1337
IVIM Imaging of Lung Cancer: A Comparison Between Gradient-and Spin-Echo, Turbo Spin-Echo and Echo-Planar Imaging Techniques
Tianyu Zhang1, Yishi Wang2, Chengxiu Yuan1, Xiaoyu Wang1, Jia Zhao1, and Huaqiang Sheng1
1The First Affiliated Hospital of Shandong First Medical University, Jinan, China, 2Philips Healthcare, Beijing, China
1The First Affiliated Hospital of Shandong First Medical University, Jinan, China, 2Philips Healthcare, Beijing, China
Synopsis
The aim of the study was to compare intravoxel incoherent motion diffusion-weighted imaging (IVIM-DWI) for evaluating lung cancer using single-shot gradient- and spin-echo (SS-GRASE), single-shot turbo spin-echo (SS-TSE) and single-shot echo-planar imaging (SS-EPI) on a 3.0T MRI scanner. The signal-to-noise ratio (SNR), contrast signal-to-noise ratio (CNR), image distortion of lesions, ADC and IVIM parameters from the three sequences were compared. We found that GRASE-IVIM had the characteristics of short scan time and small distortion, relatively low SNR but high CNR. Our study showed that GRASE-IVIM has great potential for lung cancer.
Introduction
At present, most lung IVIM studies have been carried out using echo planar imaging (EPI) technique, which has fast imaging speed and high SNR, but due to the characteristics of lung tissue, image quality is frequently deteriorated by susceptibility artifacts. This could lead to lower accuracy of IVIM assessment1. Turbo spin-echo (TSE) technique has the advantage of negligible distortion but low scan efficiency2. GRASE sequence has shown high application value in cholangiopancreatography3, but its application in lung IVIM has not been reported. This study explored the application value of GRASE technique in lung cancer and compared it with the TSE and EPI technique.Materials and Methods
PatientsA total of 28 patients with lung cancer (17 males and 21 females; age range, 42–84 years; mean age, 62.6 years) were included with written informed consent obtained from each patient. This study was approved by the local IRB.
MRI Experiments
All the MRI examinations were performed on a 3.0T MR scanner (Ingenia CX; Philips Healthcare, Best, The Netherlands) equipped with a body phase array coil. The examination included routine MR scans and IVIM sequences: (1) Coronal single-shot fast spin echo breath-hold T2-weighted imaging (T2WI); (2) Axial fat-suppressed respiratory-triggered T2WI. In order to save the scan time, both IVIM and T2WI use 12 slices, with coronal T2WI as the positioning image to ensure that the largest layer of the lesion was in the center of the IVIM scan. Table 1 shows the detailed scan parameters of the IVIM sequences.
Data analysis
The quantitative assessments of the image quality of all 28 patients were analyzed by 2 radiologists with 3 and 6 years of experience for MR diagnosis, respectively. Image distortions of the lesions in each sequence were quantitatively compared using the maximum displacement in the phase-encoding direction of the lesion between T2WI/SPIR and IVIM by superimposing IVIM on T2WI(with b = 800 s/mm2 ), signal-to-noise ratio(SNR), and contrast-to-noise ratio (CNR) from TSE-IVIM ,EPI-IVIM and GRASE-IVIM (with b = 800 s/mm2 ) were measured. 3 circular regions of interest (ROIs, ≥70 pixels per ROI) were delineated by 2 experienced readers independently and placed in lesions, erector spinae muscle, and the lung for the measurement of the SNR and CNR.One ROI in the lung was put right next to the lesion to assess local noise. Mean signal intensity (SI) and the standard deviation (SD) were measured for each ROI and the results from the two readers were averaged. SNR and CNR were calculated using Eq. (1–2)2:
(1) $$$\mathrm{SNR}=\mathrm{SI}_{\text {lesion }} / \mathrm{SD}_{\text {lung }} $$$
(2) $$$\mathrm{CNR}=\left(\mathrm{SI}_\text {lesion }-\mathrm{SI}_{\text {muscle }}\right) / \sqrt{{\mathrm{SD}_{\text {lesion }}}^{2}+{\mathrm{SD}_{\text {muscle}}}^{2}}$$$
Where SIlesion and SImuscle are the mean SI in the lesion and muscle; SDlesion, SDlung, and SDmuscle are the standard deviations of the SI in the lesion, lung, and muscle, respectively.
