1382
Minimizing motion artifacts in myocardial quantitative mapping by combined use of motion-sensitive CINE imaging and FEIR
Takumi Ogawa1, Michinobu Nagao2, Masami Yoneyama3, Yasutomo Katsumata3, Yasuhiro Goto1, Isao Shiina1, Yutaka Hamatani1, Kazuo Kodaira1, Mamoru Takeyama1, Isao Tanaka1, and Shuji Sakai2
1Department of Radiological Services, Women's Medical University Hospital, tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Women's Medical University Hospital, tokyo, Japan, 3Philips Japan, tokyo, Japan
1Department of Radiological Services, Women's Medical University Hospital, tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Women's Medical University Hospital, tokyo, Japan, 3Philips Japan, tokyo, Japan
Synopsis
Myocardial mapping such as T1 and T2 is widely used clinically for evaluating the properties of myocardium. We evaluated the feasibility of the combined use of Motion-Sensitive (MoSe) CINE imaging for determining accurate TD setting and fast elastic image registration (FEIR), which is a registration-based nonrigid motion correction for minimizing the influence of cardiac motion-related artifacts.
Introduction
Myocardial quantitative mapping such as T1 and T2 map is useful in diagnosing cardiomyopathy, edema, inflammation, iron deposition, myocardial infarction, and severity associated with fibrosis [1]. To obtain clinically acceptable myocardial quantitative maps, there are two important points especially for minimizing the influence of cardiac motion-related artifacts: choice of exact cardiac trigger delay (TD) and image registration-based motion correction. Commonly, the exact TD for the acquisition is determined by using system automatic pre-set timing, but there is still sub-optimal choice of TD in some cases, resulting in deterioration of quantitative accuracy. Recently, we proposed a Motion-Sensitive (MoSe) CINE imaging for determining accurate TD setting which leads to increase the robustness of image quality in quantitative myocardial mapping [2]. On the other hand, small motions of the heart may still occur due to motion of the diaphragm, variations in R-R interval, and due to failed breath holding. For myocardial mapping, these variations of in-plane heart shape can be mitigated by registering the source images before creation of the parametric map. A method for the registration is called Fast Elastic Image Registration (FEIR) [3]. FEIR has proven accurate in cardiac T1 mapping [4]. In this study, we evaluated the feasibility of the combined use of MoSE CINE imaging (to determine exact TD) and FEIR (to register the respective phase/TE images) for improving the robustness of quantitative cardiac T1 and T2 mapping.Methods
A total of five volunteers were examined on a 3.0T system (Ingenia, Philips Healthcare). The study was approved by the local IRB, and written informed consent was obtained from all subjects. We compared MOLLI T1mapping and T2prep-based T2mapping [5] with/without MoSe-CINE approach and FEIR. MoSe-CINE imaging is based on T2FFE sequence, could clearly visualize the motion-insensitive cardiac-phase timing (especially, when is the accurate systole or diastole) due to its motion sensitivity (Figure 1). Visually confirming the MoSe-CINE imaging could be useful for optimal TD selection. First, we compared two procedures in respective T1 and T2 mapping acquisition: one is conventional approach (operator set