1298
Inter-rater reliability of sciatic nerve evaluation with MR neurography: a comparison study of multiple sequences1Department of Radiology, Chiba University Hospital, Chiba, Japan, 2Diagnostic Radiology and Radiation Oncology, Graduate School of Medicine, Chiba University, Chiba, Japan, 3Philips Japan, Tokyo, Japan
Synopsis
MR neurography (MRN) is a useful technique to evaluate damaged peripheral nerves showing increased signal intensity and enlarged nerve diameter. Although various MRN sequences have been developed, the inter-rater reliability of MRN have rarely been evaluated. Therefore, the purpose of this study was to evaluate inter-rater reliability of sciatic nerve evaluation with MRN sequences: T2WI, 3D-STIR, T2-FFE, 3D-iNerveVIEW, Diffusion-neurography, DTI, and pcDSDE. Measured diameters varied among the sequences. 3D-iNerveVIEW showed a high inter-rater reliability for signal measurements. In MRN, it is important to understand the characteristics of each sequence.
INTRODUCTION
Damaged nerves show increased the signal intensity and enlarged nerve diameter.1,2 In general, T2WI-based MR neurography (MRN) has high resolution, while DWI-based excellent has high contrast. Various sequences have been developed, and new imaging methods include 3D-iNerveVIEW and pcDSDE (phase-cycling-diffusion-sensitized driven-equilibrium). 