1380
Structure Light based Optical MOtion Tracking system (SLOMO) for Contact-free respiratory Motion Tracking from Neck in MR Imaging1Center for Biomedical Imaging Research, School of Medicine, Tsinghua University, Beijing, China, 2Philips Healthcare, Beijing, China
Synopsis
This study proposed a parallel line Structure Light based Optical Motion Tracking system (SLOMO) and verified its feasibility in respiratory detection and motion correction in MR liver imaging.
Introduction
Respiratory motion artifact is a common challenge during the abdominal MR imaging. Traditional solutions for respiratory compensation mostly rely on external contact sensor by trigger or gating method, which will truly induce uncomfortable constriction to patient and complicate scan procedures. In recent years, optical based depth visual technique has presented immense potential for 3D object motion tracking and human physiological signal extraction, due to its non-contact property, real time performance, and high accuracy and sensitivity[1,2]. However, traditional marker-based optical tracking system is incompetent to non-rigid motion. Our previous work has demonstrated the capability of SLOMO system for rigid head motion correction in MR brain imaging[3]. In this study, we aim to implement the SLOMO system into MRI non-rigid respiratory motion correction and to investigate its feasibility of extraction of respiration information.Method and materials
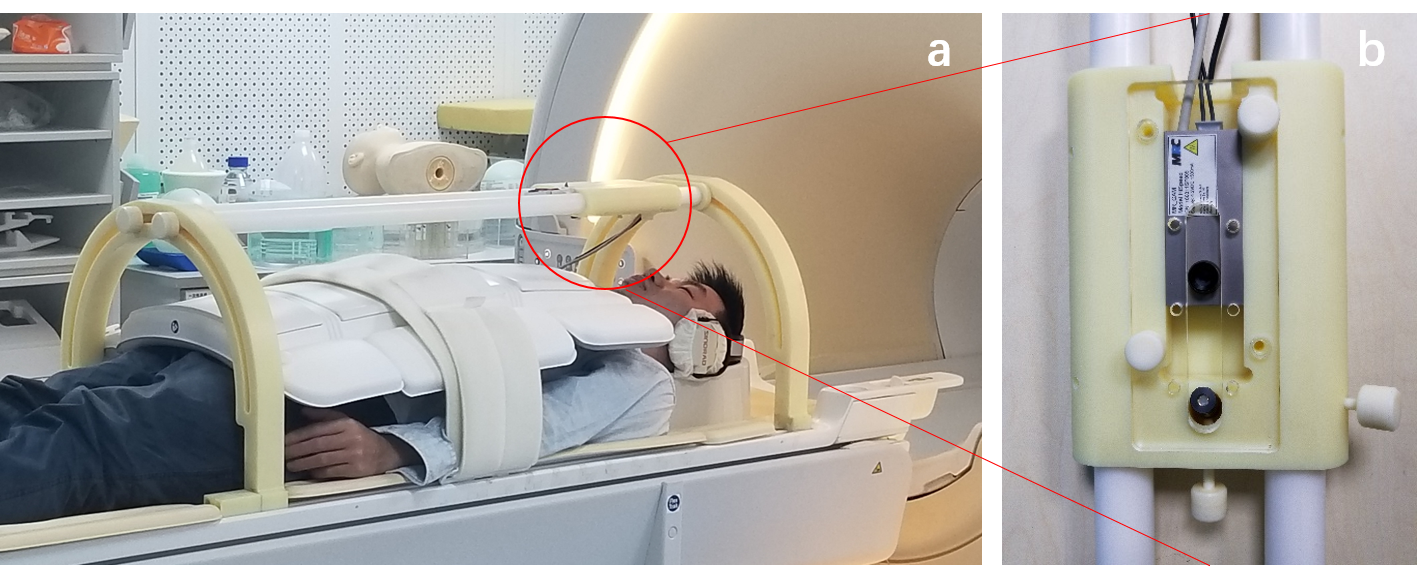
SLOMO systemThe setup of SLOMO system for abdominal imaging is composed of a MR compatible high-speed camera (250Hz, MRC, Germany), a 41 parallel-line infrared laser (980nm, 5mw) and a set of dedicated adjustable frame holders. Camera-laser system was pre-calibrated and packaged into a plastic box (Fig.1). This subsystem was hanged onto the suspension girder, that can be adjusted and fixed along the z and arc direction for the best field of view.