ADC maps were generated automatically inline by the scanner. IVIM paraments were processed offline with an open source medical imaging interaction toolkit (MITK Diffusion, v. 2018; DKFZ, Heidelberg, Germany).
Statistical analyses were conducted using SPSS (Version 26; IBM Corporation) and MedCalc software (Version 19; Mariakerke, Belgium). ADC value, IVIM parameters, SNR and CNR from TSE-IVIM, GRASE-IVIM and EPI-IVIM were compared using ANOVA, and the distortion level were compared between each pair of sequences with Wilcoxon test (P value < 0.05 was considered to be statistically significant for all the analyses).
Results
The imaging efficiency of GRASE-IVIM and TSE-IVIM was 100%, and the imaging efficiency of EPI-IVIM was 89% (3 cases of lesions could not be analyzed on EPI-IVIM because of severe geometric deformation). In terms of SNR, EPI-IVIM>TSE-IVIM>GRASE-IVIM, pairwise comparisons showed significant differences (P<0.05)(Figure 2); CNR was significantly lower for EPI-IVIM compared with GRASE-IVIM and TST-IVIM (P<0.001), whereas the CNR of GRASE-IVIM was higher than that of TSE-IVIM, but the difference was not significant (P>0.05)(Figure 2).The image distortions of lesions in GRASE-IVIM and TSE-IVIM were significantly lower than that of EPI-IVIM (P<0.001)(Figure 2) . In terms of IVIM and ADC parameters, the ADC and D value of TSE-IVIM were higher than those of EPI-IVIM and GRASE-IVIM (P<0.001), The f value of TSE-IVIM were higher than those of EPI-IVIM in the lesions(P<0.05)(table 2).Discussion
The SS-GRASE technique can be viewed as a hybrid of TSE and EPI4. Our data showed that GRASE-IVIM could reduce the lesion deformation artifacts (Figure 1) and had a higher CNR, while the SNR was lower than EPI-IVIM and TSE-IVIM. ADC, D and f values of IVIM from the three techniques showed statistically significant differences, thus ADC and IVIM parameters from different techniques should be interpreted with great caution.Conclusion
Our results showed that GRASE technology is a useful technique for IVIM imaging of pulmonary space-occupying lesions. It has fast imaging speed and small lesion distortions. The IVIM parameters using different techniques should be interpreted with caution.Acknowledgements
We thank Yishi Wang from Philips Healthcare for this valuable support on the IVIM sequence.References
1. Ohno Y, Koyama H, Yoshikawa T, et al. Diffusion-weighted MR imaging using FASE sequence for 3T MR system: Preliminary comparison of capability for N-stage assessment by means of diffusion-weighted MR imaging using EPI sequence, STIR FASE imaging and FDG PET/CT for non-small cell lung cancer patients. Eur J Radiol. 2015;84(11):2321-2331.
2. Wan Q, Lei Q, Wang P, et al. Intravoxel Incoherent Motion Diffusion-Weighted Imaging of Lung Cancer: Comparison Between Turbo Spin-Echo and Echo-Planar Imaging. J Comput Assist Tomogr. 2020;44(3):334-340.
3. Yoshida M, Nakaura T, Inoue T, et al. Magnetic resonance cholangiopancreatography with GRASE sequence at 3.0T: does it improve image quality and acquisition time as compared with 3D TSE?. Eur Radiol. 2018;28(6):2436-2443.