3D-iNerveVIEW is a T2WI-based sequence, which is expected to improve the visibility of peripheral nerves by suppressing the visualization of vessels and muscles.3 pcDSDE can reduce signals of the neighboring structures, including the vessels, and visualize the nerves with diffusion contrast.4 There are few studies that compare MRN sequences and examine inter-rater reliability. The peripheral nerve is thin and has anatomical variation, so the inter-rater reliability of quantitative measurements can be unstable. The purpose of this study was to evaluate the inter-rater reliability of sciatic nerve size and the signal value among seven MRN sequences: T2WI, 3D-short-TI-inversion-recovery (3D-STIR), T2-fast-field-echo (T2-FFE), 3D-iNerveVIEW, diffusion-neurography (DN), diffusion-tensor-image (DTI), and pcDSDE.METHODS
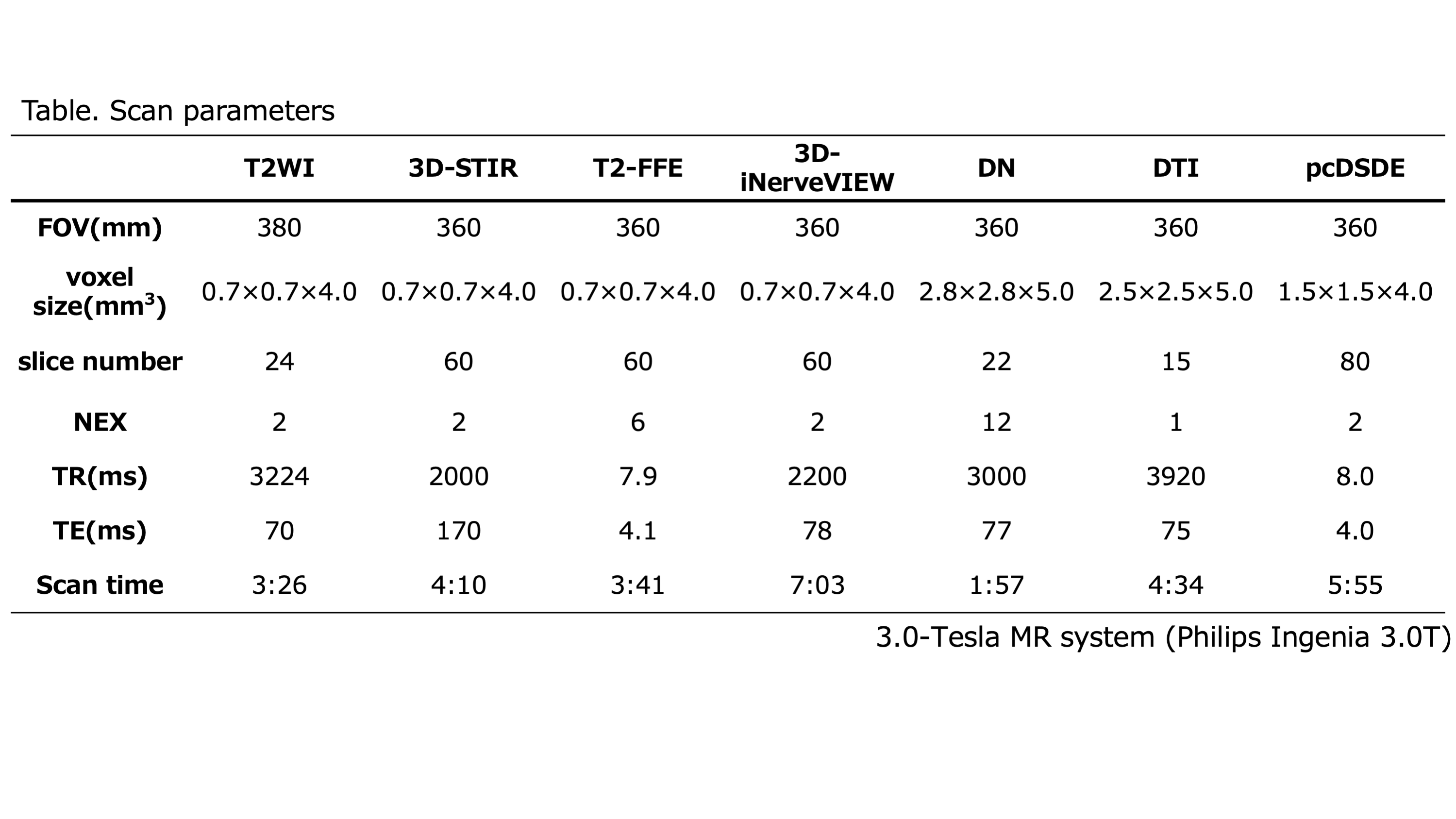
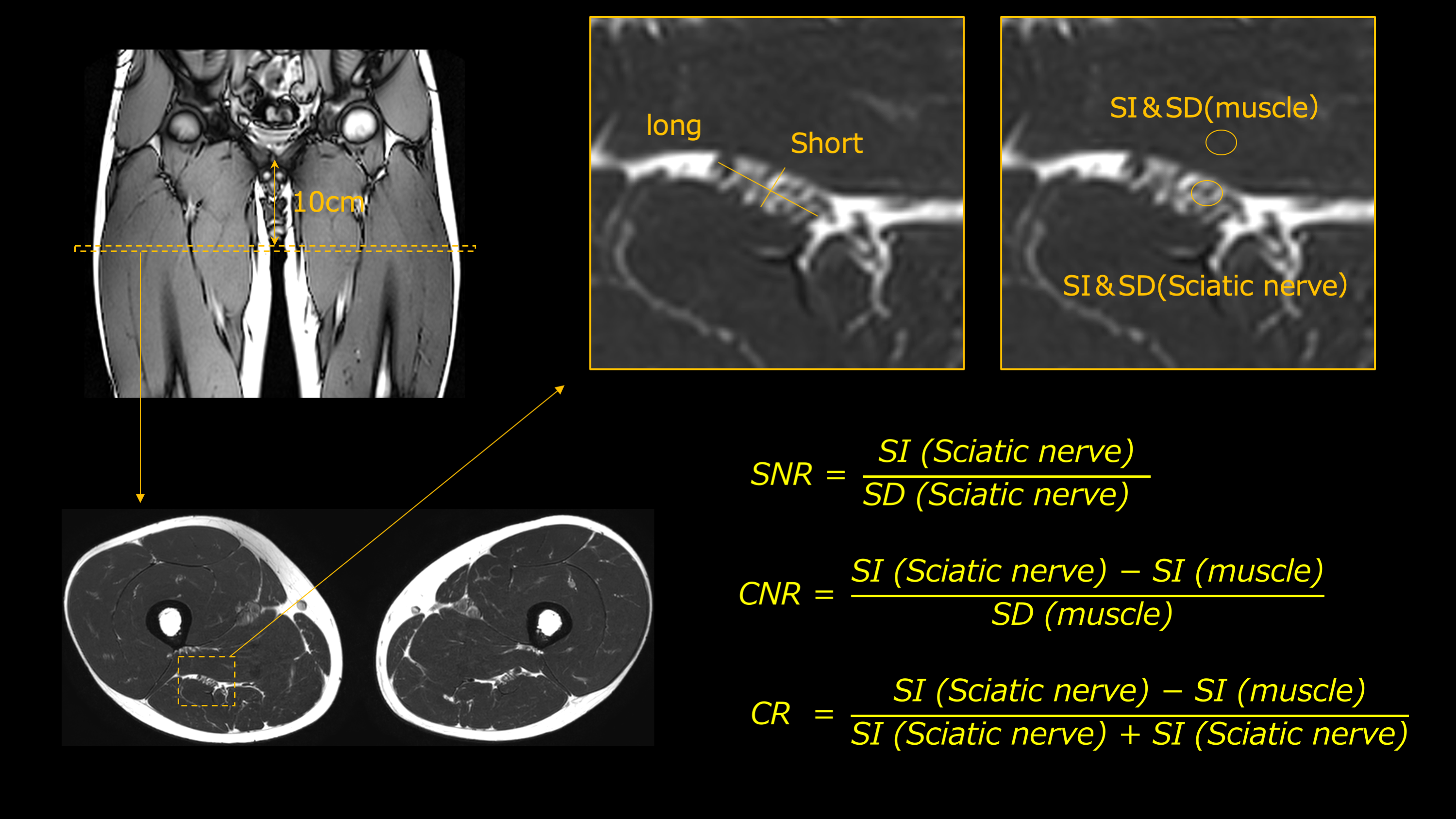
This study included 20 healthy volunteers (median age 32, age-range 23-60, 18 men and 2 women). MRNs were acquired in the proximal part of the femur using a trousseau coil. The scanning parameters are summarized in Figure 1. Two Radiologists measured the long and short diameters of bilateral sciatic nerves at the level 10 cm below the pubic symphysis and set regions of interest (ROIs) on the nerve and adductor muscle (Figure 2). The signal-to-noise ratio (SNR), contrast-to-noise ratio (CNR), and contrast ratio (CR) were