1388
Detecting Respiratory Motion Using Accelerometer Sensors: Preliminary Insight1Radiology, New York University School of Medicine, New York, NY, United States, 2New York University Grossman School of Medicine, New York, NY, United States
Synopsis
MRI scans are often under continues involuntary motion which weakens their reliability and diagnostic utility for examining the chest and abdomen. Acquisitions using traditional external sensors (e.g. respiratory belt) and self-gated techniques tend to be highly sensitive to patient position and setup, and on MR sequence parameters. Here, we demonstrate the use of accelerometer sensors for detecting respiratory signals. We show how the use of this simple sensor, with its relatively small dimensions, high sampling rate capability, and low cost, can produce motion corrected-images under free-breathing conditions.
INTRODUCTION
The relatively slow acquisition timing of MRI challenges its applicability in many types of anatomical exams. Long acquisition durations are not only a burden for patients but also can lead to motion artifacts caused by physiological movements such as cardiac and respiratory motion (1). A common mitigation strategy in clinical routines include the use of external sensors (2) such as respiratory belts. This technique is not always robust and tends to be time-consuming to achieve the best motion sensitivity signal. Alternatively, self-gated (3-4) techniques directly extract motion from k-space, allowing tracking of motion via MR signal changes of the complete object. However, this approach tends to depend strongly on the slice orientation and imaging parameters (e.g. TR, number of slices). In this work, we demonstrate an alternative approach for detecting respiratory motion using external MR-compatible accelerometer sensors. Following our recent work on motion detection using a wireless RF transmitter (5-6), here we explore a simple, open-source, and low-cost (<$300) option for using wired accelerometers sensors. The accelerometer approach was tested with a radial MR sequence and was compared to conventional methods for motion correction, demonstrating comparable results.METHODS
