1415
Safety and imaging performance of 2-channel RF shimming for fetal MRI at 3T1Fetal-Neonatal Neuroimaging and Developmental Science Center, Boston Children's Hospital, Boston, MA, United States, 2Department of Pediatrics, Harvard Medical School, Boston, MA, United States, 3Department of Radiology, Harvard Medical School, Boston, MA, United States, 4Department of Electrical Engineering and Computer Science, Massachusetts Institute of Technology, Cambridge, MA, United States, 5Harvard-MIT Division of Health Science and Technology, Massachusetts Institute of Technology, Cambridge, MA, United States, 6Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Charlestown, MA, United States
Synopsis
3T MRI provides increased SNR but poses technical challenges for fetal imaging such as increased field inhomogeneity and SAR. RF shimming can address some of these challenges but also adds safety considerations. Using a diverse set of 5 numerical pregnant body models generated from patient MRI datasets, we found that 2-channel RF shimming can improve transmit field amplitude and uniformity by up to 19% and 36% respectively without increasing maternal or fetal SAR. The biggest difference in SAR and transmit field patterns was observed between the supine models and the left lateral model.
Target audience
MR physicists and clinicians interested in RF safety of 3T fetal imaging.Introduction
3T MRI can improve the quality of fetal imaging compared to the more established 1.5T MRI due to improved SNR1,2. However, transmit field inhomogeneities and specific absorption rate (SAR) concerns at 3T can reduce this gain and limit imaging speed3. Parallel transmission (pTx)4–6 has the potential to mitigate transmit field inhomogeneities and reduce SAR and several 3T scanners today already utilize two channel pTx systems. However, the safety of pTx systems for fetal imaging is severely understudied. Moreover, one previous study7 found that two-channel RF shimming can significantly increase fetal SAR and advised restriction to circularly polarized (CP) birdcage mode for pregnant subjects. They used three pregnant body models with different gestational ages (3-, 7- and 9-month-old) all artificially generated from the same non-pregnant female body model. In this study, we examine RF safety of two channel RF shimming at 3T for a more diverse set of numerical pregnant body models with differing posture, BMI, arms’ position and gestational age generated from MRI data of actual pregnant subjects8.Methods