Image acquisition, processing and motion extraction
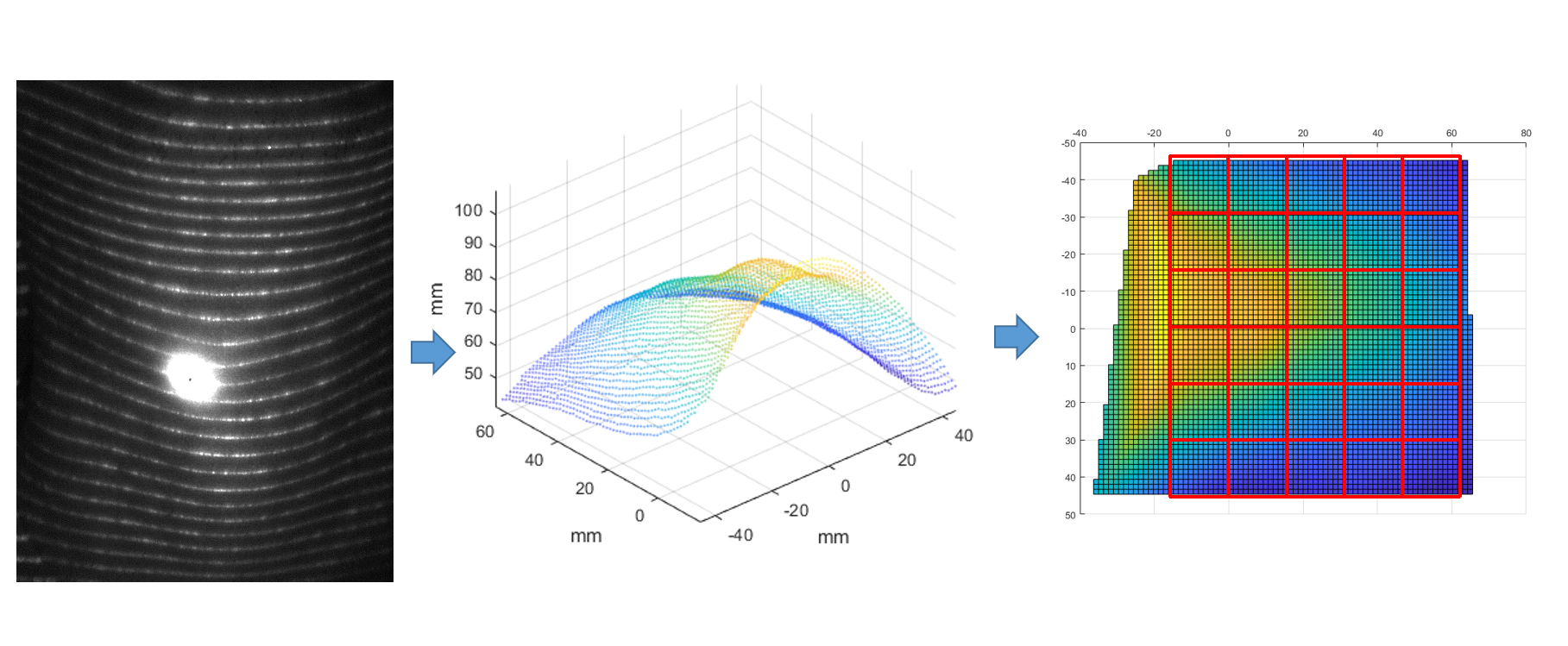
For Scanner-SLOMO synchronization, image acquisition controller on PC was triggered by scanner acq-trigger signal from spectrometer monitor port (delay<50μs) through USB. Laser beam were projected onto the subject’s neck. Image sequences were captured at the framerate of 30Hz, meanwhile, physiological signals from respiratory sensors (bellow) were logged in file. All the captured images will be reconstructed into 3D point clouds according to the calibration results by triangulation measurement (Fig.2). After the coordinate transformation from camera to scanner system, reconstructed neck surface will be cropped into M×N blocks (each block:1.5*1.5cm2). Temporal dynamic curve of each mean height of points within each block was taken for respiratory information detection.
