1441
Can we use Ultrafast Dynamic Contrast Enhanced MRI to evaluate Ductal Carcinoma in situ?1Diagnostic Imaging and Nuclear Medicine, Kyoto University Graduate School of Medicine, Kyoto, Japan, 2Kyoto Medical Center, Kyoto, Japan, 3Department of Diagnostic Pathology, Kyoto University Hospital, Kyoto, Japan, 4Department of Breast Surgery, Kyoto University Hospital, Kyoto, Japan
Synopsis
Using ultrafast DCE (UF-DCE) MRI, size and morphology of DCIS on very early phase of the post contrast injection were compared to those on early phase of conventional DCE (C-DCE) MRI and on High resolution post contrast enhancement (HR-CE). Lesion size tended to be smaller on UF-DCE MRI. Clustered ring is not frequently observed on UF-DCE MRI compared to HR-CE. These data suggest evaluating DCIS on UF-DCE may be dealt with caution.
INTRODUCTION
Ultrafast DCE (UF-DCE) MRI is a promising method of evaluating breast lesions with much shorter image acquisition. High temporal resolution (4~8 sec) with 1 mm in-plane resolution can be achieved. Diagnostic performance of kinetic information using these semi-quantitative UF-DCE parameters are equivalent to conventional kinetic information obtained on conventional DCE (C-DCE) MRI protocols (1-4). On the other hand, evidence to apply UF-DCE in diagnosing ductal carcinoma in situ (DCIS) is limited. The need of evaluating DCIS on MRI is increasing with wider use of MRI in triaging suspicious microcalcification or high-risk screening. DCIS tends to be smaller in size, more sparsely distributed, and with slower enhancement pattern compared to invasive carcinoma. Due to the slower enhancement, lesion size may be smaller on UF-DCE MRI. Clustered ring, one of the morphological features in BI-RADS specific to DCIS, may not be visible on very early phase, making diagnosis of DCIS difficult. In this study, we aimed to compare size and morphological assessment of DCIS, in particular, presence of clustered ring on UF-DCE MRI to the assessment on early phase of C-DCE and high-resolution post contrast images (HR-CE).METHODS
Study population consists of 25 consecutive patients (mean age 51.4) with 26 lesions who underwent Breast MRI with UF-DCE protocol to evaluate suspicious/known breast lesions from April 2016 to July 2018 with histopathological diagnosis of DCIS (n=22, high/intermediate/low grade:8/13/1) or DCIS with microinvasion (n=4).MR scanning was performed using a 3 T MR system (MAGNETOM Prisma/Skyra, Siemens Healthcare, Erlangen, Germany) equipped with a dedicated 18/16-channel bilateral breast array coil. T2-weighted, T1-weighted, diffusion weighted and fat-suppressed T1-weighted DCE images were obtained. C-DCE Protocol: pre-contrast and two (early and delayed) post-contrast acquisitions at 1–2 and 5–6 min after gadolinium injection for whole breast axial scanning with high temporal resolution (3D-VIBE: TR/TE 3.70/1.36ms, FA 15 and FOV 330 ×330 mm2, thickness 1.0 mm, TA 1min), post contrast acquisition at 2–5 min after gadolinium injection for whole breast coronal scanning with high (spatial) resolution (3D-VIBE: TR/TE 4.01/1.63ms, FA 15, FOV×3302 mm, matrix 512x461, TA 2.5min thickness 0.8mm). Gadobutrol (Gadovist, Bayer, Germany) at a dose of 0.1 ml/kg power injected at a speed of 2.0 ml/s were infused and flushed with 20 ml of saline at the same rate. UF-DCE acquisitions were obtained using a prototype sequence based on the 3D gradient-echo VIBE sequence at a very early phase, starting 15 seconds before injection and lasting until 1 min after gadolinium injection (TR/TE 5.0/2.5, FA 15, FOV 360 mm×360 mm, matrix 384x269, thickness 2.5 mm, CS acceleration=16.5, temporal resolution 3.7 sec for 20 time frames).
Image analysis was performed per lesion. On UF-DCE MRI, all 20 images of different time frames were reviewed to identify enhancing lesions, and the 20th image was used to measure lesion size. Their size (maximum diameter), lesion type (mass and non-mass enhancement (NME)). morphology including presence of clustered ring were evaluated independently by two experienced radiologists based on BI-RADS MRI 2013. On C-DCE MRI, early post-contrast DCE images (Early-DCE), and high-resolution post contrast images (HR-CE) were used. Difference between lesion size on each MRI sequence and that on pathology (reference) were calculated by [“size on MRI” minus “size on pathology”]. Difference of lesion size from pathology among UF-DCE, Early-DCE, HR-CE images were compared using Wilcoxon’s signed rank test. Proportion of clustered ring among UF-DCE, Early-DCE, HR-CE images were compared using McNemar test. The significance level was adjusted for multiple comparison by Bonferroni correction.
