1339
Validating the Accuracy of Multi-Spectral Metal Artifact Suppressed Diffusion-Weighted Imaging1Radiology and Imaging, Hospital for Special Surgery, New York, NY, United States, 2Medical College of Wisconsin, Wauwatosa, WI, United States
Synopsis
Diffusion-weighted MAVRIC is a novel pulse sequence that can obtain quantitative diffusion values in regions with high susceptibility. The goal of this work is to compare the quantitative accuracy of DWI-MAVRIC with sequences currently available on clinical MR scanners, using a diffusion phantom and images acquired at different orientation and spatial offsets in the scanner. Overall, good linearity with diffusivity was observed, with a large positive ADC bias at low diffusivity in both axial and coronal DWI-MAVRIC noted. Right and left spatial offsets increased ADC errors that can be mitigated by gradient nonlinearity correction.
Introduction
Diffusion weighted imaging (DWI) provides quantitative measurement of random water displacement(1), as calculated in an apparent diffusion coefficient (ADC) map. DWI is a promising tool for evaluating musculoskeletal tissues(2–4) but has had limited effectiveness in peri-prosthetic regions due to strong susceptibility artifacts from metallic components frequently found in orthopedic hardware(5). One solution is to utilize multispectral imaging (MSI) techniques, such as multi-acquisition with variable resonance image combination (MAVRIC)(6), which is an artifact-reducing technique that sums spectral bins to form a composite image containing less metal artifact than 3D-FSE acquisitions alone. Diffusion-weighted MAVRIC(7) is a recently-developed modification of the 2D PROPELLER DUO diffusion-weighted pulse sequence(8), which acquires multiple spectral bins and DUO encoded PROPELLER blades, allowing quantitative diffusion values to be obtained with low geometric distortion and improved signal in regions with high susceptibility. Since diffusivity is sensitive to alterations to tissue microstructure caused by disease(9), DWI-MAVRIC may provide a novel means for evaluating peri-prosthetic joint infection and avascular necrosis among other orthopedic conditions,. The goal of this work is to compare the quantitative accuracy of DWI-MAVRIC with standard EPI-readout-based DWI and diffusion tensor imaging (DTI) pulse sequences currently available on clinical MR scanners. This analysis is important, as there are many sources of quantitative bias such as spatial nonlinearity, imaging gradients, image distortion, and eddy currents.Methods