In vivo study
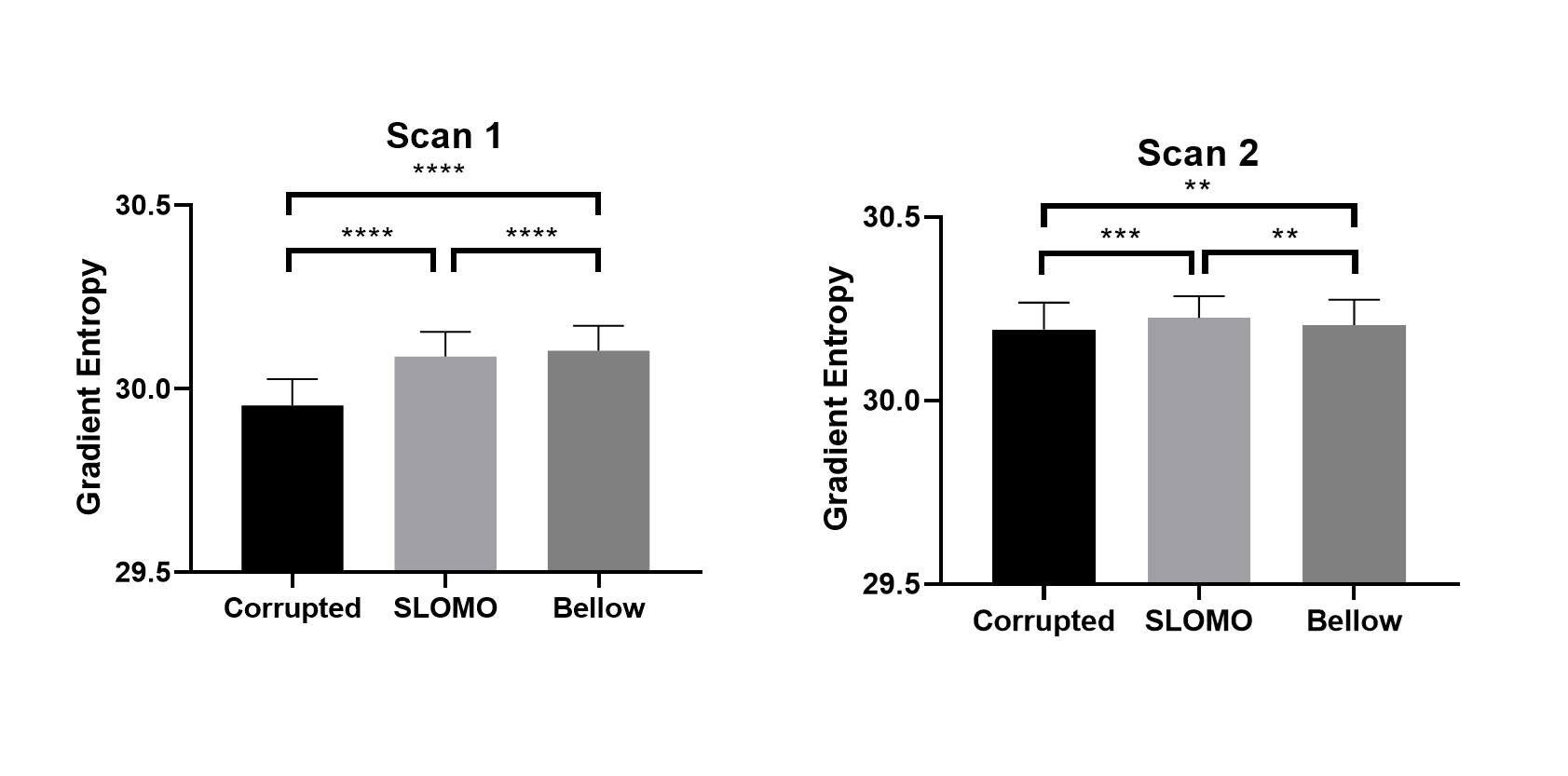
All the studies were performed on a Philips Ingenia CX 3.0T scanner (Philips, Best, The Netherlands) with a 26-channel abdominal coil. 2 healthy volunteers underwent Golden-Angle-Radial 3D TFE liver scan with following parameters: TR/TE=3.3/1.37ms; in-plane resolution=1.5×1.5mm2; slice thickness=3mm; slice number=67; flip angle=10°; FOV= 380×380mm2; in-plane over sampling=600%; acquisition time=6:03min. During each scan, subject was asked to breath freely until the end of the scan. Respiratory bellow was attached to subject. After obtained a series of height fluctuation curves from different neck parts, the curve that best presented the breathing pattern was manually selected. This curve was filtered by a band-pass FIR filter using Kaiser-Bessel window with passband between 0.2Hz and 0.6Hz and stopbands below 0.1Hz and above 0.7Hz[2]. Since signals from SLOMO system has been well synchronized with scanner sensor signals, the differences of respiratory peak time and breathing interval time between bellow and optical tracing curves were