the preset TD timing for diastole and TD was automatically determined by MR system software) and visual approach using MoSE-CINE (operator visually defined the diastole and check whether heart structure is not obscured by cardiac movements at the determined TD). Subsequently we applied FEIR after image reconstruction for both conventional approach and using MoSE-CINE images respectively. Consequently, we obtained four image datasets and we compared the image quality. To evaluate quantitatively, regions-of-interest (ROIs) were placed on 16 segments of the myocardium in the short axis image of the left ventricle [6], standard deviation (SD) of relaxation times in respective ROIs were compared among all datasets. Imaging parameters for… MOLLI T1mapping imaging: TFE, FOV=300mm, pixel size=1.97*2.02mm, slice thickness=8mm, flip angle=20, TR=2.1ms, TE=0.97ms, NSA=1, SENSE=2 and acquisition time=11s. T2prep-based T2mapping: TFE, FOV=300mm, pixel size=1.97*2.02mm, slice thickness=8mm, flip angle=20, TR=1.90ms, TE=0.68ms, NSA=1, SENSE=2 and acquisition time=12s. MoSe-CINE imaging: T2FFE with free-breathing and retrospective cardiac gating, FOV=380mm, pixel size=2.64*1.7mm, slice thickness=12mm, flip angle=25, number of heart phase=32, TR=6.6ms, TE=3.7ms, ProSet water excitation 121, NSA=16, and acquisition time=2m55s.Results & Discussion
Figure 2 and 3 shows the examples of comparison among conventional and MoSE-CINE visual approach with/without FEIR post-processing. In Figure 2, both conventional MoSE-CINE visual approach with FEIR clearly improved the accuracy on T1 confidence map and the combination of MoSE-CINE visual approach with FEIR showed the best image quality. Likewise, in Figure 3, the combination of MoSE-CINE visual approach with FEIR most improved the image quality of T2map. Combined use of MoSe-CINE approach and FEIR indicated lowest rSD for 16-segment ROIs on the T1map [Fig.4], which reflects improved image uniformity, compared with other combinations.Conclusion
Combined use of the MoSe-CINE imaging, to determine the exact cardiac trigger delay, and FEIR, to register among all source images, could be useful to increase the robustness of image quality and improve the quantitative accuracy in myocardial mapping.Acknowledgements
No acknowledgements found.References
[1]. Hamlin SA, et.al. Mapping the future of cardiac MR imaging: case-based review of T1 and T2 mapping techniques. Radiographics. 2014 Oct; 34(6):1594-611. [2]. Shiina I, et al, Motion-Sensitive (MoSe) CINE imaging: utility for improving robustness of myocardial quantitative mapping. Proc. ISMRM:2020.2061 [3]. Kabus S, et al. Fast elastic image registration. Proc. MICCAI:2010. 81–89. [4]. Zhang S, et al. Cardiac magnetic resonance T1 and extracellular volume mapping with motion correction and co-registration based on fast elastic image registration. MAGMA. 2018 Feb;31(1):115-129. [5]. Yoneyama M, et al. Rapid free-breathing 3D isotropic whole-heart diastolic and systolic myocardial T2mapping. Proc. ISMRM:2020.2061 [6]. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation,105:539-42,2002.Figures
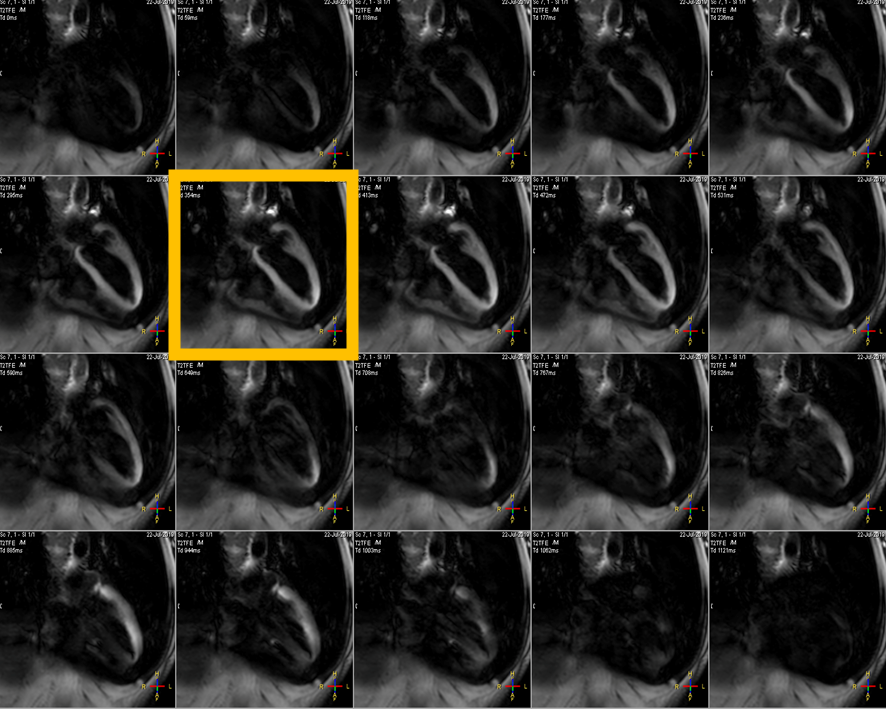
Figure.1 MoSe-CINE
images allows direct visualization of motion-independent cardiac phase timing. It shows depicted signal decrease due to cardiac
motion and it pointed out when is the best timing to trigger for both systolic
and diastolic timings.
