1527
Task-phase fMRI evidencing cognitive improvement post carotid angioplasty and stenting (CAS) – initial findings of a follow-up study1Department of Biomedical Physiology & Kinesiology, Simon Fraser University, Burnaby, BC, Canada, 2Health Research and Innovation, Fraser Health Authority, Surrey, BC, Canada, 3Department of Medicine, University of British Columbia, Vancouver, BC, Canada, 4Department of Radiology, Royal Columbian Hospital, New Westminster, BC, Canada, 5Department of Neurology, Royal Columbian Hospital, New Westminster, BC, Canada
Synopsis
This longitudinal task-phase fMRI study aims to provide direct evidence of possible effects of Carotid angioplasty and stenting (CAS) on cognition. The initial phase enrolled patients with severe carotid stenosis (≥70% stenosis) who had MRI scans pre-CAS and two-month post-CAS. At each scan, patients completed two fMRI sessions while performing a working memory task. Improved cerebral perfusion to areas supplied by carotid arteries following CAS was correlated with improved cognitive function in working memory performance along with increased fMRI activations in the re-perfused vascular territory especially in frontal and temporal lobes and reduced in the contralateral hemisphere.
Introduction
The narrowing of the carotid arteries with plaque formation (carotid stenosis) represents a major risk factor for ischemic stroke and cognitive impairments especially when severe (≥70% stenosis).1-2 Carotid angioplasty and stenting (CAS) is a standard clinical treatment to reduce stroke risk. 3 The cognitive effect of CAS remains largely unknown. Current clinical standard evaluates primarily the successful completion of the procedure by assessing correct stent placement and perioperative complications such as 30-day stroke rate and death. 4 Previous research has mostly relied on paper-based cognitive tests to study the cognitive impact of CAS while the few functional MRI (fMRI) studies were only conducted at resting phase. 5-11 Both traditional cognitive tests and the resting-state fMRI data lacked the ability to detect the brain functional changes in solving cognitive problems that require the application of task-phase fMRI. This study aims to provide direct evidence of possible effects of CAS on cognition, using task-phase blood-oxygen level dependent (BOLD) fMRI.Methods
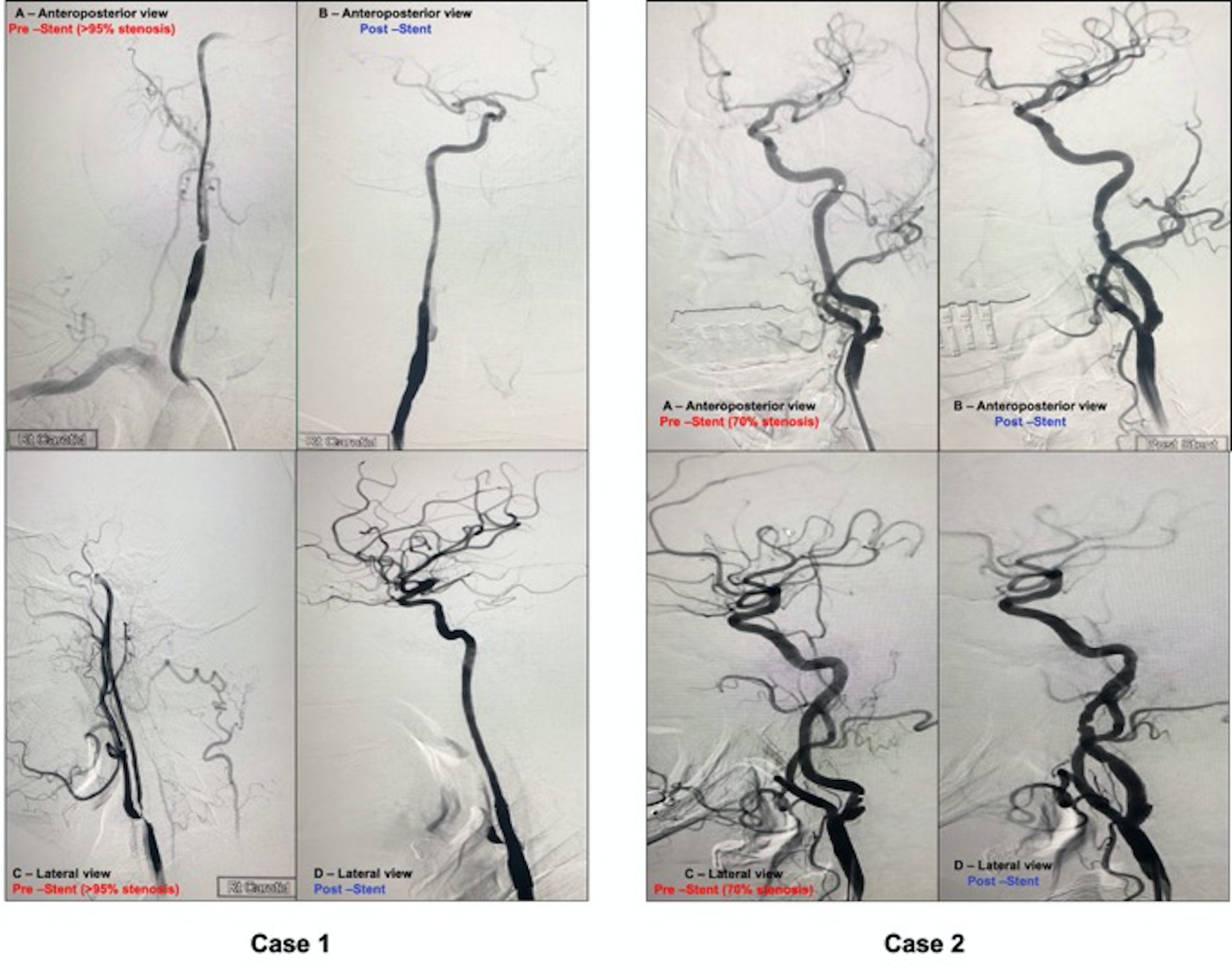
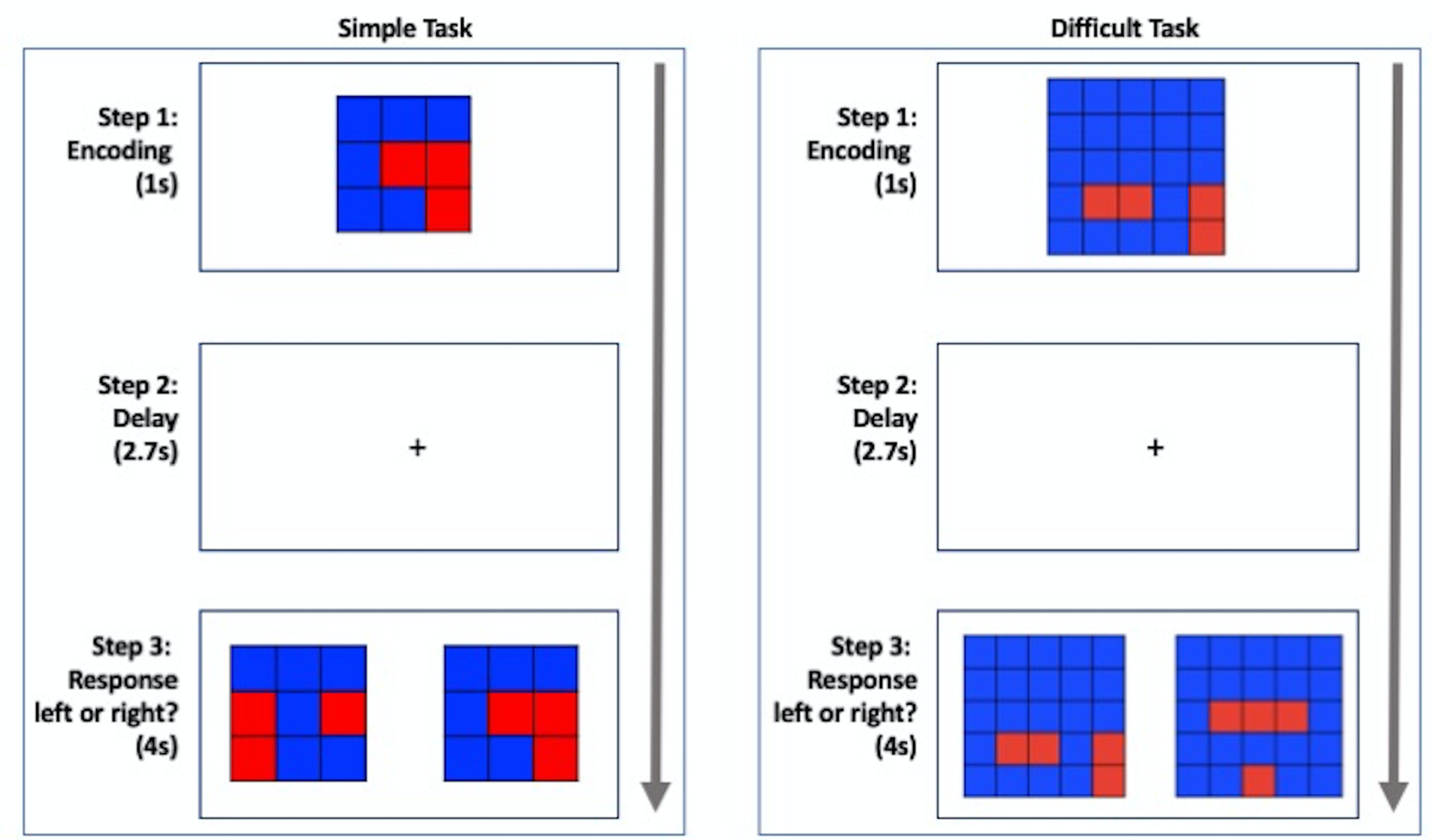
This study built is on top of standard clinical care. Patients with carotid stenosis scheduled for CAS as part of standard care, had MRI scans pre-CAS and two-month post-CAS. The initial findings involved two