1563
Motion Robust Free-Breathing MR-Fingerprinting1Memorial Sloan Kettering Cancer Center, New York, NY, United States, 2Philips Research, Hamburg, Germany
Synopsis
The acquisition of quantitative MRI biomarkers with sufficiently high spatiotemporal resolution and coverage remains challenging. This is particularly difficult in organs of the abdomen, where respiratory, pulsative, and peristaltic motion may introduce biases in the expected evolution of signal intensity. This work describes an implementation of free-breathing MR-fingerprinting (MRF) for quantitative imaging of the abdomen. The method relies on golden-angle radial sampling combined with compressed sensing and parallel imaging. We compare MRF-derived parametric maps in vivo as a function of reconstruction algorithm and in free-breathing (FB) and breath-hold (BH) acquisitions.
Synopsis
The acquisition of quantitative MRI biomarkers with sufficiently high spatiotemporal resolution and coverage remains challenging. This is particularly difficult in organs of the abdomen, where respiratory, pulsative, and peristaltic motion may introduce biases in the expected evolution of signal intensity. This work describes an implementation of free-breathing MR-fingerprinting (MRF) for quantitative imaging of the abdomen. The method relies on golden-angle radial sampling combined with compressed sensing and parallel imaging. We compare MRF-derived parametric maps in vivo as a function of reconstruction algorithm and in free-breathing (FB) and breath-hold (BH) acquisitions.Purpose
We aim to implement a free-breathing MR-fingerprinting acquisition with improved image quality and reduced sensitivity to artifacts from physiologic motion.Materials and Methods