compared. Respiratory motion correction was conducted by grouping readout spokes into 4 respiratory bins[5] according to the bellow and optical tracing curves, respectively. Consistent number of spokes were used to reconstruct images of different respiratory phases using NUFFT algorithm. The gradient entropy[6] was used to quantified the sharpness of image before and after the motion correction.
Results
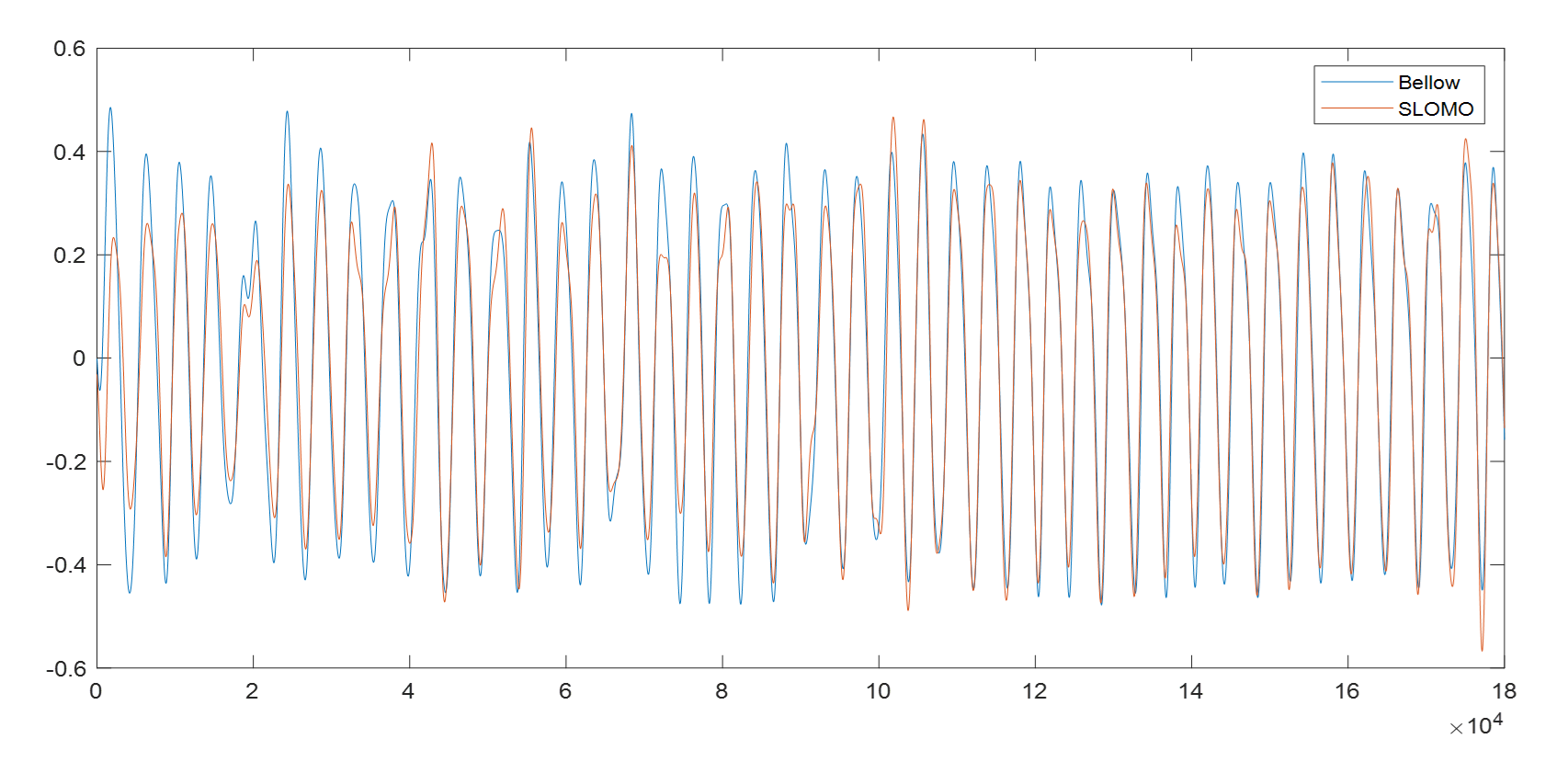
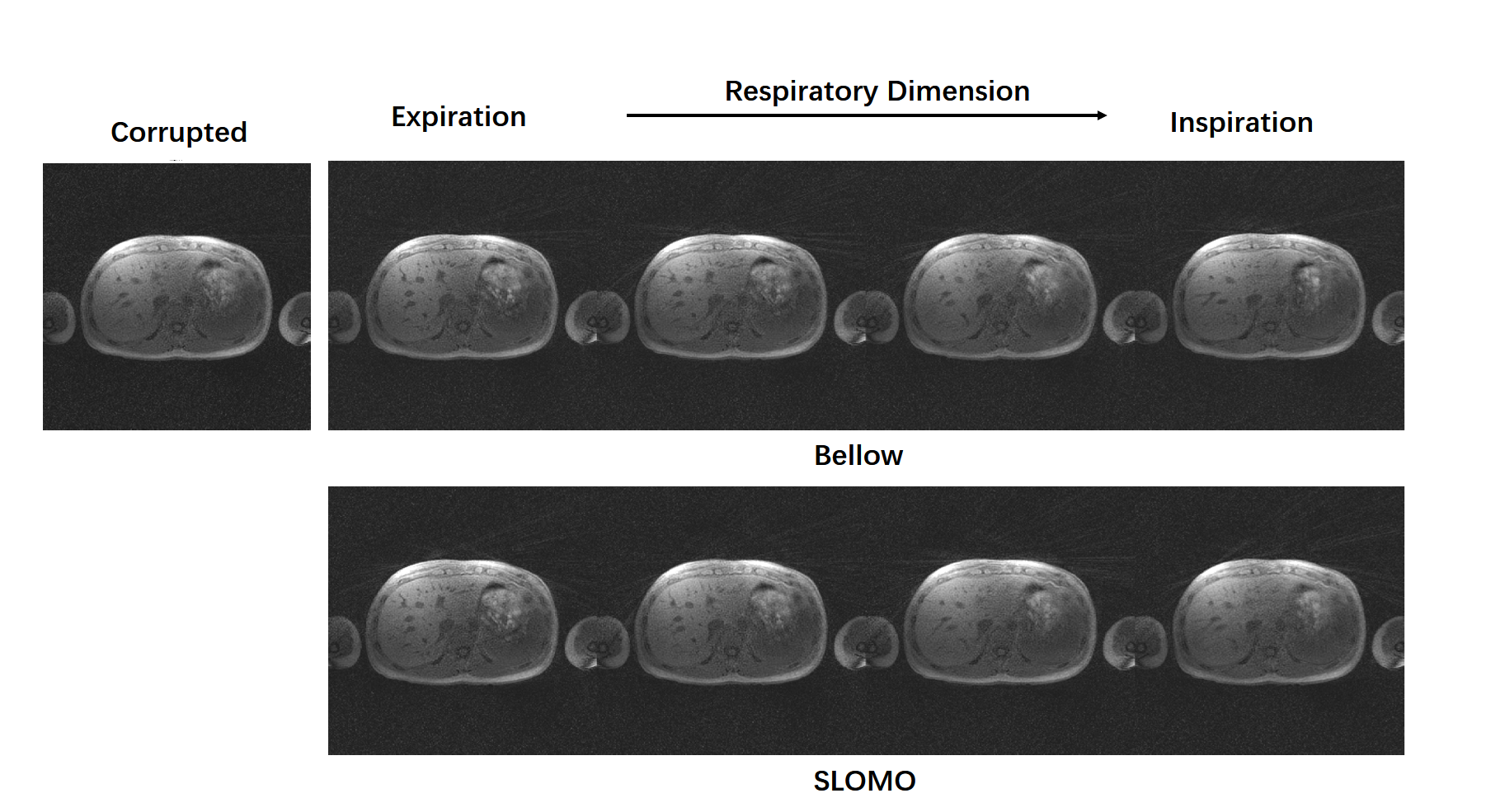
Fig.3 presents he alignment of bellow and SLOMO tracked respiratory curves. Compared with bellow’s, the mean difference of peak time is 61ms (0.26 spoke), the mean difference of peak interval is 19ms (0.02 spoke). No respiratory peak was missed. Images were successfully reconstructed into 4 respiratory phases with less blurring artefact and sharper structural boundary compared with corrupted one (Fig.4). Images reconstructed by optical tracking curve indicated the comparative image quality with that from bellow’s. The gradient entropies of bellow-corrected and SLOMO-corrected images are both significantly higher than corrupted images, which demonstrate the improved sharpness after correction (Fig.5).Discussion and conclusion