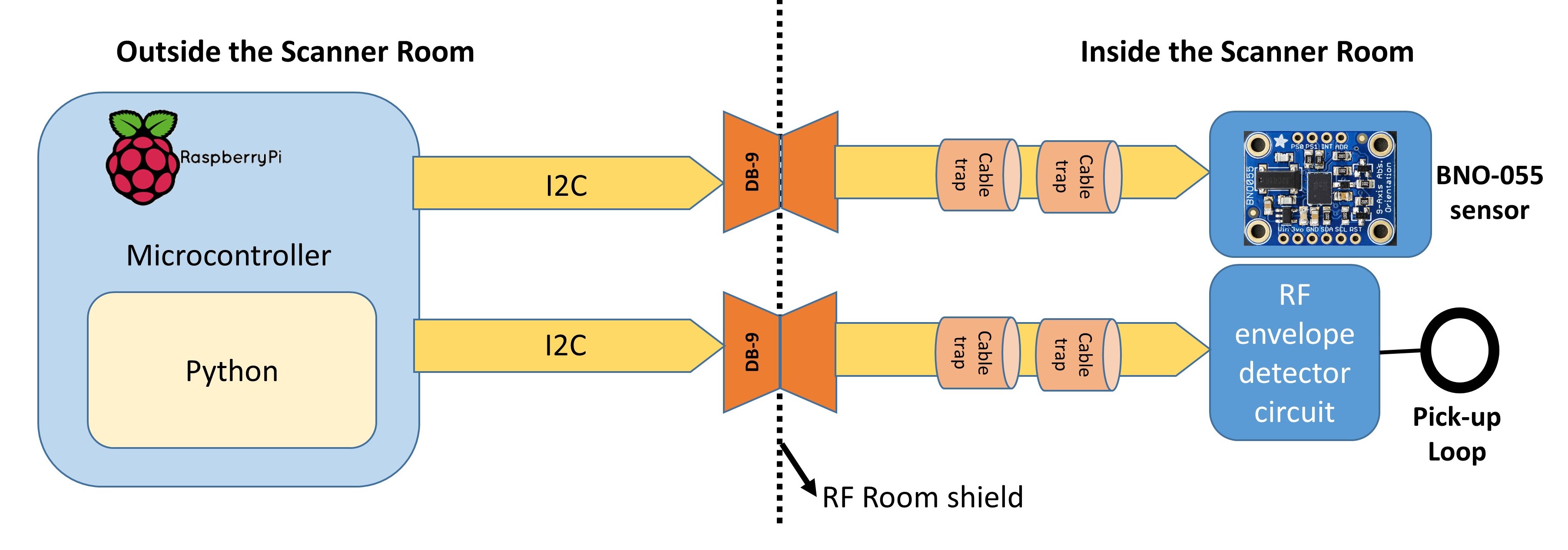
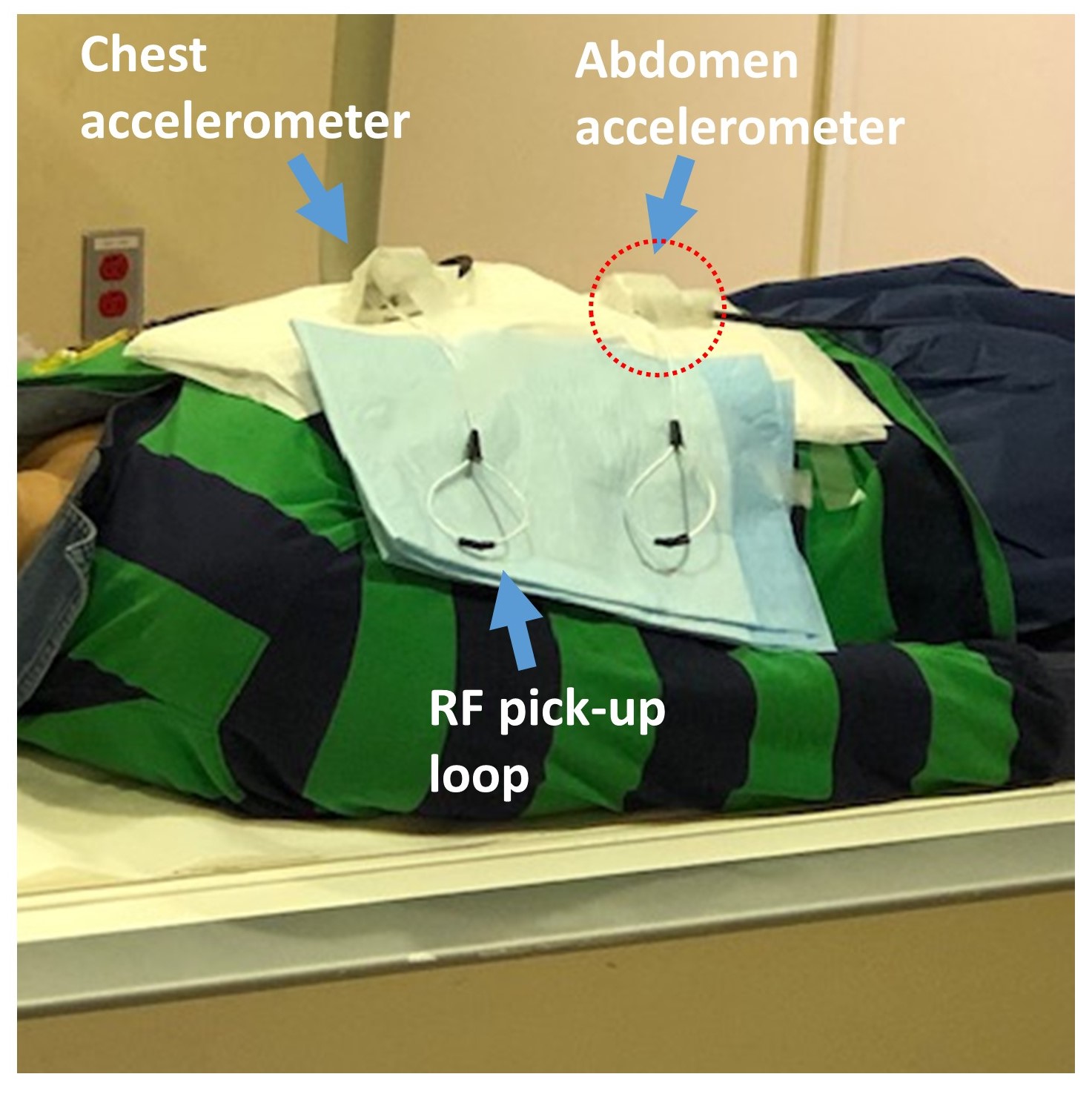
Sensor setup: Sensors were controlled by a Raspberry Pi computer run on Debian Linux and placed outside the scanner room (Fig. 1). Equipped by shielded cables, the accelerometer (BNO-055, Adafruit Industries LLC.) and RF detector were connected from the control room into the scanner room, through the RF penetration panel. The accelerometer was placed on top of the abdomen of the subject to ensure proper monitoring of the breathing motion. In this study, we have chosen to explore only the abdomen sensor (Fig. 2, circled in red) since this sensor was expected to have the most dominant motion signal. The RF detector circuit includes a pick-up loop connected to an RF envelope detector that senses the RF pulses and triggers the recording of the accelerometer sensor. Both the RF detector and accelerometer are controlled by a dedicated python script, enabling a sampling rate of 50ms. Once executed, the accelerometer measurements are presented in a graphical user interface (GUI) plotting the acceleration in x-, y-, and z-directions and saving the data to a text file. We have also explored the use of an RF transmitter device for the detection of motion, termed ‘Pilot-Tone’. The Pilot-Tone is a small wireless device placed outside the MR bore with no direct contact with the patient that has been shown to be effective for motion tracking (5-6).Imaging: Images were acquired on a 3T Prisma system (Siemens Healthcare, Erlangen, Germany) using a body coil array. The study protocol included a free-breathing radial stack-of-stars 3D GRE (RAVE) sequence with golden-angle acquisition. RAVE imaging parameters included TR/TE=5.0/1.7ms, BW=500Hz/pixel. Scans were conducted while the patient was instructed to follow different breathing conditions: 1) Deep breathing, 2) Breath-holds. 3) Hyperventilation (shallow and rapid breathing), 4) Normal physiological breathing. Fig. 3 (conditions 1-3) and Fig. 4 (condition 4) were acquired with 24-48 slices, 400 radial views, 1.4 mm in-plane resolution and 3 mm slice thickness. Fig. 5 (condition 4) was acquired with 120 slices and 1.3 mm isotropic resolution.