calculated from the signals of the sciatic nerve and adductor muscle as shown in Figure 2. The sciatic nerve diameters of each MRN sequence were compared using the Wilcoxon tests; the P-value was corrected by the Bonferroni method. Inter-rater reliability of sciatic nerve size and the signal value were assessed using intraclass coefficient correlations (ICC), which was interpreted as follow: 0.000–0.200, slight; 0.201–0.400, fair; 0.401–0.600, moderate; 0.601–0.800, substantial; 0.801–1.00, almost perfect agreement.RESULTS
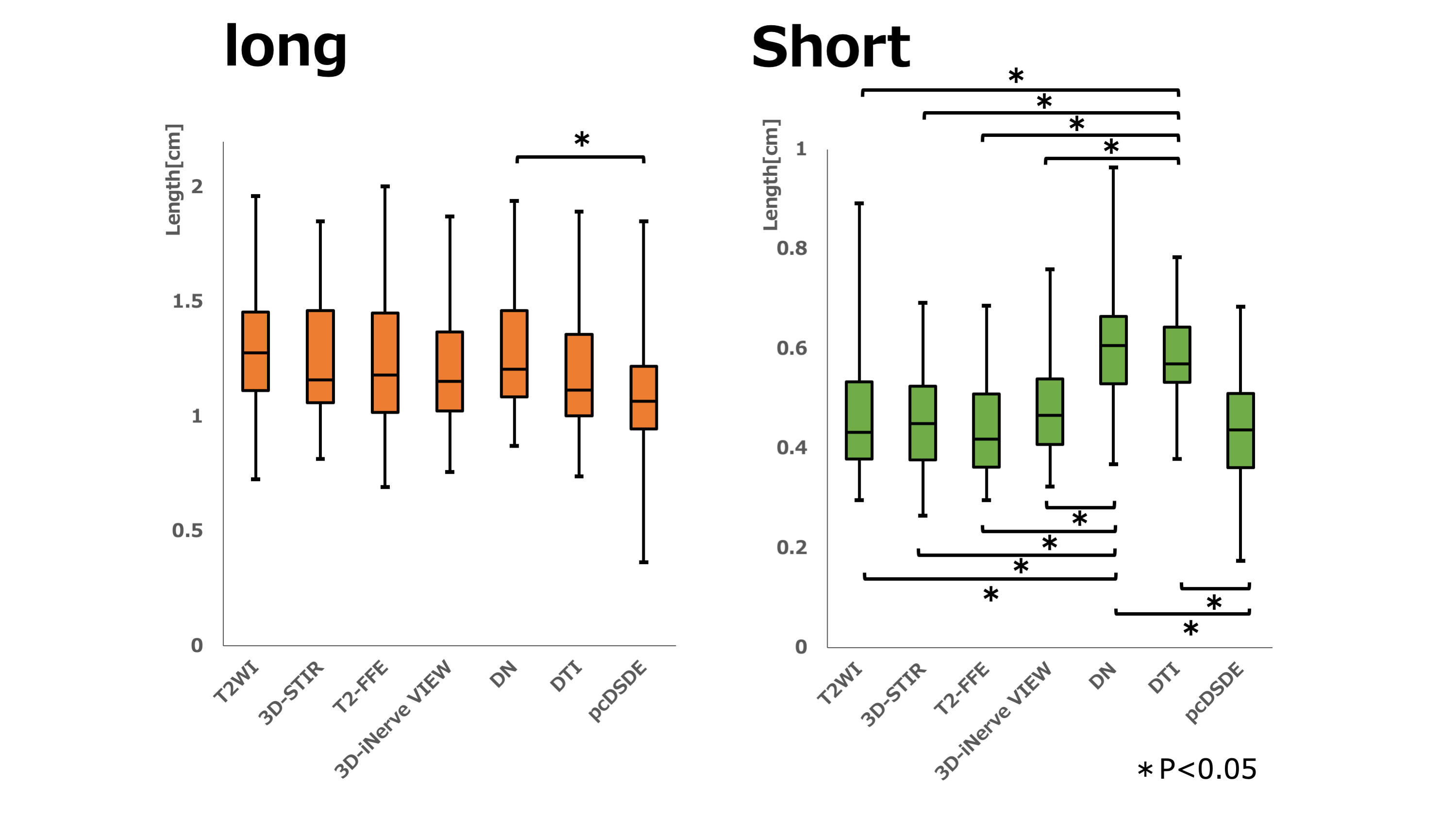
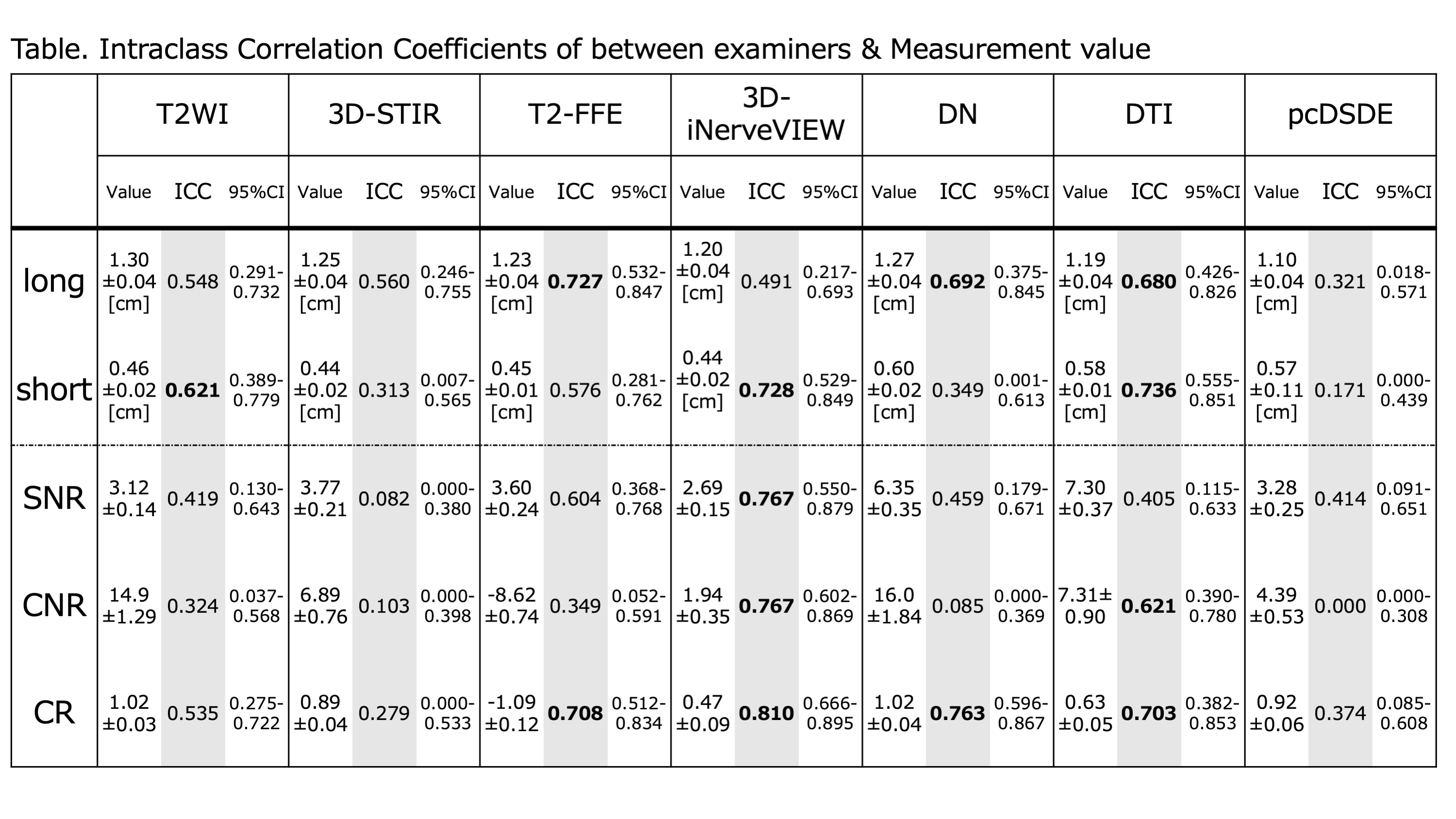