4. Chu ML, Chien CP, Wu WC , et al. Gradient- and spin-echo (GRASE) MR imaging: a long-existing technology that may find wide applications in modern era. Quant Imaging Med Surg. 2019;9(9):1477-1484.
Figures
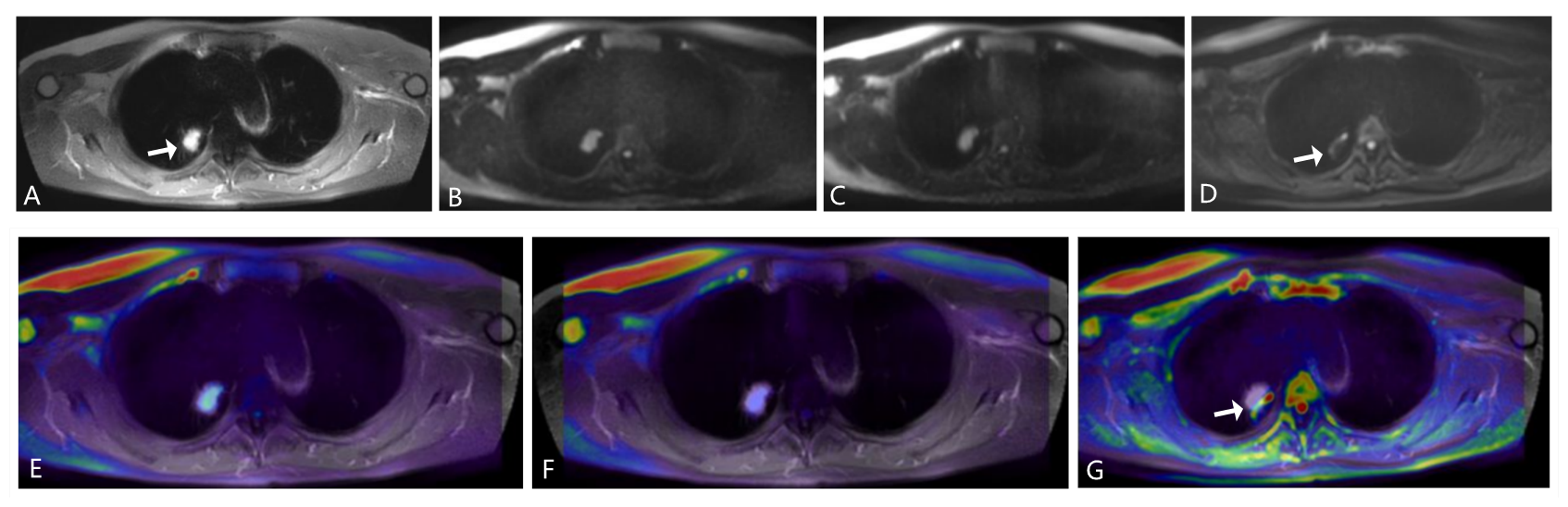
FIGURE 1. A nodular lesion (arrow) in the right upper lobe. A, T2WI-SPIR. B, GRASE-IVIM (b = 800 s/mm2 ). C, TSE-IVIM (b = 800 s/mm2 ). D, EPI-IVIM (b = 800 s/mm2 ).E,T2WI fused with GRASE-IVIM. F, T2WI fused with TSE-IVIM.G, T2WI fused with EPI-IVIM. The distortion and displacement of the lesion are shown on EPI-IVIM (arrow). On TSE and GRASE-IVIM ,the lesion, along with its air bronchus, can be clearly shown. Fused images showed that GRASE and TSE-IVIM is perfectly matched with T2WI-SPIR.