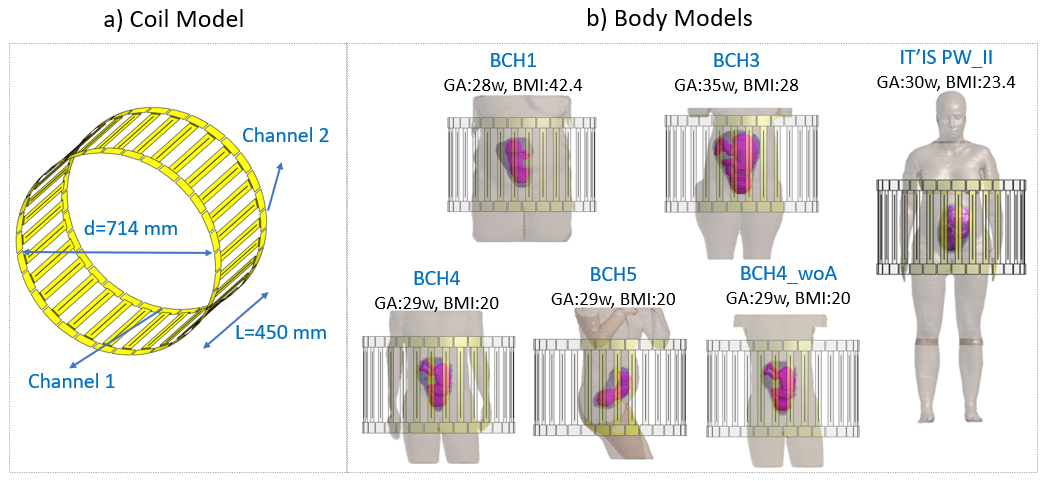
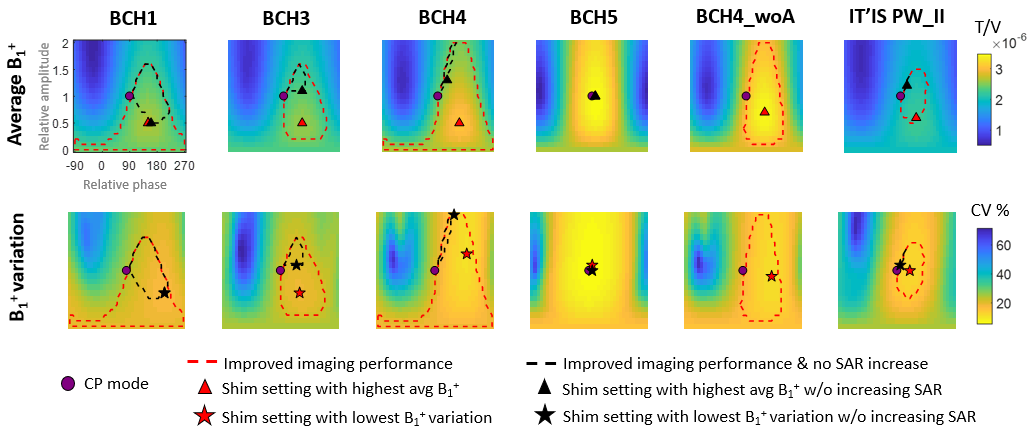
We utilize 5 pregnant numerical body models previously generated8; BCH1, BCH3, BCH4, BCH5, and BCH4_woA as well as the 7-month-old model by the IT’IS Foundation9, called "PW_II" in short. The fetal tissues in PW_II were simplified to two tissue classes, “fetal brain” and “fetus”, similar to the BCH models. These body models were loaded into a 2-channel 32-rung high pass birdcage body coil, tuned to 123.2 MHz, as shown in Figure 1. All tissue dielectric properties were assigned according to the IT’IS database10 except “fetus”, “fetal brain” (Hand et al.11), and “amniotic fluid” (Peyman et al.12). Electromagnetic simulations were carried out using Sim4Life (Zurich MedTech, Zurich, Switzerland). Virtual observation points (VOPs)13 were computed with an overestimation factor of 1% and used to estimate maternal and fetal peak 10g-averaged local SAR (pSAR10g). Maternal and fetal SAR were calculated for a range of RF shim settings where the relative amplitude and phase of the two channels was varied from 0 to 2 (steps of 0.1) and -90° to 270° (steps of 10°) respectively. CP mode corresponds to a relative amplitude/phase of 1/90°. In order to quantify imaging performance, average B1+ and variation of B1+ (coefficient of variation, CV) inside the fetus were calculated similarly to Murbach et al.7 for each model and RF shim setting. All SAR and B1+ values were normalized to whole-body average SAR of 2 W/kg.Results
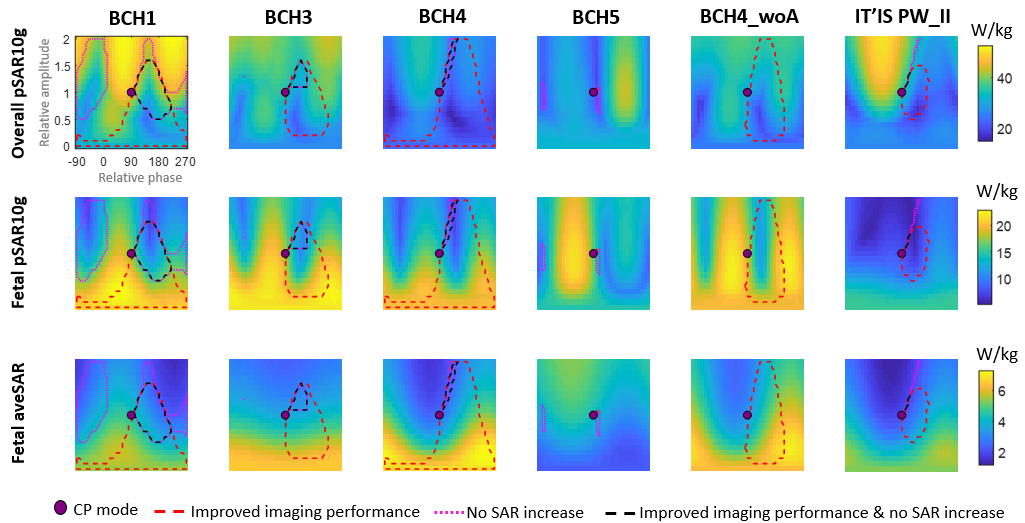
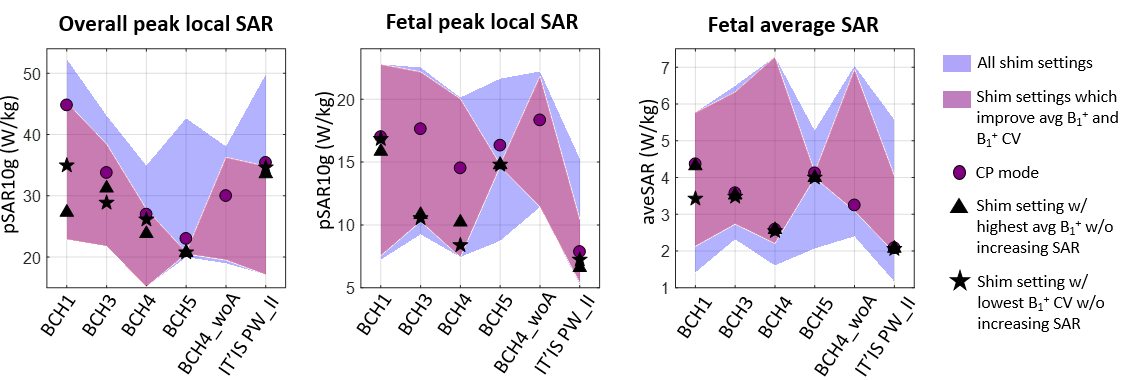
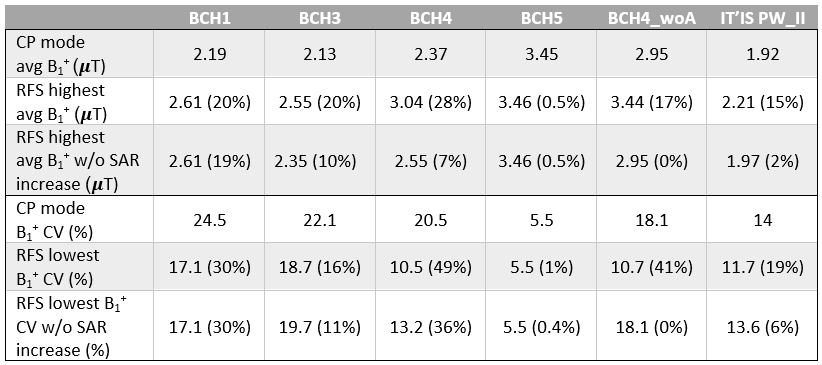
Figure 2 shows the average B1+ and B1+ variation patterns for the specified RF shim settings for all models. Imaging performance patterns are mostly similar across models except for the one in the left lateral position. Figure 3 shows overall (maternal and fetal) and fetal pSAR10g and fetal average SAR (aveSAR) patterns. In general, overall pSAR10g and fetal SAR have roughly opposite patterns as reported in Murbach et al.7 Overall pSAR10g and fetal pSAR10g values as well as fetal aveSAR values across all models are compared in Figure 4. CP mode fetal and maternal SAR vary significantly (by a factor of 1.9-2.3) among models as reported in Abaci-Turk et al.8. Maternal and fetal SAR varies by a factor of 3.5-6.2 across different RF shim settings and models. The highest average B1+ and lowest B1+ variation achievable with RF shimming (with or without increasing maternal and fetal SAR compared to CP mode) are described in Table 1.Discussion