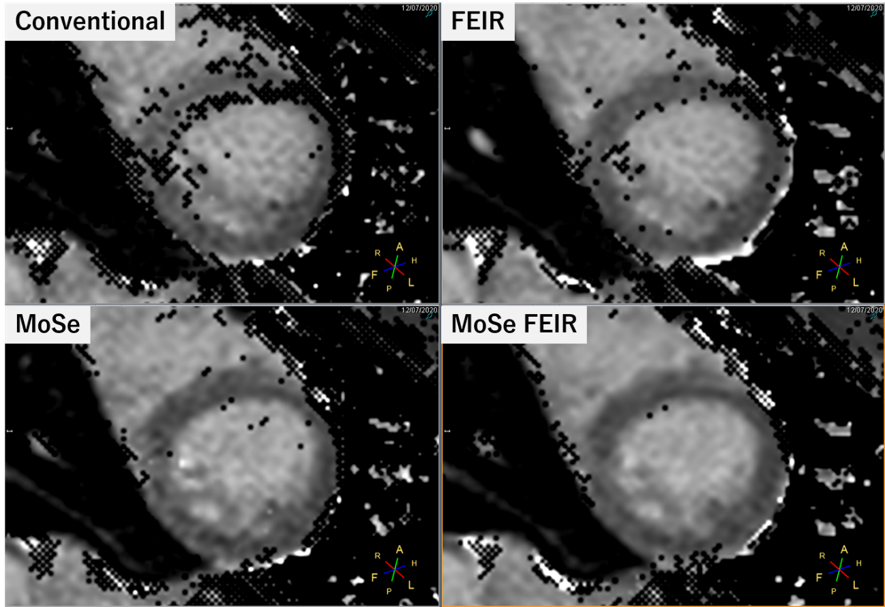
Figure.2 A comparison MOLLI T1mapping with/without MoSe-CINE approach and FEIR. Both
conventional MoSE-CINE visual approach with FEIR clearly improved the accuracy
on T1 confidence map and the combination of MoSE-CINE visual approach with FEIR
showed the best image quality.
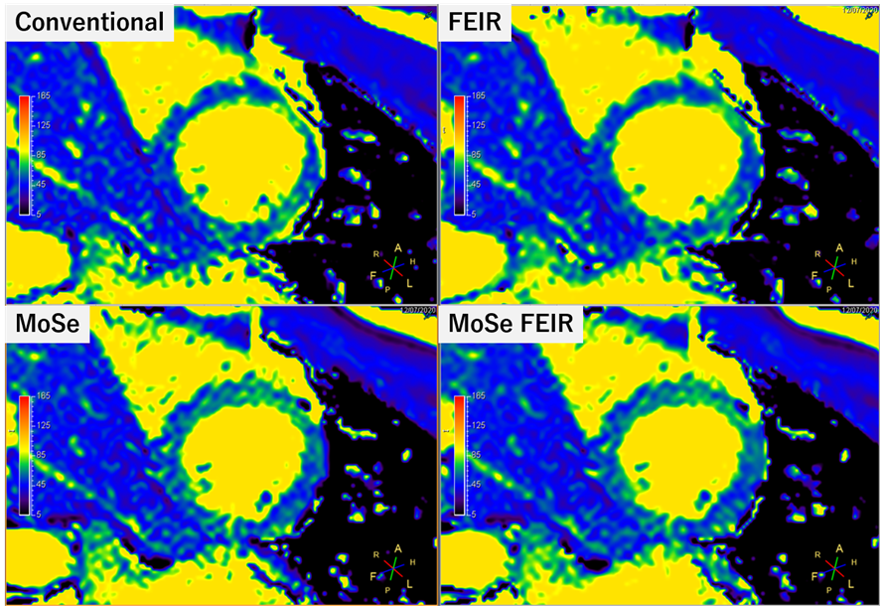
Figure.3 A comparison T2prep-based T2mapping
with/without MoSe-CINE approach and FEIR. The
combination of MoSE-CINE visual approach with FEIR most improved the image
quality of T2map.