patients. Case 1 is a 65-year-old man who had severe (>95%) flow-limiting stenosis in the right carotid artery. Case 2 is an 81-year-old man who had 70% non-flow limiting stenosis in the left carotid artery (Figure 1). At each scan, patients completed two fMRI sessions that lasted for approximately 5 minutes each, while performing a working memory task. The delayed match to sample working memory task was applied, adapted with modification for the study with two levels of task difficulties (Figure 2). The task began with presentation of a stimulus (for encoding), followed by a 2.7 sec delay, and then a response, for which participants were instructed to indicate the stimulus shown before, when it was presented together with a distractor image. 12-13 MRI scans were conducted using a whole-body Philips Ingenia 3.0T CX Quasar Dual MRI system equipped with 32-channel dStream head coil and operated by Release 5.3 (Philips Medical Systems Nederland B.V.). The fMRI utilized an echo planar imaging (GRE-EPI) sequence (TR/TE=2000/30ms, flip angle=90◦, 3x3x3 mm3 voxels covering the whole-brain). High-resolution anatomical T1 images (for co-registration) were acquired. Data were analyzed using FMRI Expert Analysis Toolbox following standard procedures. 14-15 Accuracy, reaction time, and brain activation were analyzed for each patient for possible pre-post CAS changes.Results