Phantom scanning was performed using a Diffusion Standard Model 128 (CaliberMRI, Boulder, CO). This phantom contains 13 vials of varying concentrations of the diffusivity-modifier polyvinylpyrrolidone(PVP) (three of: 0% wt/wt, two of: 10%,20%,30%,40%,50%) with known diffusivity values at 0oC(10). All images were acquired on a 1.5T MRI scanner with an 8-channel cardiac coil (GE Healthcare, Chicago, IL). The phantom was filled with crushed ice and stored in a refrigerator overnight to establish steady-state temperature during apparent diffusion coefficient (ADC) measurement. The phantom was first securely positioned at iso-center. A total of 8 sequences were acquired (six coronal, two axial), including: coronal conventional DWI-EPI (3 diffusion directions, repeated with 1 and 3 averages (NEX)), coronal DTI-EPI (30 directions), coronal DWI-MAVRIC (repeated with 3, 2, and 1 bins), axial DWI-EPI (NEX=3) and axial MAVRIC-DWI (3 bins) using a b-value of 1000 s/mm2. The phantom was rotated 90o between the coronal and axial sequences to ensure the vial contents were in-plane for all scans. Scans commenced 5 minutes after repositioning to reduce residual flow effects. To evaluate effects of gradient nonlinearity and off-isocenter positioning, the 8 sequences were then repeated at two nominal spatial offsets of 10 cm left and right off iso-center. Left and right positions were assigned from the perspective of a supine patient entering the scanner headfirst. Images were processed with software (MATLAB, Mathworks, Natick, MA) to generate ADC Maps with and without gradient nonlinearity correction (GNC)(11). Circular region-of-interests of ~208 mm2 (coronal) and 102 mm2 (axial) were placed on the ADC maps using ITK-SNAP(12) on each vial for analysis.Results
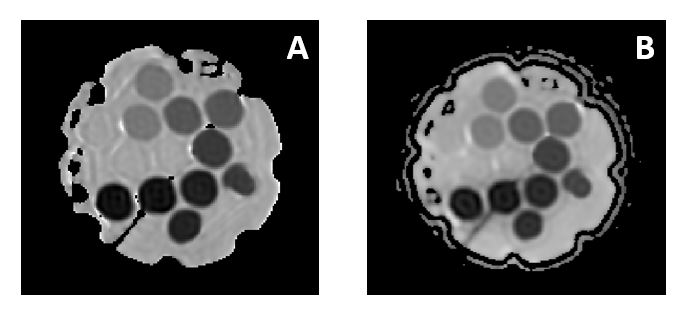
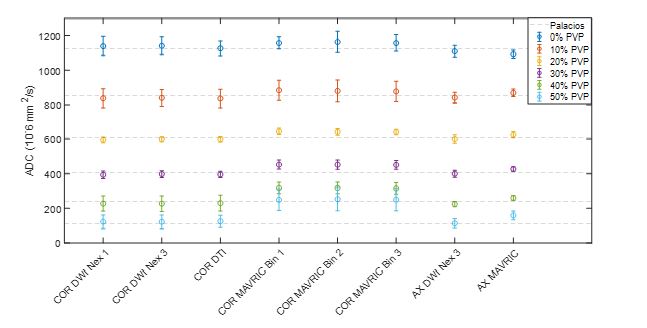
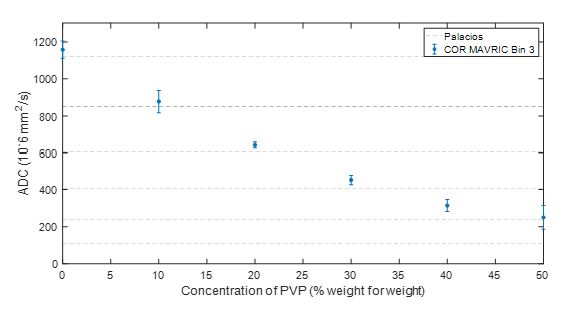
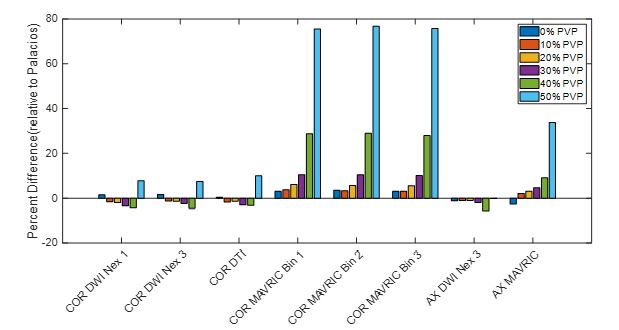
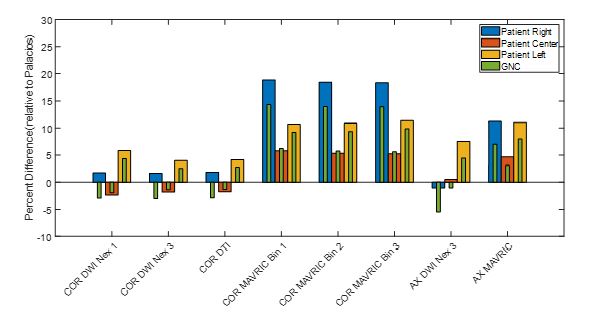
Fig. 1 compares ADC maps from DWI-EPI and DWI-MAVRIC, showing less geometric distortion in the MAVRIC maps. Fig. 2 compares the mean ADC at all PVP concentrations against the reference values(10). Excellent (negative) correlation between ADC and concentration was obtained with all EPI (r=-0.987 to -0.991) and MAVRIC scans (r=-0.978 to -0.992). However, we observed a pattern of bias at the high PVP vials (40-50%) with low diffusivities in the DWI-MAVRIC scans (Fig. 3). The bias was analyzed more closely in the error plot of Fig.4, which showed the lowest error in axial DWI-EPI, a small positive bias in the 50% vials with coronal DWI-EPI, a large positive bias in the 50% vials with axial DWI-MAVRIC, and large biases in both 40% and 50% vials in coronal DWI-MAVRIC. Fig. 5 shows the effects of positioning, whereby the lowest ADC errors were found at isocenter, as compared to the left and right positions. Gradient nonlinearity correction reduced the absolute error in all eight sequences by 0.31 %, 3.63%,0.65% for the center, left, and right positions respectively.Discussion
