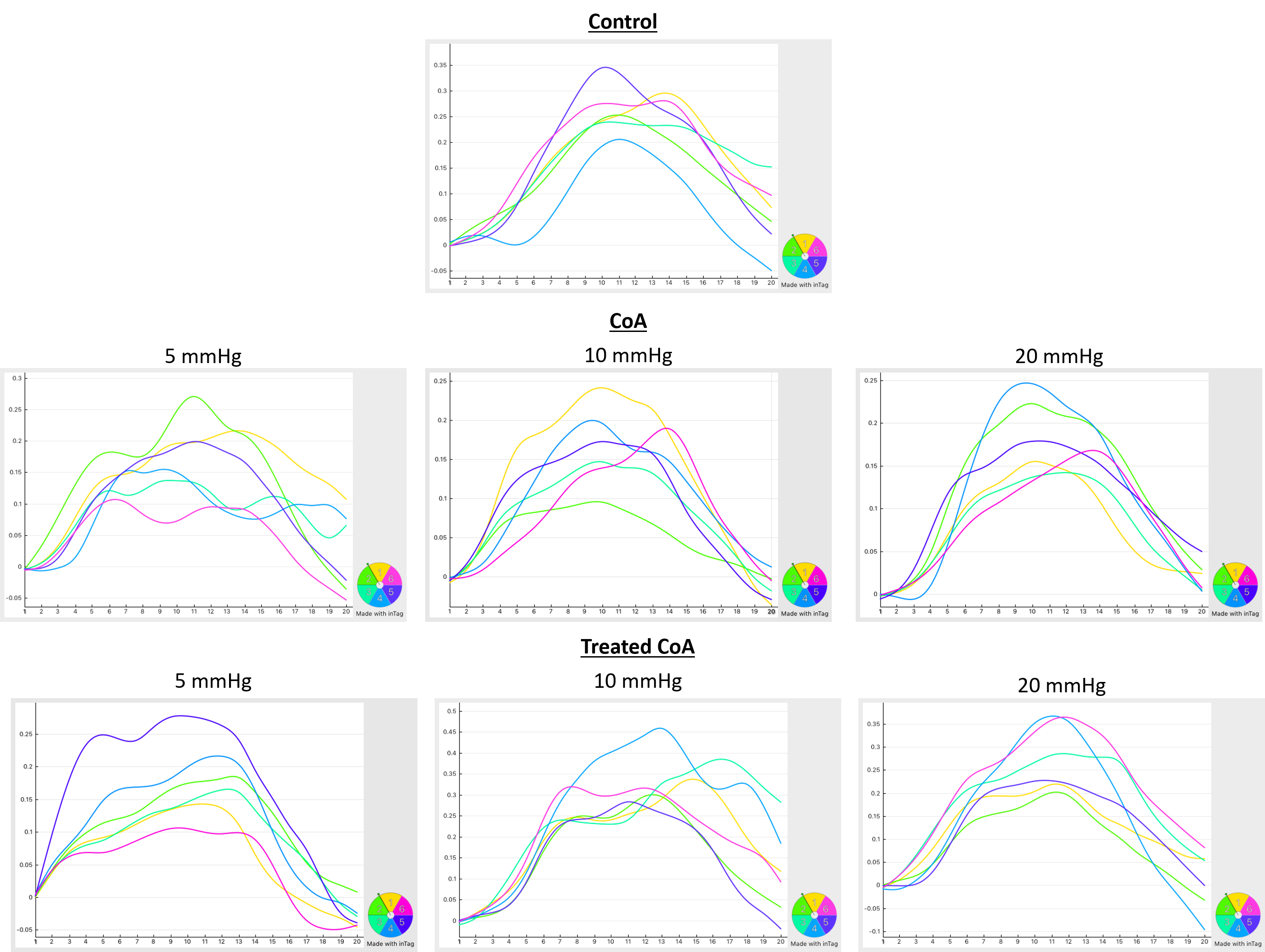
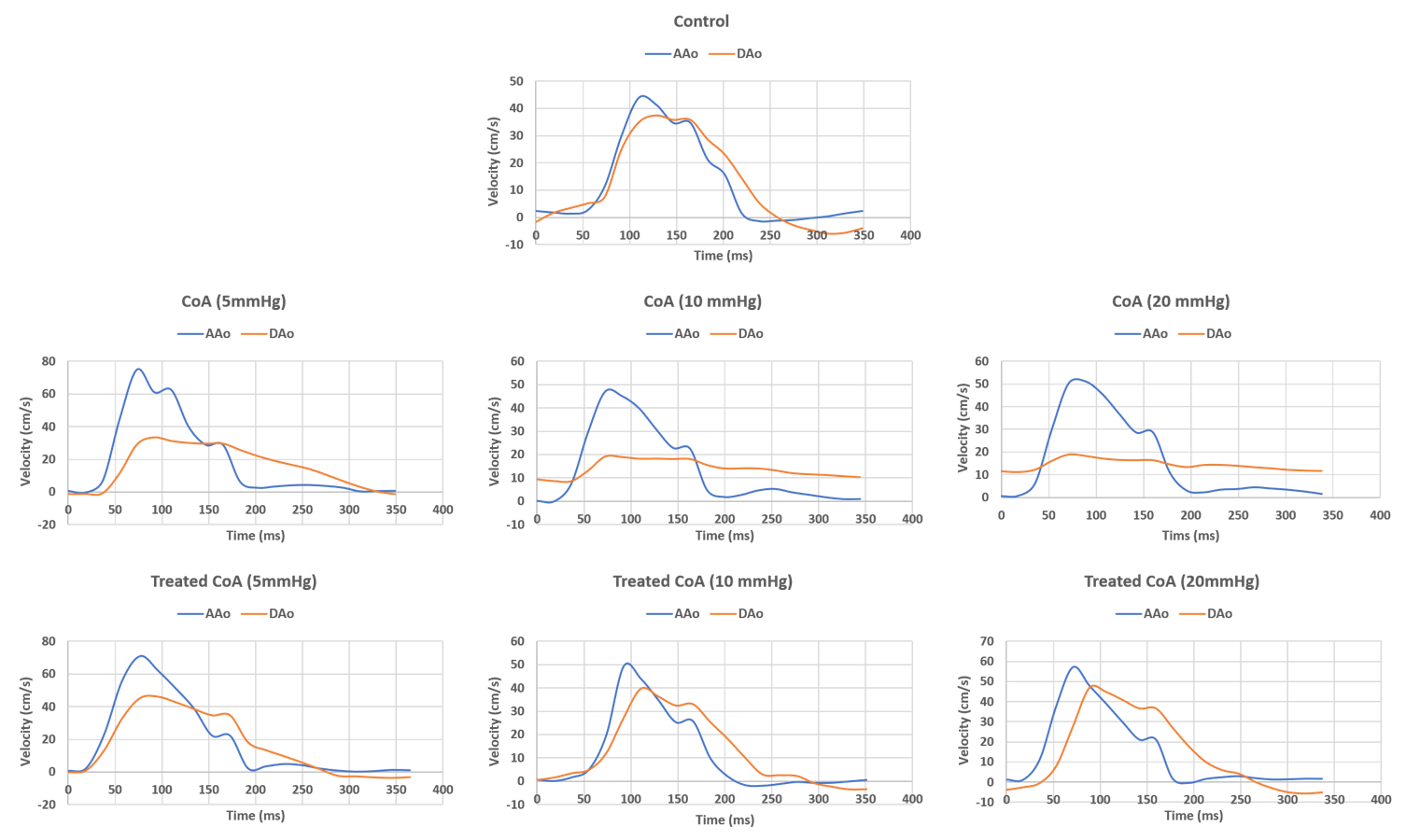
Table-1 summarizes the results from all rabbits. The results showed distinguishing measurements between permanent and treated coarctation, which also depended on the severity of coarctation. Compared to control (EF=50%), EF increased to 60% at 5mmHg, but decreased to 47% and 53% at 10mmHg and 20mmHg, respectively, in untreated CoA rabbits. However, this pattern was reversed in the treated CoA rabbits, where EF was 47% at 5mmHg, but increased to 68% and 59% at 10mmHg and 20mmHg, respectively. Myocardial mass at 10mmHg untreated CoA (4.1g) was similar to that in the control rabbit (4g). However, mass increased at 5mmHg (4.6g) and 20mmHg (4.8g) in the untreated CoA. This pattern was reversed in treated CoA rabbits, where mass was higher at 10mmHg (5.4g) compared to 5mmHg (4.2g) and 20mmHg (4.3g). Both Ell and Ecc showed continuous decrease (in absolute value) with increasing degree of coarctation in untreated CoA compared to control, as shown in Figure-1. Ell was -22%, -20%, -19%, and -18% in the control, 5mmHg, 10mmHg, and 20mmHg untreated CoA rabbits, respectively. Ecc was -28%, -22%, -20%, and -19% in the control, 5mmHg, 10mmHg, and 20mmHg untreated CoA rabbits, respectively. The corresponding strain measurements were different