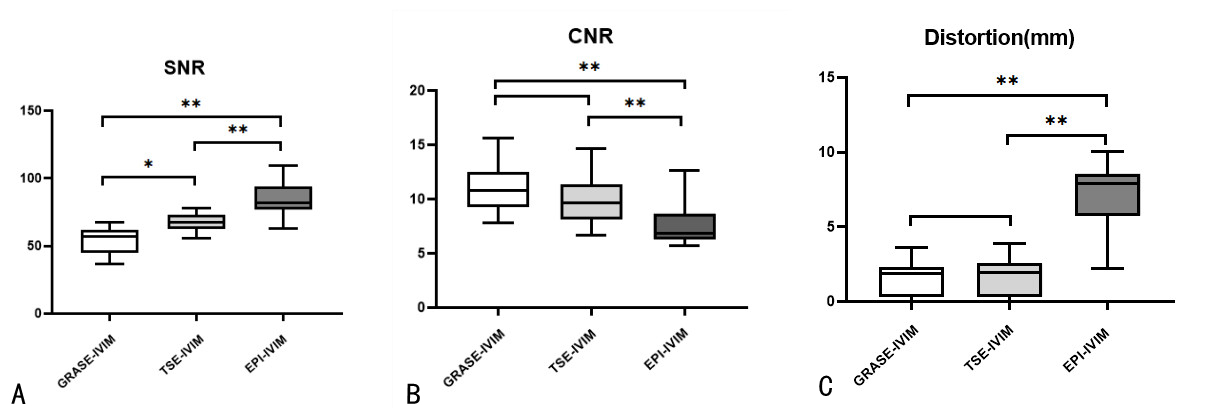
FIGURE 2. Comparison of SNR,CNR and Distortion between GRASE-IVIM,TSE-IVIM and EPI-IVIM.
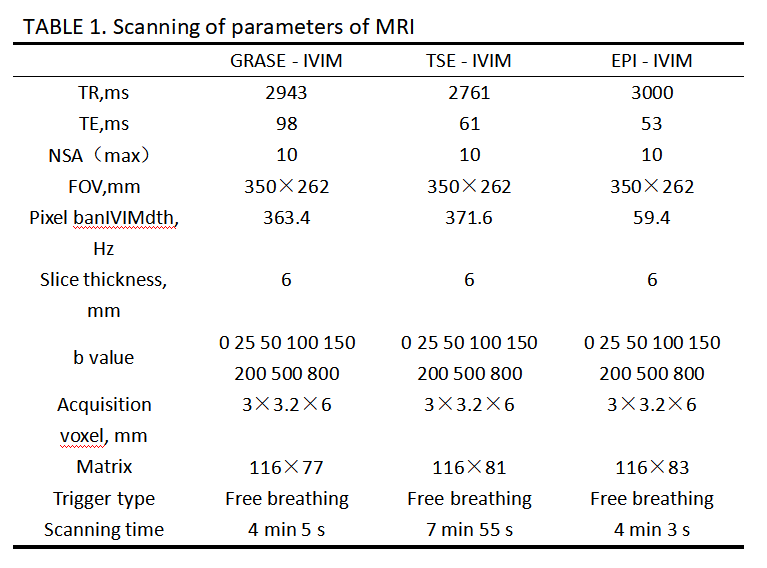
TABLE 1 Scanning of paraments of MRI
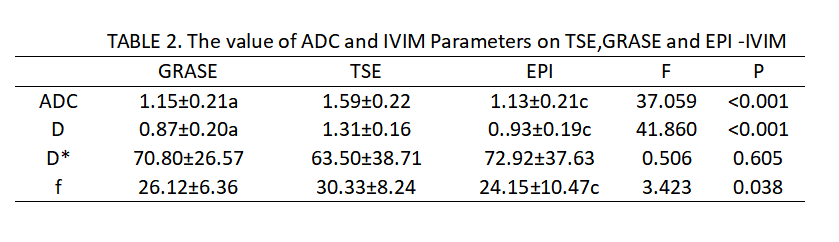
TABLE 2 The value of ADC and IVIM Parameters on TSE,GRASE and EPI-IVIM