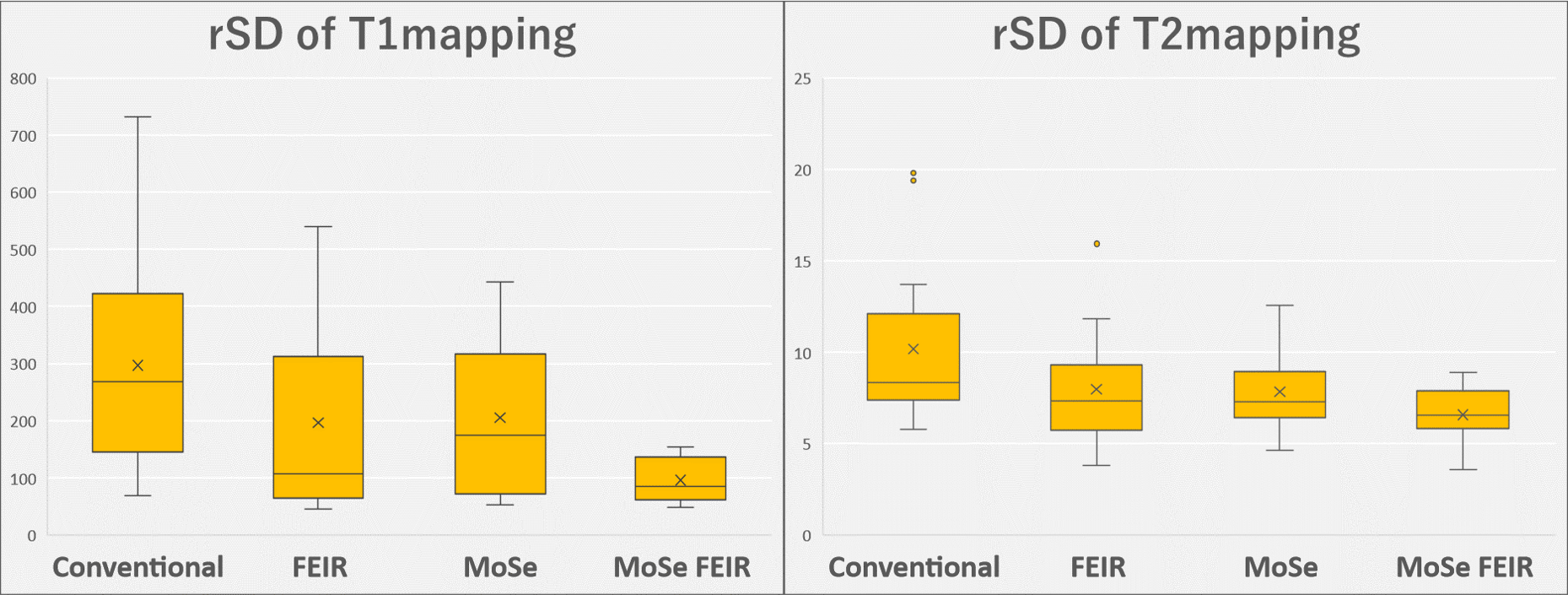
Figure.4 ROIs were placed on 16 segments of the myocardium
in the short axis image of the left ventricle, relative standard deviation (rSD)
of relaxation times in respective ROIs were compared among all datasets. Combined use of MoSe-CINE approach and FEIR
indicated lowest rSD, which reflects improved image uniformity, compared with
other combinations.