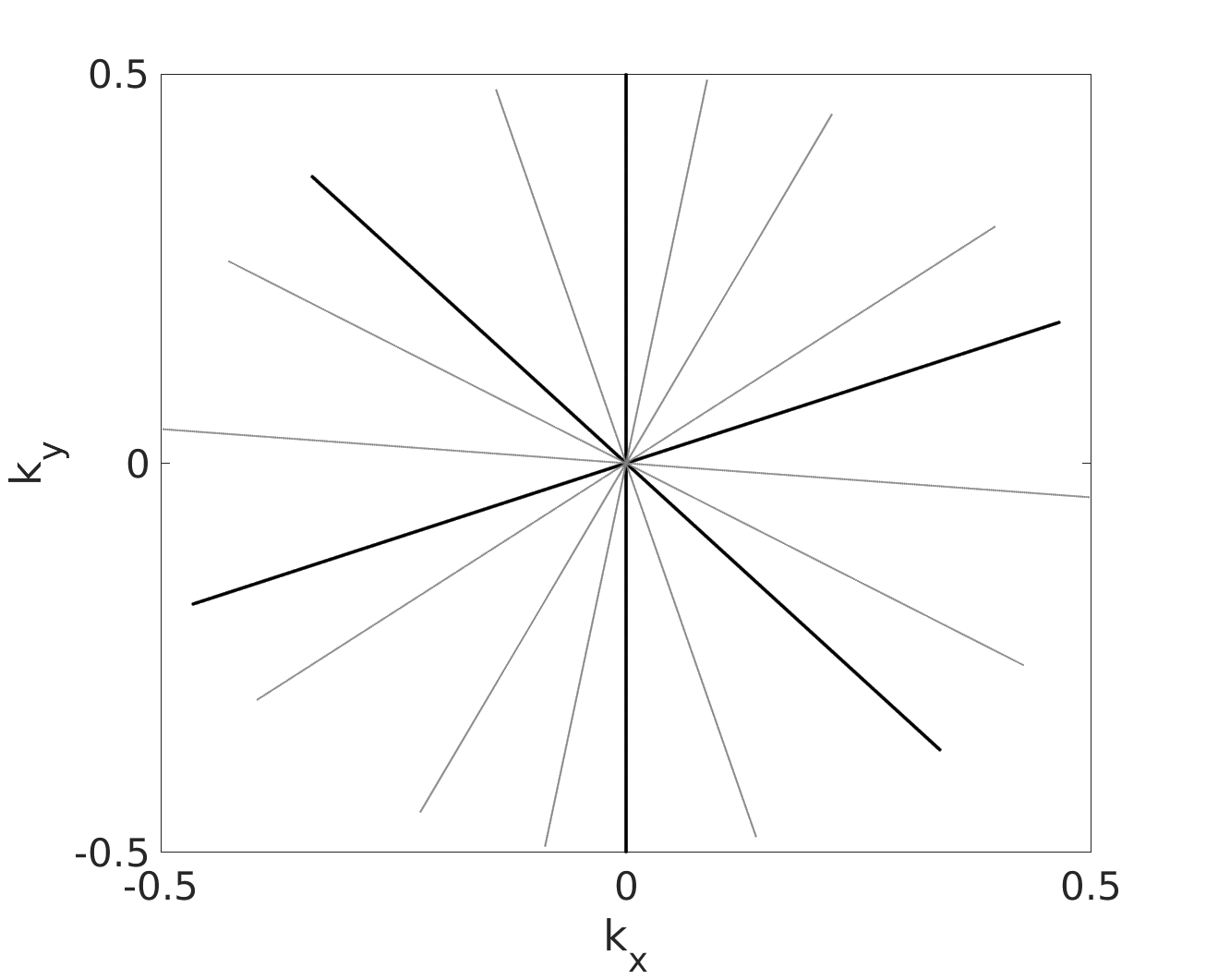
The proposed method is based on golden-angle radial sparse parallel (GRASP)1 MRI combined with a gradient-spoiled SSFP MRF sequence with a varying flip-angle (FA) train. The sequence consists of an inversion pulse followed by the varying flip angle schedule and a delay time (Td) to allow for some relaxation to thermal equilibrium. Slice effects are minimized by using a high-bandwidth excitation pulse. The imaging parameters are: TR/TE/TI/Td = 8/4/15/100 ms, FOV = 25 x 25cm2, matrix = 224 x 224, and slice thickness = 5mm. An FA train with 500 timepoints in the range [0° 60°] was used. The sequence is implemented in a 3T MRI scanner (Philips Medical Systesm, Best, Netherlands). The total number of spokes in the acquisition is spaced based on the golden-angle. In each interleaf with the spokes are spaced by the multiplication of golden angle and number of spokes/timepoint. Figure 1 demonstrates schematically the sampling function for 3 spokes/timepoint.A healthy volunteer was imaged using a 16-channel anterior coil combined with a 12-channel posterior coil. The imaging slice was positioned in the axial plane corresponding to the largest coverage of the liver. The volunteer was instructed to breathe normally during the FB acquisitions and hold their breath at end inspiration for the BH acquisitions. The number of spokes/dynamic was varied from 1-3. Images were reconstructed with either gridding or GRASP. ROIs were placed at three uniform regions in the liver parenchyma and the mean and standard deviation of the MRF-derived parametric maps was compared.