Validating diffusion MAVRIC as a clinical imaging tool requires evaluating the differences between measured ADC values and ground truth. The negative ADC bias associated with lower PVP is likely associated to noise and can be addressed using various denoising techniques. The positive ADC bias due to high PVP was attributed to suboptimal b-value, which can be mitigated by a multi b-value acquisition. Finally, the large positive bias identified in data from MAVRIC images remains a point of investigation but is suspected to be caused by a combination of residual CPMG violations and reconstruction algorithm vulnerabilities of the PROPELLER DUO approach.Acknowledgements
Research reported in this abstract was supported by NIH/NIAMS under award number R01AR064848. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.References
1. Bihan DL, Turner R, MacFall JR. Effects of intravoxel incoherent motions (IVIM) in steady-state free precession (SSFP) imaging: application to molecular diffusion imaging. Magnetic Resonance in Medicine 1989;10:324 337.
2. Raya JG, Melkus G, Adam-Neumair S, et al. Change of diffusion tensor imaging parameters in articular cartilage with progressive proteoglycan extraction. Invest Radiol 2011;46:401–9 doi: 10.1097/rli.0b013e3182145aa8.
3. Hooijmans MT, Damon BM, Froeling M, et al. Evaluation of skeletal muscle DTI in patients with duchenne muscular dystrophy. Nmr Biomed 2015;28:1589–1597 doi: 10.1002/nbm.3427.
4. Wengler K, Tank D, Fukuda T, et al. Diffusion tensor imaging of human Achilles tendon by stimulated echo readout‐segmented EPI (ste‐RS‐EPI). Magnet Reson Med 2018;80:2464–2474 doi: 10.1002/mrm.27220.
5. Farahani K, Sinha U, Sinha S, Chiu LC-L, Lufkin RB. Effect of field strength on susceptibility artifacts in magnetic resonance imaging. Comput Med Imag Grap 1990;14:409–413 doi: 10.1016/0895-6111(90)90040-i.
6. Koch KM, Lorbiecki JE, Hinks RS, King KF. A multispectral three‐dimensional acquisition technique for imaging near metal implants. Magnet Reson Med 2009;61:381–390 doi: 10.1002/mrm.21856.
7. Koch KM, Bhave S, Gaddipati A, et al. Multispectral diffusion‐weighted imaging near metal implants. Magnet Reson Med 2018;79:987–993 doi: 10.1002/mrm.26737.
8. Pipe JG, Farthing VG, Forbes KP. Multishot diffusion‐weighted FSE using PROPELLER MRI. Magnet Reson Med 2002;47:42–52 doi: 10.1002/mrm.10014.
9. Razek AA, Nada N. Role of diffusion-weighted MRI in differentiation of masticator space malignancy from infection. Dentomaxillofac Rad 2013;42:20120183 doi: 10.1259/dmfr.20120183.
10. Palacios EM, Martin AJ, Boss MA, et al. Toward Precision and Reproducibility of Diffusion Tensor Imaging: A Multicenter Diffusion Phantom and Traveling Volunteer Study. Am J Neuroradiol 2017;38:537 545 doi: 10.3174/ajnr.a5025.
11. Tan ET, Marinelli L, Slavens ZW, King KF, Hardy CJ. Improved correction for gradient nonlinearity effects in diffusion-weighted imaging. J Magn Reson Imaging 2012;38:448–53 doi: 10.1002/jmri.23942.
12. Yushkevich PA, Piven J, Hazlett HC, et al. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage 2006;31:1116–1128 doi: 10.1016/j.neuroimage.2006.01.015.
Figures