RESULTS
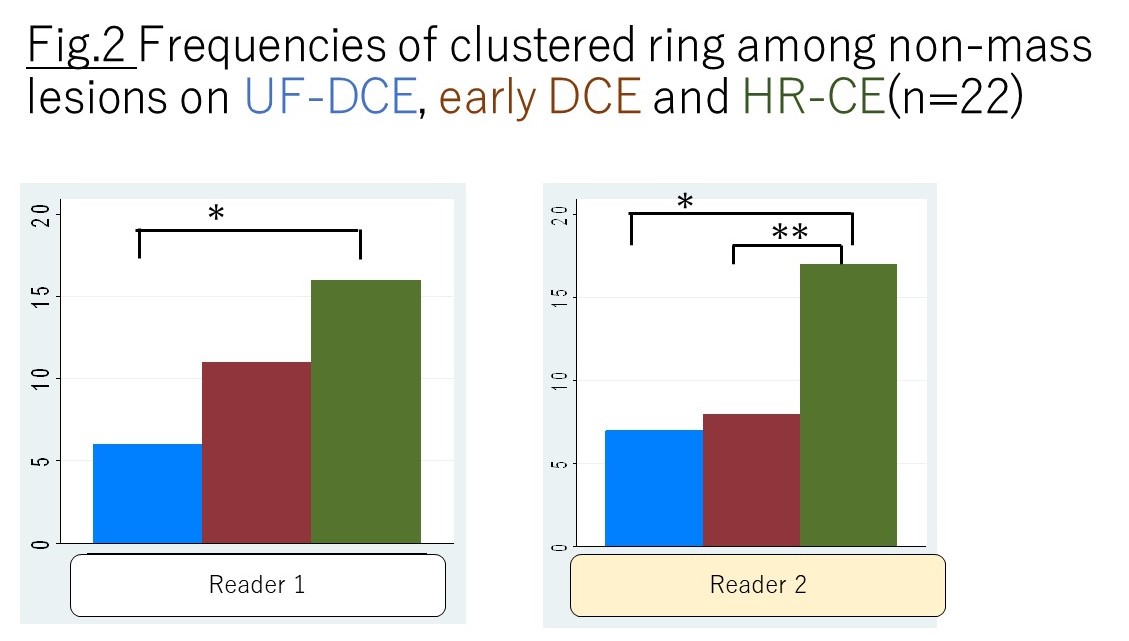
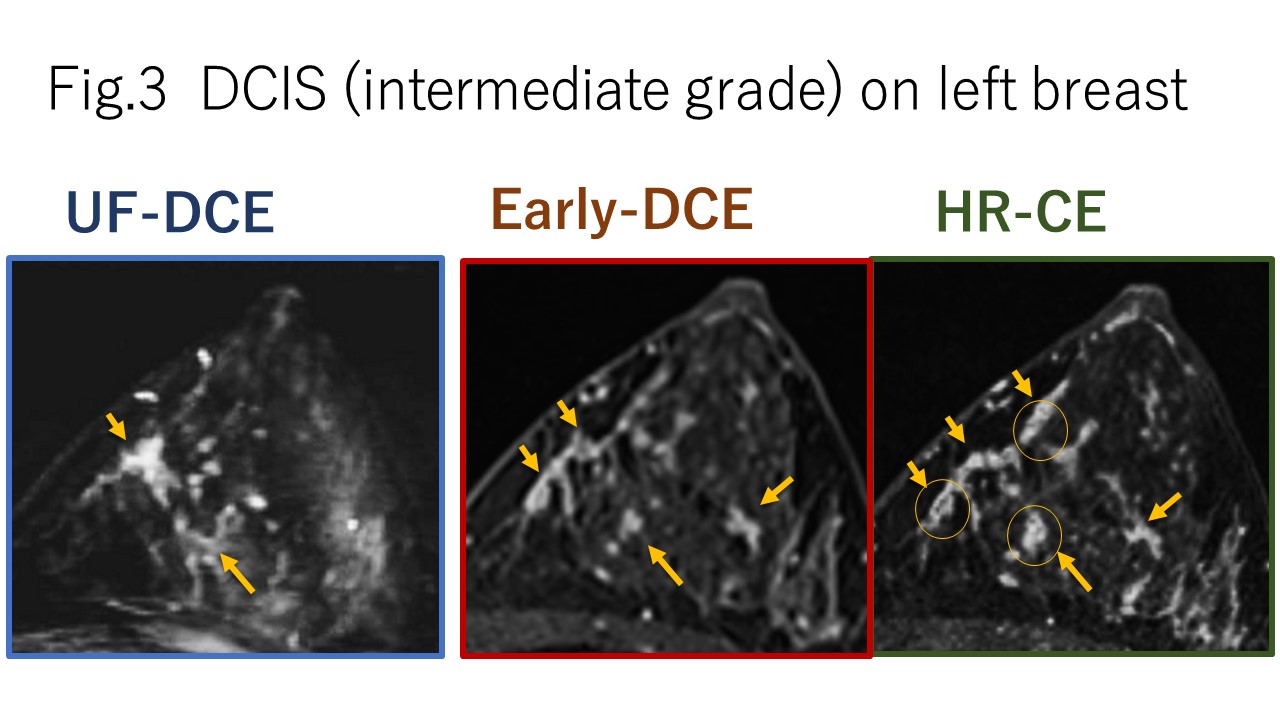
Size: Average lesion size on UF-DCE/Early-DCE/HR-CE MRI were 32.8 (SD23.7) /36.0 (24.9) /38.7 (25.2) mm respectively for reader 1, 30.7 (22.9) /32.8 (24.3) /34.7(24.8) mm respectively for reader 2. Lesion size tended to be smaller on UF-DCE MRI. Difference between lesion size on each MRI sequence and that on pathology were displayed on box plot on figure 1. Difference between lesion size on MRI and pathology was smaller on UD-DCE, compared to that on Early-DCE and HR-CE for both readers (p<0.01). Difference was smaller on early DCE compared to that on HR-CE (p<0.01).Morphology: Among 26 lesions, four lesions were classified as “masses” while 22 lesions were classified as “NME. For 22 NME lesions, the most discrepant morphology among all three contrast-enhanced images was “clustered ring”. Frequencies of clustered ring among NME on UF-DCE, early DCE and HR-CE were demonstrated on figure 2. Compared to HR-CE, clustered ring was less visible on UD-DCE for both readers. (McNemar test, *p<0.01). Similar tendency was observed between Early-DCE and HR-CE for reader 2 (**p<0.05). Representative cases were shown in figure 3.