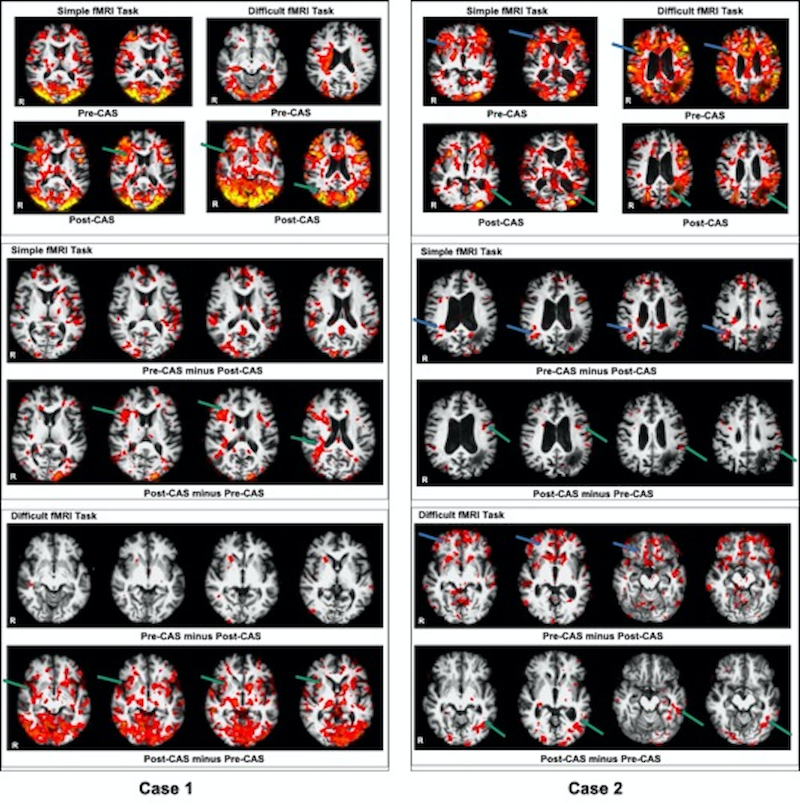
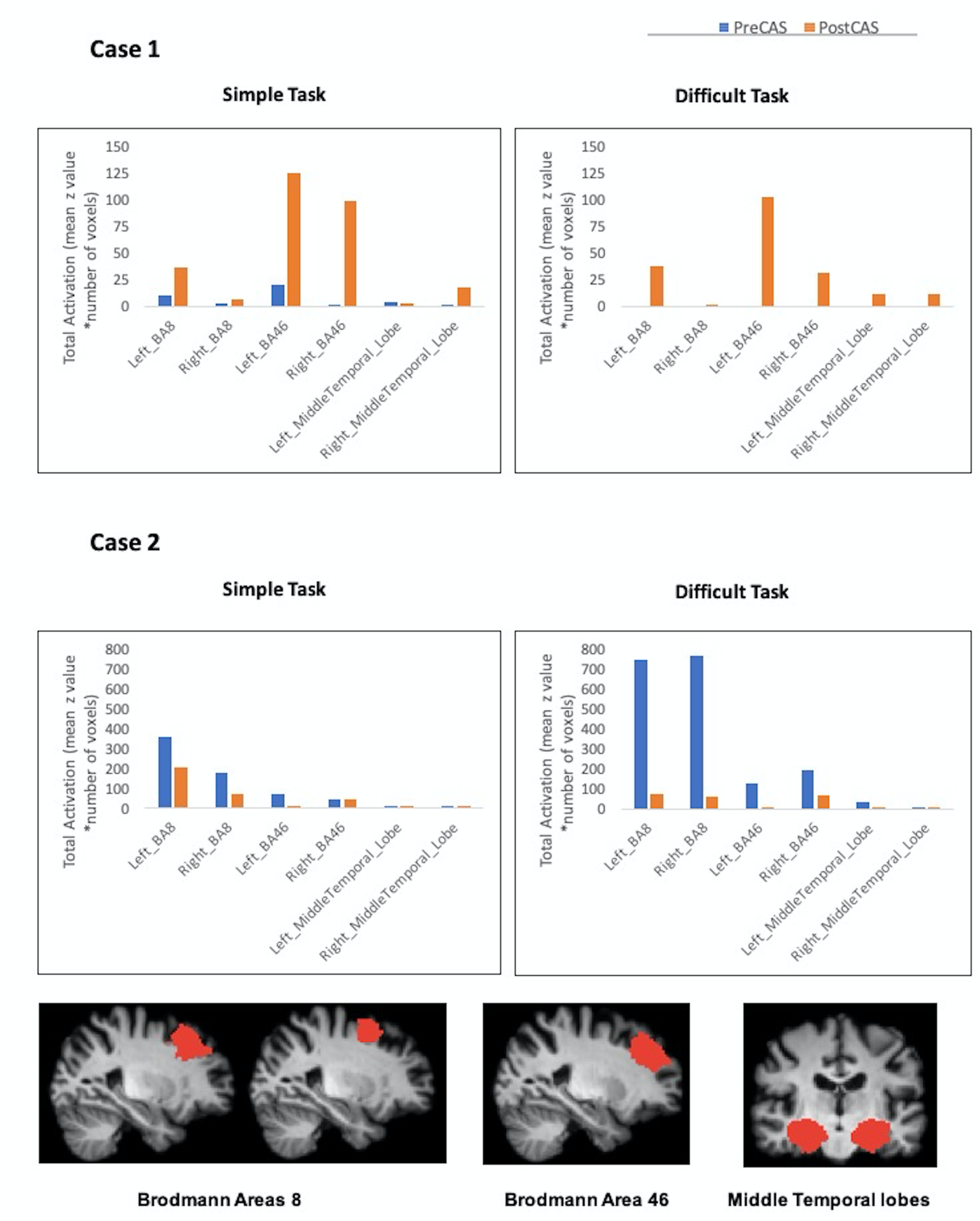
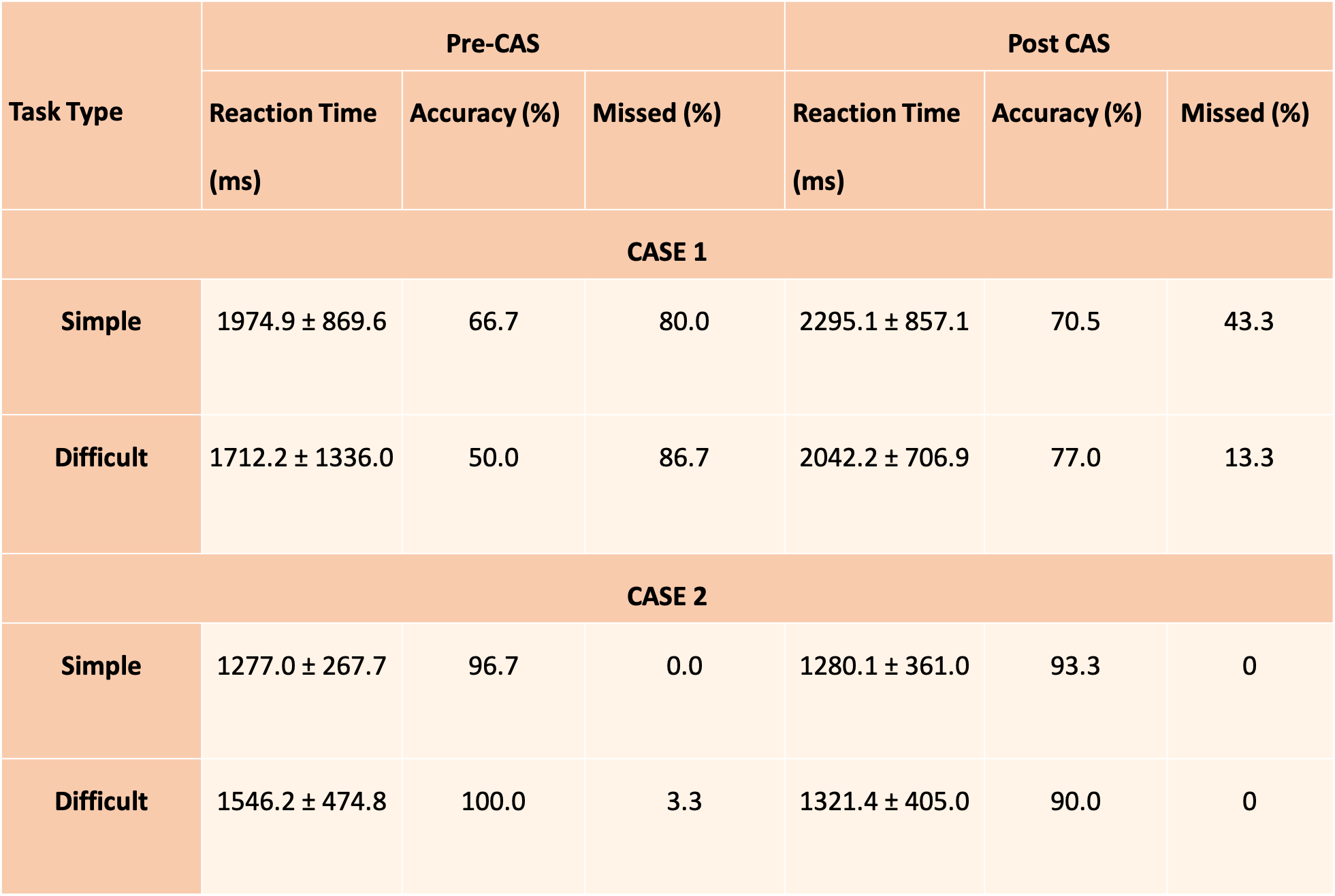
Case 1 showed increased activation in the right (treated-side) frontal and medial temporal lobes post-CAS; which was associated with improvements in accuracy (from 58% to 74%) and task completion rate (from 17% to 72%). Excellent baseline cognitive performance was observed pre-CAS across both the simple and difficult tasks, which was not improved further by the CAS procedure in Case 2. Case 2 completed the tasks pre- and post-CAS with >90% accuracy, while decreased fMRI activation in the contralateral (untreated) hemisphere and mildly increased activation in the left (treated -side) anterior circulation territory were observed post-CAS (Figures 3-5).Discussion
Improved cerebral perfusion to areas supplied by carotid arteries following CAS was correlated with improved cognitive function in working memory performance along with increased fMRI activations in the re-perfused vascular territory especially in frontal and temporal lobes and reduced in the contralateral hemisphere. However, considerable individual variability between the two cases impacted the cognitive changes observed post-CAS. Higher severity of stenosis with great flow limitation, poorer collateral circulation and lower cognitive reserve pre-CAS was associated with greater cognitive improvements post-CAS in Case 1 compared to Case 2.Conclusion
This study provided the first task-phase fMRI data demonstrating that CAS improved cognitive function in the re-perfused vascular territory. The finding supports the role of CAS in improving cognitive performance beyond reducing stroke risk. Enlightened by these cases, we hope to further test the cognitive outcomes of artery stenting using task-phase fMRI as described here with increased sample size and more follow-up sessions, involving matched healthy control participants.Acknowledgements
The authors would like to thank Bob Strain and Kim Crooks-William, patient partners of the research project for their valuable and constructive contributions. We thank the patient participants for volunteering in the study. We thank the SFU ImageTech Lab for approval for the research team to conduct the MRI experiment with three hours of pilot scans at reduced MRI scanner fee charge. The authors acknowledge the Departments of Medical Imaging, Interventional Radiology and Neurology at Royal Columbian Hospital, Department of Evaluation and Research Services, and Surrey Memorial Hospital of Fraser Health for technical and administrative supports.