RF shimming can improve average B1+ and B1+ variation inside the fetus by up to 28% and 49% respectively while keeping the whole-body average SAR at 2 W/kg. Without increasing maternal or fetal SAR compared to each model’s corresponding CP mode SAR levels, RF shimming can improve average B1+ and B1+ variation by up to 19% and 36% respectively (Table 1). Note that for models with low CP mode SAR values, restricting SAR to below that of the CP mode is more limiting compared to models with high CP mode SAR values. Safety of RF shimming for fetal MRI should be further investigated by temperature simulations7,14 to determine SAR levels that could be considered “safe” for all subjects. This way, SAR constraints for models with low CP mode SAR values (such as IT’IS PW_II and BCH4_woA) might be relaxed, improving the imaging performance of “safe” RF shimming. Both imaging performance and SAR patterns vary most significantly between the left lateral model and the supine models. Imaging performance patterns depend on the chosen ROI, which was the entire fetus for this study (similar to Murbach et al.7). In the future, we will repeat the same analysis for when the ROI is the uterus. In order to improve computational efficiency in the estimate of SAR for hundreds of shim settings and 6 different body models, we used VOP matrices computed from interpolated fields (from a nonuniform grid onto a uniform grid). This introduced up to 9% error for the CP mode SAR values. Finally, motion is an inevitable part of fetal MRI and its effect on B1+ and SAR patterns will be studied in the future.Acknowledgements
This work was supported by R01EB017337, U01HD087211, R01EB006847, P41EB015896, PS1 4000002543, Siemens MR.References
1. Krishnamurthy U, Neelavalli J, Mody S, et al. MR imaging of the fetal brain at 1.5T and 3.0T field strengths: comparing specific absorption rate (SAR) and image quality. J Perinat Med. 2015;43(2):209-220. doi:10.1515/jpm-2014-0268