in treated CoA rabbits, where (Ell and Ecc) were larger at 10mmHg (-29%, -31%) compared to 5mmHg (-20%, -21%) and 20mmHg (-18%, -28%). Velocity patterns in AAo and DAo are shown in Figure-2. Maximum blood velocity in AAo increased in (untreated CoA and treated CoA) at 5mmHg (75cm/s, 71cm/s) compared to 10mmHg (47cm/s, 49cm/s) and 20mmHg (51cm/s, 57 cm/s), but all values were larger than that in the control rabbit (44 cm/s). A similar pattern occurred for the DAo in untreated CoA, where maximum velocity at 5mmHg (33 cm/s) was larger than 10mmHg and 20mmHg (both values were 19cm/s), while in treated CoArc, maximum velocity was 46cm/s, 40cm/s, and 47cm/s at 5mmHg,10mmHg, and 20mmHg, respectively. Maximum velocity in the DAo in the control rabbit was 37cm/s. As blood velocity is affected by flow and vessel cross-sectional area, these parameters are listed for different rabbit models in Table-1.Discussion and Conclusions
The results showed different patterns of changes in global function, regional function, and hemodynamics between untreated and treated CoA, which depended on the severity of coarctation. In general, myocardial hypertrophy and increased EF in most CoA models represent an underlying ventricular remodeling to maintain global function in treated CoA compared to untreated CoA, especially at high degree of coarctation. Nevertheless, regional cardiac function, represented by myocardial strain, showed to be a sensitive measure of CoA, especially in untreated cases, where both Ell and Ecc continuously decreased with increasing severity of coarctation. The hemodynamic results showed that the ratio between maximum velocity in AAo to that in DAo was slightly >1 in control and treated CoA compared to untreated CoA, where the ratio was always >2 in the latter. In conclusion, MR imaging of the developed models of treated and untreated aortic CoA provides valuable information about global and regional cardiac function and hemodynamics in different controlled settings that resemble patients with aortic CoA. The results showed that cardiovascular parameters can normalize in treated CoA compared to untreated cases and that myocardial strain and blood velocity in AAo and DAo are sensitive parameters for differentiating between treated and untreated CoA as well as the severity of coarctation.Acknowledgements
Funding source: NIH R01HL142955 (PI: LaDisa)References
1. Wendell et al. J Surg Res. 218:194-201
2. Menon et al. Am J Physiol Heart Circ Physiol. 303:H1304-18
3. Kwon et al. Pediatr Cardiol. 35:732-740
4. Coogan et al. J Thorac Cardiovasc Surg. 145:489-495
5. LaDisa et al. J Biomech Eng. 133(9):091008
Figures