DISCUSSION and CONCLUSIONS
Our results demonstrated that DCIS tended to be smaller on UF-DCE MRI. When compared to pathology, there were cases with over-estimation and under-estimation. Although there are wide discrepancies in lesion size between MRI and pathology, the mean difference was minimum on UF-DCE compared to early DCE or HR-CE. For morphological evaluation, clustered ring was visible, yet less frequently observed on UF-DCE MRI. Considering that clustered ring is one of the useful features for DCIS, diagnosis of DCIS based on UF-DCE MRI might be interpreted with caution. A new approach of diagnosing DCIS using UF-DCE MRI may be needed in the era of abbreviated MRI.Acknowledgements
We thank Yuta Urushibata, Siemens Japan, and Marcel Dominik Nickel, SiemensHealthcare GmbH, Germany, for their technical support in this work. This work was partly supported by JSPS KAKENHI Grant NUmber 18K07673 "Tumor vascularity and tumor-related vessels using ultrafast DCE MRI of the Breast"References
References:
1) Mann RM et al. A novel approach to contrast-enhanced breast magnetic resonance imaging for screening: high-resolution ultrafast dynamic imaging. Invest Radiol 2014; 49:p579
2) Abe H, et al., Kinetic analysis of benign and malignant breast lesions with ultrafast dynamic contrast-enhanced MRI: comparison with standard kinetic assessment. AJR Am J Roentgenol, 2016. 207(5): p1159.
3) Goto M, et al., Diagnostic performance of initial enhancement analysis using ultra-fast dynamic contrast-enhanced MRI for breast lesions. Eur Radiol, 2018.
4) Onishi N et al. Ultrafast dynamic contrast-enhanced MRI of the breast using compressed sensing: separate visualization of breast arteries an veins. JMRI, 2017
5) Honda M et al. New Parameters of Ultrafast Dynamic Contrast Enhanced Breast MRI Using Compressed Sensing JMRI 2019
Figures
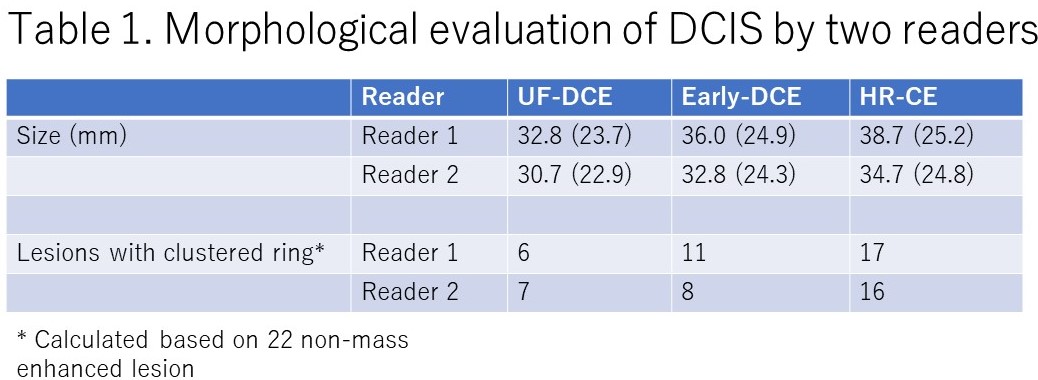

Figure 1. Difference between lesion size on UF-DCE, early DCE and HR-CE and that on pathology.
Difference between lesion size on MRI and pathology was smaller on UD-DCE, compared to that on Early –DCE and HR-CE for both readers. Difference was smaller on Early-DCE compared to that on HR-CE. (Wilcoxon signed rank test, p<0.01, indicated by *)