2. Victoria T, Johnson AM, Edgar JC, Zarnow DM, Vossough A, Jaramillo D. Comparison Between 1.5-T and 3-T MRI for Fetal Imaging: Is There an Advantage to Imaging With a Higher Field Strength? AJR Am J Roentgenol. 2016;206(1):195-201. doi:10.2214/AJR.14.14205
3. Soher BJ, Dale BM, Merkle EM. A review of MR physics: 3T versus 1.5T. Magn Reson Imaging Clin N Am. 2007;15(3):277-290, v. doi:10.1016/j.mric.2007.06.002
4. Katscher U, Börnert P, Leussler C, Brink JS van den. Transmit SENSE. Magn Reson Med. 2003;49(1):144-150. doi:10.1002/mrm.10353
5. Zhu Y. Parallel excitation with an array of transmit coils. Magn Reson Med. 2004;51(4):775-784. doi:10.1002/mrm.20011
6. Adriany G, Van de Moortele P-F, Wiesinger F, et al. Transmit and receive transmission line arrays for 7 Tesla parallel imaging. Magn Reson Med. 2005;53(2):434-445. doi:10.1002/mrm.20321
7. Murbach M, Neufeld E, Samaras T, et al. Pregnant women models analyzed for RF exposure and temperature increase in 3TRF shimmed birdcages. Magn Reson Med. 2017;77(5):2048-2056. doi:10.1002/mrm.26268
8. Turk EA, Yetisir F, Adalsteinsson E, et al. Individual variation in simulated fetal SAR assessed in multiple body models. Magn Reson Med. 2020;83(4):1418-1428. doi:10.1002/mrm.28006
9. Gosselin M-C, Neufeld E, Moser H, et al. Development of a new generation of high-resolution anatomical models for medical device evaluation: the Virtual Population 3.0. Phys Med Biol. 2014;59(18):5287-5303. doi:10.1088/0031-9155/59/18/5287
10. Hasgall P, Gennaro F, Baumgartner C, et al. IT’IS Database for thermal and electromagnetic parameters of biological tissues. 2018;4. doi:10.13099/VIP21000-04-0
11. Hand JW, Li Y, Thomas EL, Rutherford MA, Hajnal JV. Prediction of specific absorption rate in mother and fetus associated with MRI examinations during pregnancy. Magn Reson Med. 2006;55(4):883-893. doi:10.1002/mrm.20824
12. Peyman A, Gabriel C. Dielectric properties of rat embryo and foetus as a function of gestation. Phys Med Biol. 2012;57(8):2103-2116. doi:10.1088/0031-9155/57/8/2103
13. Eichfelder G, Gebhardt M. Local specific absorption rate control for parallel transmission by virtual observation points. Magn Reson Med. 2011;66(5):1468-1476. doi:10.1002/mrm.22927
14. Hand JW, Li Y, Hajnal JV. Numerical study of RF exposure and the resulting temperature rise in the foetus during a magnetic resonance procedure. Phys Med Biol. 2010;55(4):913-930. doi:10.1088/0031-9155/55/4/001
Figures