Results
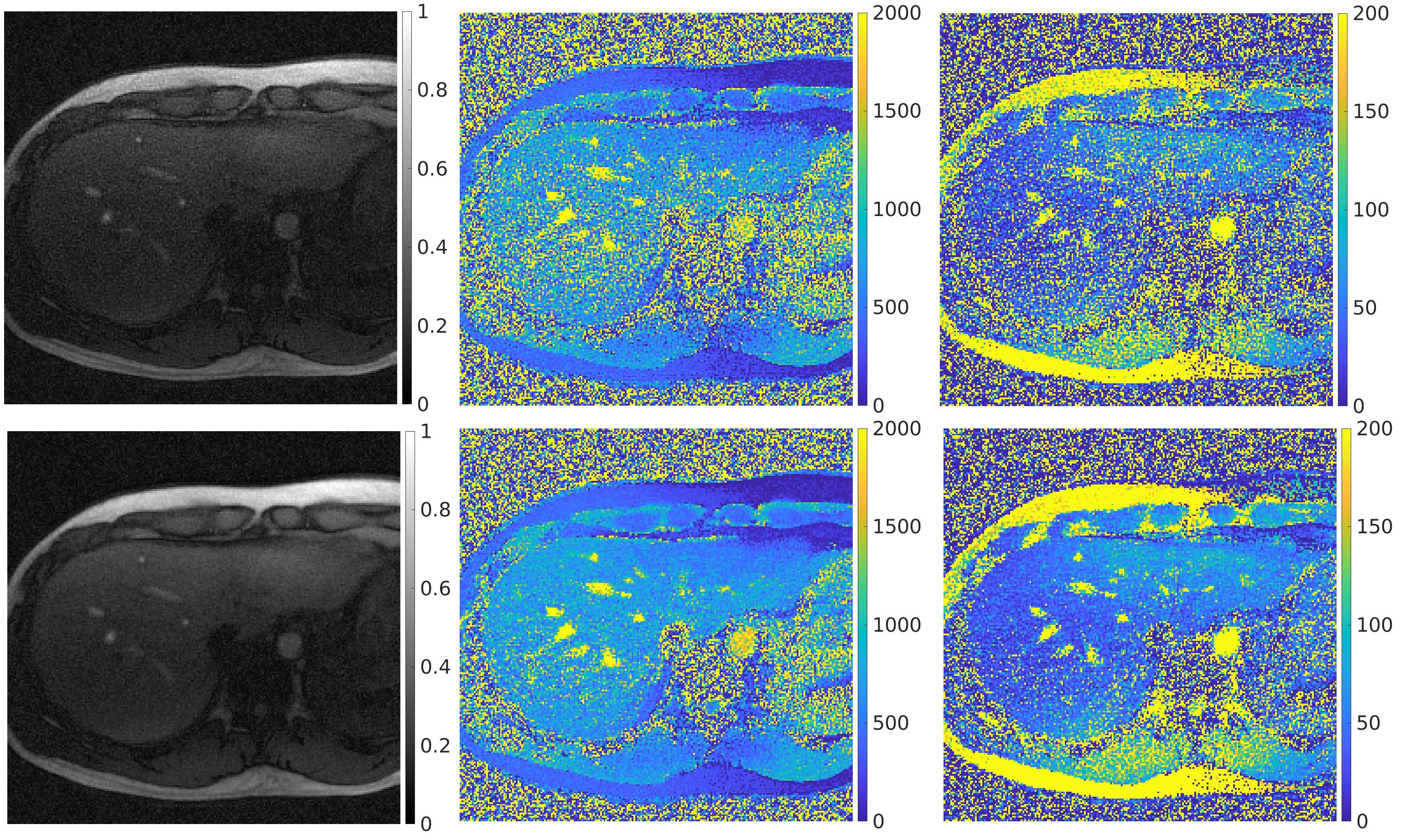
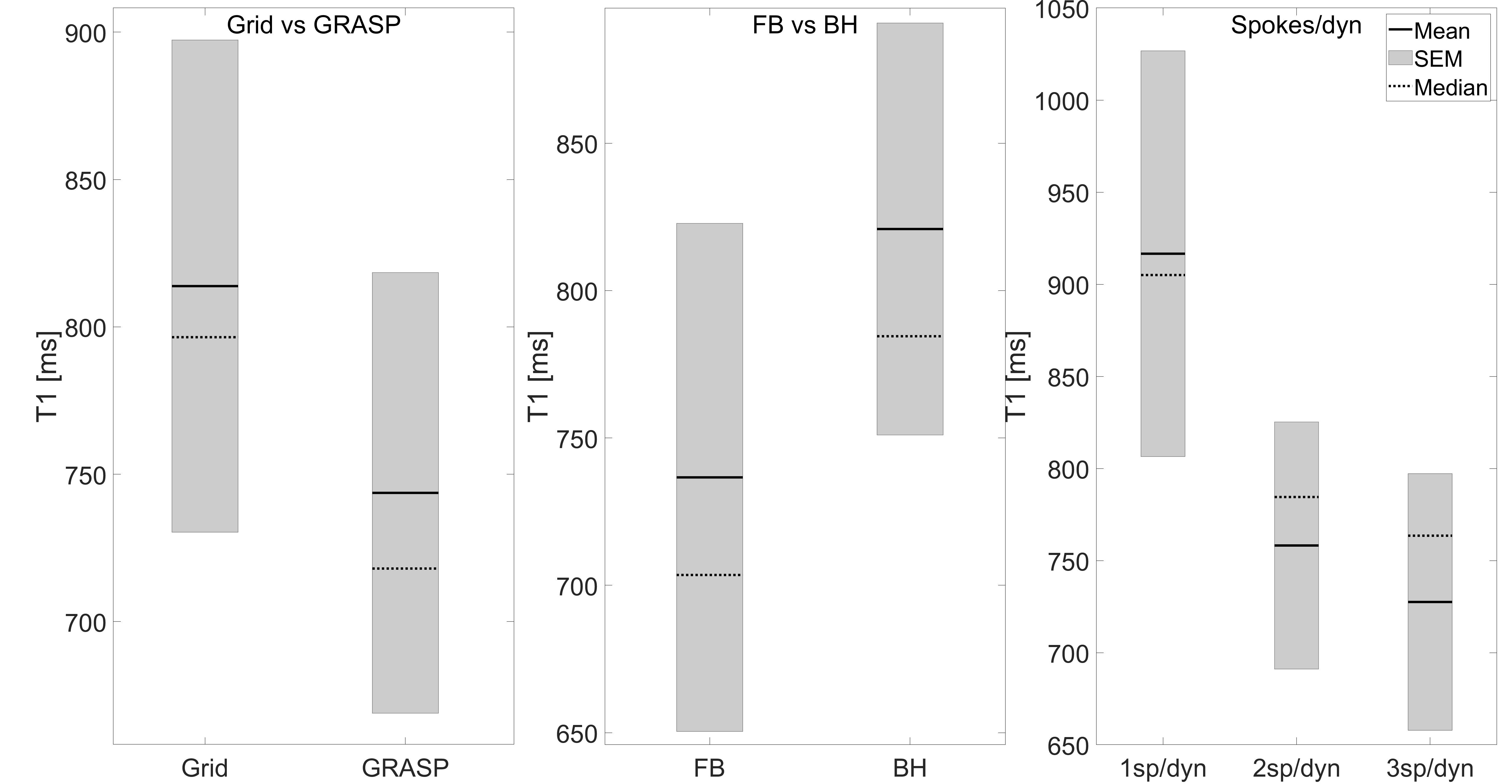
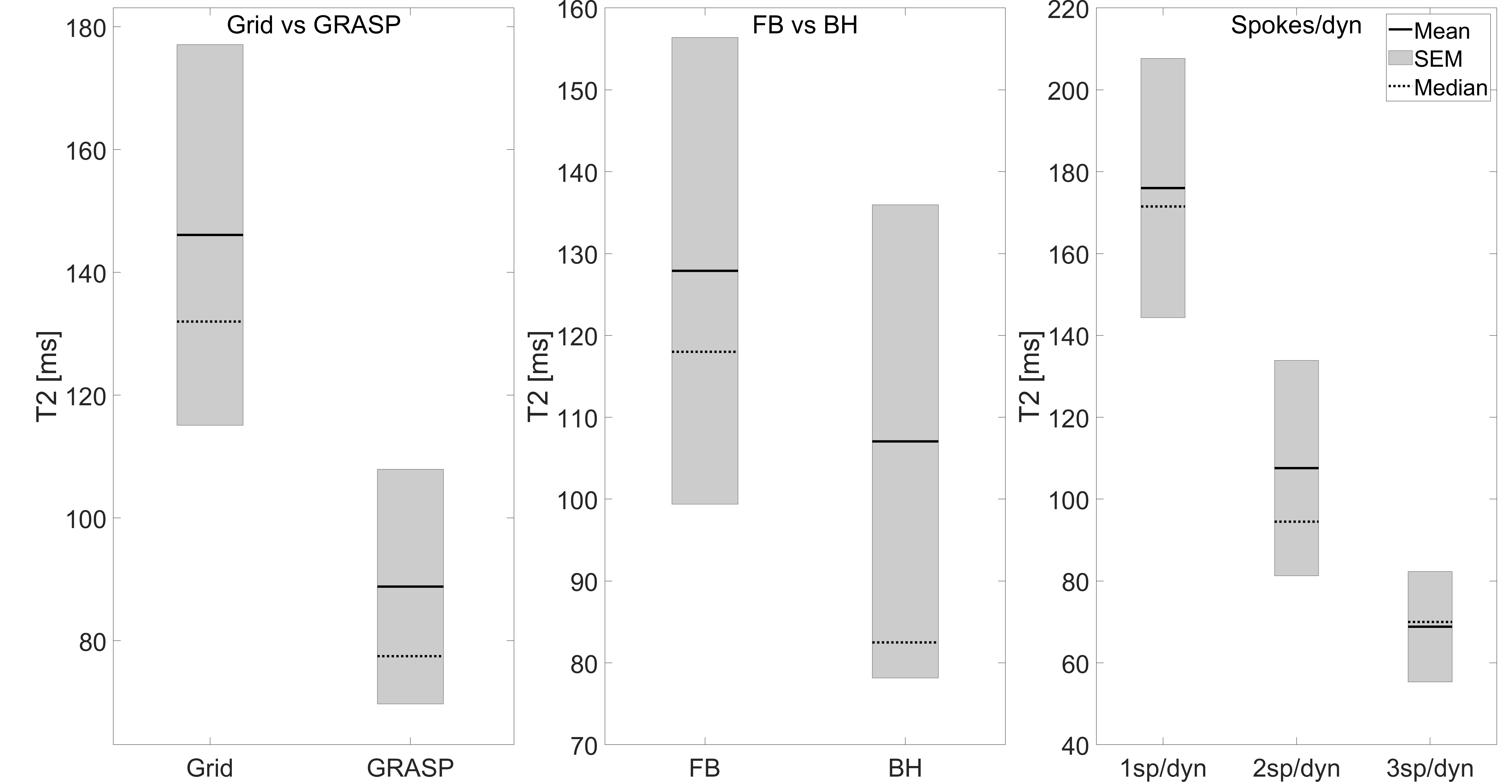
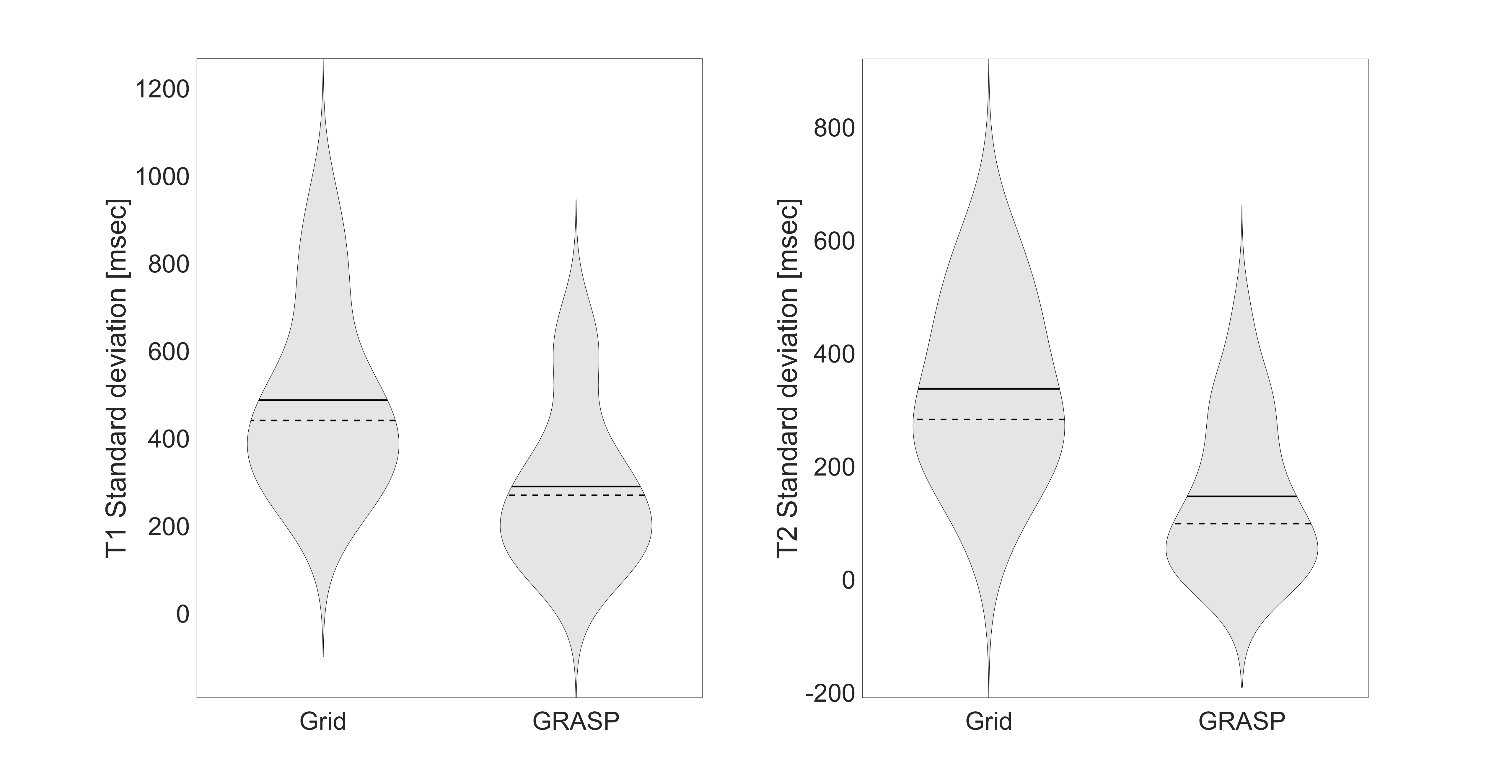
Figure 2 demonstrates improvements in image quality in a comparison of proton density (PD), T1, and T2 maps for FB imaging. The effect of reconstruction algorithm, FB vs BH, and number of spokes/dynamic on the estimated T1 values is shown in Fig.3. Similarly, the effect of reconstruction algorithm, FB vs BH, and number of spokes/dynamic on the estimated T2 values is shown in Fig.4. Figure 5 demonstrates the effect of reconstruction algorithm on the standard deviation of the estimated parametric maps.Discussion
The reconstruction algorithm shows an improvement in image quality as measured by the amount of artifacts in the parametric maps and noise, as shown in Fig. 5. Overall, GRASP reconstruction estimates lower value of the parametric maps while undersampling increases the estimation of the parametric maps increases. While there were differences in FB vs BH reconstructions, this may arise due to different levels of breath hold. All estimated T1/T2 values were within the range of normal values reported in the literatureConclusion
GRASP provides a feasible method for free-breathing MR-fingerprinting with improved image quality and reduced sensitivity to artifacts from physiologic motion.Acknowledgements
No acknowledgement found.References
1. Feng L, Grimm R, Block KT, et al. Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magnetic resonance in medicine. 2014;72(3):707-717.
2. Obmann. V, Mertineit, N, Marx, C, et al. Liver MR relaxometry at 3T - segmental normal T(1) and T(2)* values in patients without focal or diffuse liver disease and in patients with increased liver fat and elevated liver stiffness. Scientifi Reports. 2019: 9(1): 8106-8106
Figures