This work was supported by a research grant from the Royal Columbian Hospital Foundation (G2019-21000). Additional research and scholarship supports were from the Surrey Hospital Foundation (G2017-001), Canadian Institute of Health Research Graduate Scholarship Program and the BC SUPPORT Unit Fraser Centre SPOR initiative.
References
- Flaherty ML, Kissela B, Khoury JC, et al. Carotid artery stenosis as a cause of stroke. Neuroepidemiology. 2013;40:36-41.
- Moneta GL, Edwards JM, Chitwood RW, et al. Correlation of north american symptomatic carotid endarterectomy trial (NASCET) angiographic definition of 70% to 99% internal carotid artery stenosis with duplex scanning. J Vasc Surg. 1993;17:152-159.
- Morris DR, Ayabe K, Inoue T, et al. Evidence-based carotid interventions for stroke prevention: state-of-the-art review. J Atheroscler Thromb. 2017;24:373-387.
- Higashida RT, Meyers PM, Phatouros CC, et al. Reporting standards for carotid artery angioplasty and stent placement. J Vasc Interv Radiol. 2004;15:421-422.
- Plessers M, Van Herzeele I, Vermassen F, et al. Neurocognitive functioning after carotid revascularization: a systematic review. Cerebrovasc Dis Extra. 2014;4:132-148.
- Yoon BA, Sohn SW, Cheon SM, et al. Effect of carotid artery stenting on cognitive function in patients with carotid artery stenosis: a prospective, 3-month-follow-up study. J Clin Neurol. 2015;11:149-156.
- Whooley JL, David BC, Woo HH, et al. Carotid revascularization and its effect on cognitive function: a prospective nonrandomized multicenter clinical study. J Stroke Cerebrovasc Dis. 2020;29:104702.
- Gaudet JG, Meyers PM, McKinsey JF, et al. Incidence of moderate to severe cognitive dysfunction in patients treated with carotid artery stenting. Neurosurgery. 2009;65:325-330.
- Tani N, Yaegaki T, Nishino A, et al. Functional connectivity analysis and prediction of cognitive change after carotid artery stenting. J Neurosurg. 2018;131:1709-1715.
- Schaaf M, Mommertz G, Ludolph A, et al. Functional MR imaging in patients with carotid artery stenosis before and after revascularization. Am J Neuroradiol. 2010;31:1791-1798.
- Wang T, Sun D, Liu Y, et al. The impact of carotid artery stenting on cerebral perfusion, functional connectivity, and cognition in severe asymptomatic carotid stenosis patients. Front Neurol. 2017;8:403.
- Daniel TA, Katz JS, Robinson JL. Delayed match-to-sample in working memory: a BrainMap meta-analysis. Biol Psychol. 2016;120:10-20.
- McDonald AP, D'Arcy RCN, Song X. Functional MRI on executive functioning in aging and dementia: a scoping review of cognitive tasks. Aging Med. 2018;1:209-219.
- Jenkinson M, Bannister P, Brady M, et al. Improved optimization for the robust and accurate linear registration and motion correction of brain images. Neuroimage. 2002;17:825-841.
- Woolrich MW, Ripley BD, Brady M, et al. Temporal autocorrelation in univariate linear modeling of FMRI data. Neuroimage. 2001;14:1370-1386.
Figures