Post-processing: After the accelerometer measurements were recorded and saved, the signals were smoothed by a Savitzky–Golay filter and normalized. The respiratory signal was processed by eXtra-Dimensional (XD) reconstruction pipeline (4), which bins the continuously acquired radial data into different respiratory states and use compressed-sensing to exploit correlations between the motion states.
RESULTS AND DISCUSSION
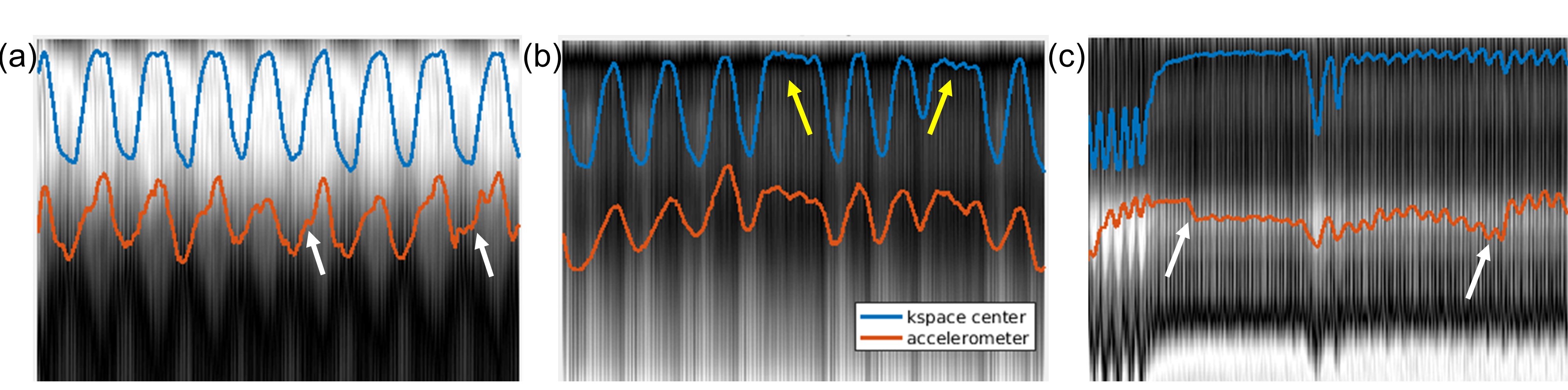
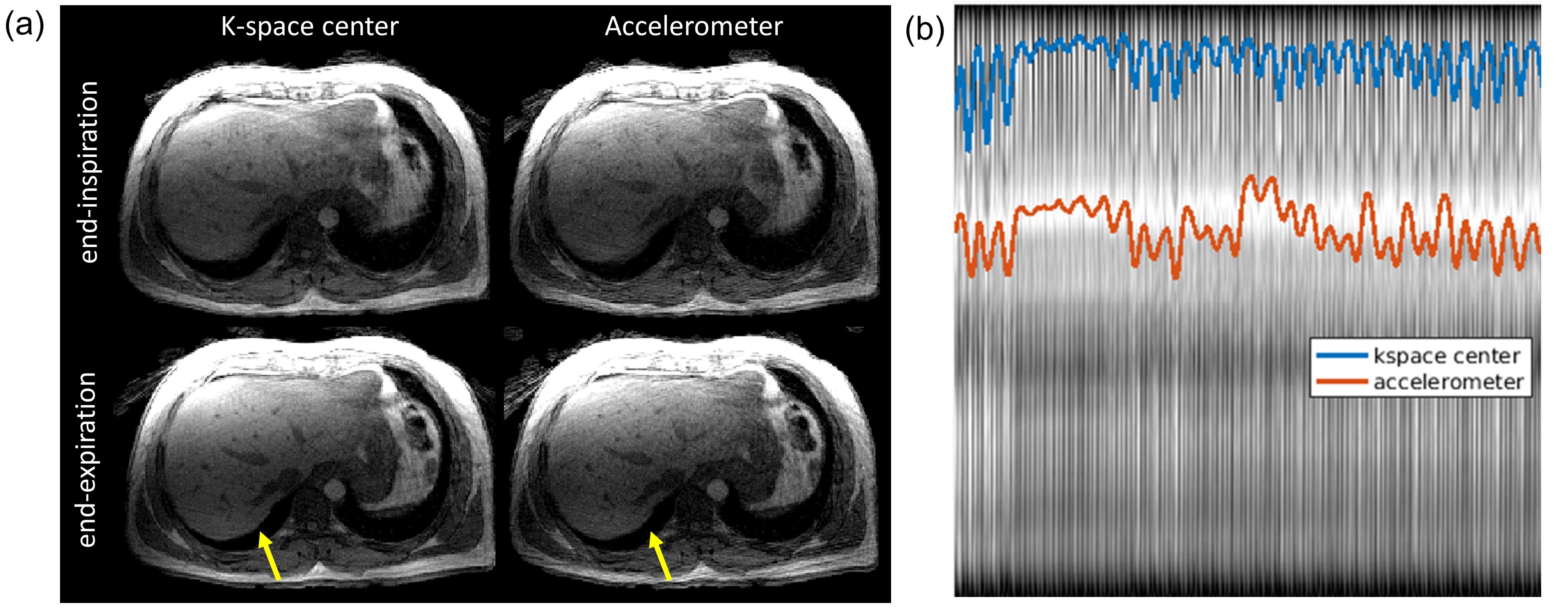
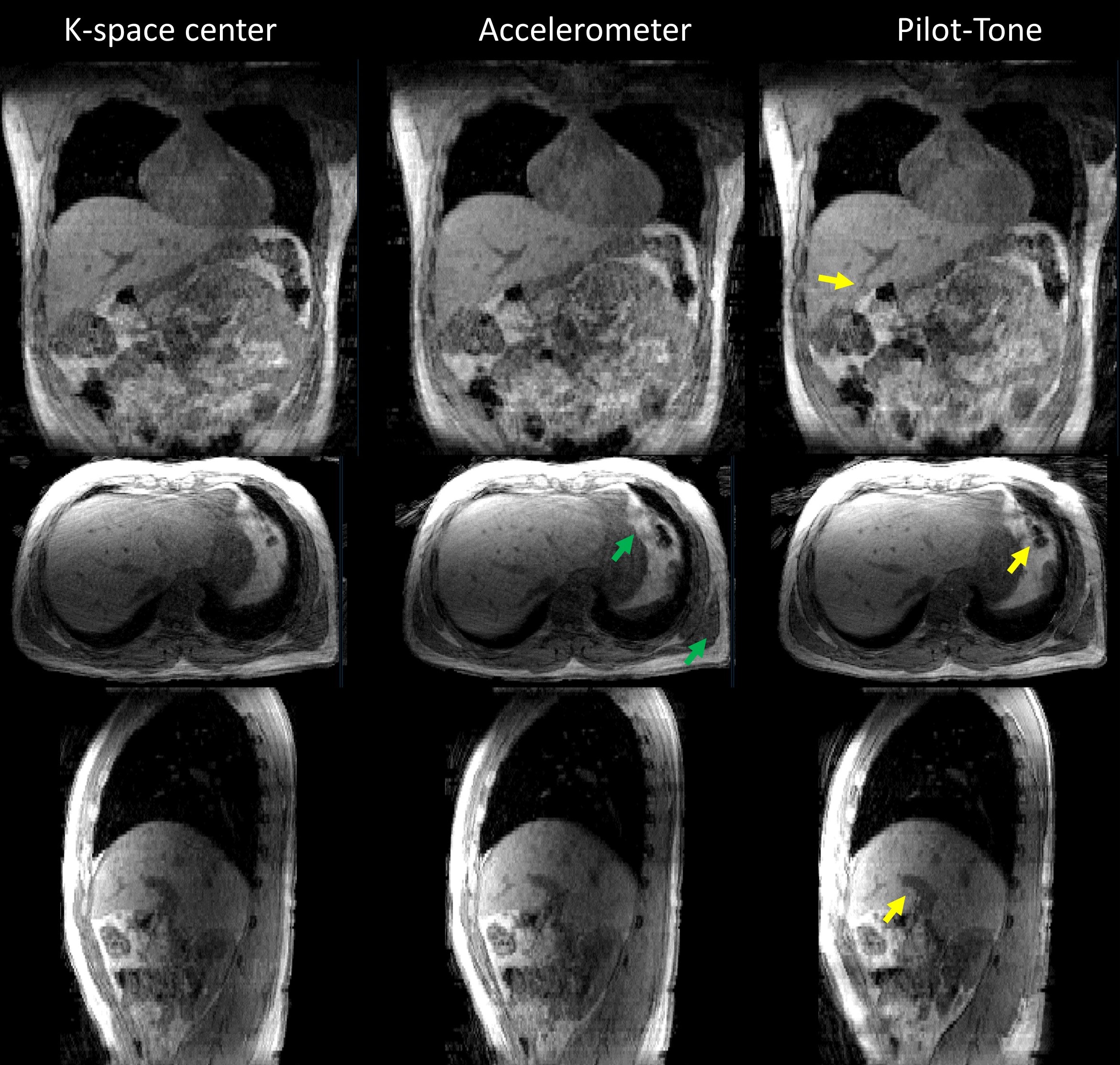
When comparing respiratory signals from the k-space self-navigation signal (Fig. 3, blue), and the accelerometer (Fig. 3, red), similar patterns were seen for the deep breathing (Fig. 3a, cond. 1), breath-holds (Fig. 3b, cond. 2), and hyperventilation (Fig. 3c, cond. 3). Interestingly, the signal recorded by the accelerometer included small changes in breathing patterns (Fig. 3a, see white arrows) which implies its high precision capability. However, during hyper-ventilation, signals recorded by the accelerometer (without correction) seemed susceptible to drift artifacts (Fig. 3c, see while arrows). Next, the MR data was sorted and binned to four respiratory