This study demonstrates the performance of SLOMO system on non-rigid motion tracking and respiratory motion corrections. Compared with cross-light tracking system[4], SLOMO system essentially solves the problem of light drift and provides more detailed motion tracking information. Comparison results of bellow and optical curves shows that breathing signal detected from neck is highly correlated with bellow with mean misalignment of 61ms. Reconstruction results also verified its capability of respiratory motion correction and sharpness improvement. In future, SLOMO system is expected to extract and recognize more complex motion patterns and physiological signals by the achievement of better pattern recognition algorithm and system stability.Acknowledgements
No acknowledgement found.References
1. Maclaren J, Herbst M, Speck O, Zaitsev M. Prospective motion correction in brain imaging: a review. Magn Reson Med 2013;69:621–636.
2. Maclaren J , Aksoy M , Bammer R . Contact-free physiological monitoring using a markerless optical system[J]. Magnetic Resonance in Medicine, 2015, 74(2):571-577.
3. Chunyao Wang, Chen Zhang,Wang Yu,Haikun Qi, Tianqi Huang, Jin Liu, Chun Yuan, Hongen Liao, Huijun Chen. Motion correction in Brain MR imaging using a Structure Light based Optical MOtion Tracking system (SLOMO). ISMRM 27th Annual Meeting & Exhibition, 11-16 May 2019. Montreal, QC, Canada.
4. Chen Zhang, Jin Liu, Jinnan Wang, Jiarui Cai, Chun Yuan, and Huijun Chen, Detection Arterial Pulsation Using Non-attached Optical Remote Motion Sensing (NORMS) System: a preliminary study; The 5th International Congress on Magnetic Resonance Imaging & 22nd Annual Scientific Meeting of KSMRM, Grand Hilton Hotel, Seoul, Korea, 3.23-3.25; 2017
5. Feng L , Axel L , Chandarana H , et al. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing[J]. Magnetic Resonance in Medicine, 2016, 75(2):775-788.
6. McGee KP, Manduca A, Felmlee JP, Riederer SJ, Ehman RL. Image metric-based correction (Autocorrection) of motion effects: Analysis of image metrics. J Magn Reson Imaging 2000;11:174–81.
Figures