states from end-inspiration to end-expiration (Fig. 4a). Data binned by the k-space center signals (Fig. 4b, blue) and by the accelerometer signal (Fig. 4b, red) showed comparable anatomical details and sharper liver tip in the end-expiration state (indicated by yellow arrows). Moreover, a slightly more stable respiratory signal provided by k-space center (Fig. 4a, blue) resulted in less streak artifacts, compared to data binned by the accelerometer. In a 1.3 mm isotropic 3D view (Fig. 5), the use of the accelerometer signal resulted in fine tissue boundaries (indicated by green arrow) relative to the k-space center method. Additionally, in this scan we compared our recent Pilot-Tone RF transmitter (right column) to k-space center (left column) and accelerometer signals (middle column). Due to its high sampling rate (TR, 5ms), data binned using Pilot-Tone showed finer liver anatomical details (indicated by yellow arrows).CONCLUSION
An MR-compatible accelerometer sensor showed reliable results in tracking motion when compared to conventional k-space self-navigation and Pilot-Tone. Its small dimensions, flexible high sampling rate, and low-cost makes it a good solution for tracking breathing motion in the MRI environment.Acknowledgements
We acknowledge support from NIH grant P41 EB0171813 and R01 5R01EB018308.References
1. Havsteen I, Ohlhues A, Madsen KH, Nybing JD, Christensen H, Christensen A. Are Movement Artifacts in Magnetic Resonance Imaging a Real Problem?-A Narrative Review. Front Neurol 2017;8:232.
2. Zaitsev M, Maclaren J, Herbst M. Motion artifacts in MRI: A complex problem with many partial solutions. J Magn Reson Imaging 2015;42(4):887-901.
3. Zhang T, Cheng JY, Chen YX, Nishimura DG, Pauly JM, Vasanawala SS. Robust Self-Navigated Body MRI Using Dense Coil Arrays. Magnetic Resonance in Medicine 2016;76(1):197-205.
4. Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn Reson Med. 2016 Feb;75(2):775-88.
5. Solomon E, Rigie DS, Vahle T, Paška J, Bollenbeck J, Sodickson DK, Boada FE, Block KT, Chandarana H. Free-breathing radial imaging using a pilot-tone radiofrequency transmitter for detection of respiratory motion. Magn Reson Med. 2020 Dec 11. doi: 10.1002/mrm.28616. 6. Speier P, Fenchel M, Rehner R, PT-Nav: a novel respiratory navigation method for continuous acquisitions based on modulation of a pilot tone in the MR-receiverProc. ESMRMB 2015, 128: 97-98.
Figures