Measured diameters are shown in Figure 3. The long diameter was significantly different between pcDSDE and DN. The short diameter was significantly different between the T2WI-based sequences vs. DN and DTI. Inter-rater reliability of sciatic nerve diameter and the signal value was shown in Figure 4. T2-FFE shows substantial agreement on long diameter (0.727). Short diameter, SNR, CNR, and CR of 3D-iNerveVIEW shows substantial to almost perfect agreement (0.728–0.810). DN and DTI show substantial agreement on long diameter and CR (0.680–0.763). pcDSDE has slight to moderate reliability for all items (0.171–0.414).DISCUSSION
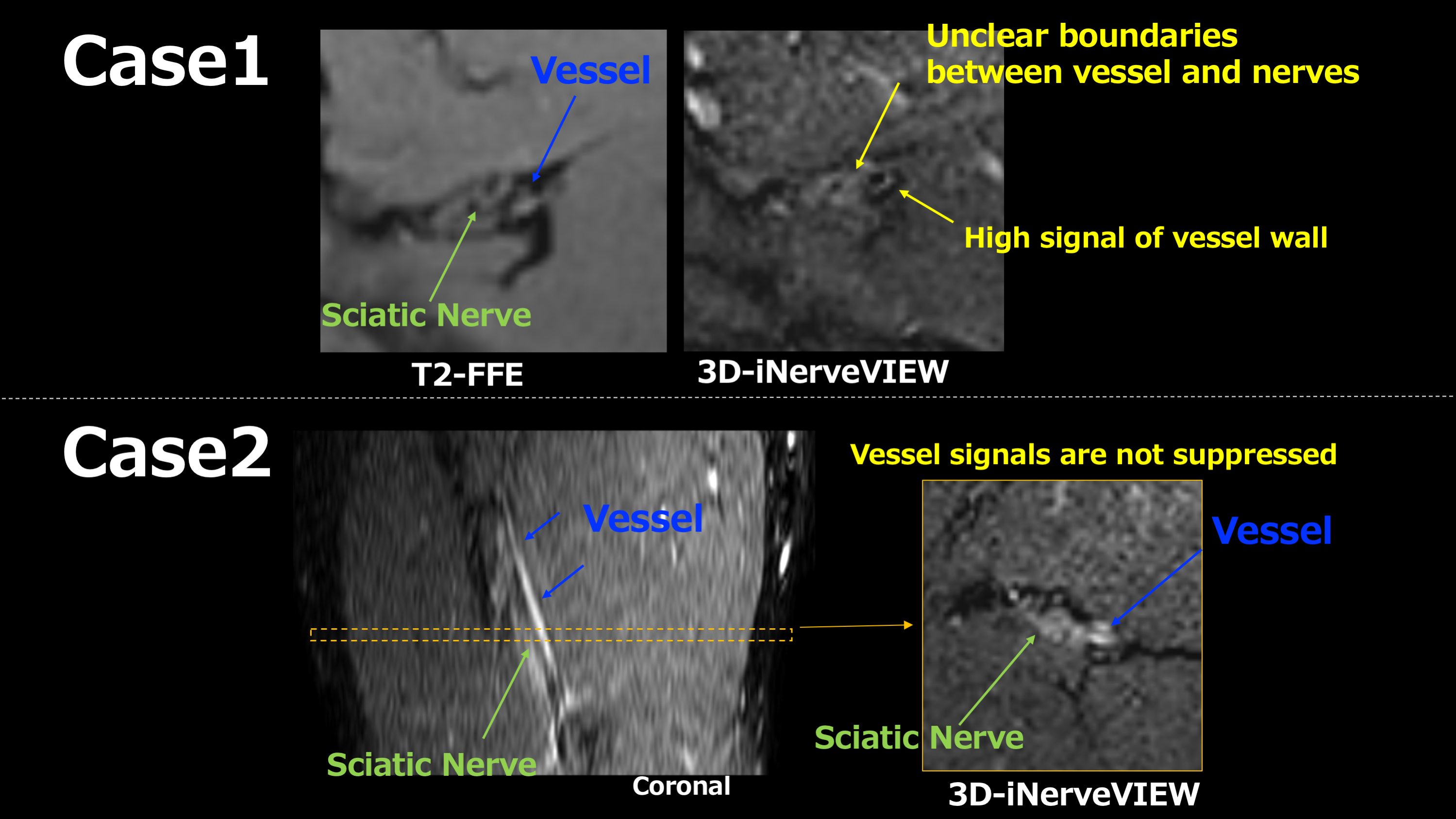
Each MRN sequence has both advantages and disadvantages for quantitative measurements. T2-FFE was relatively reliable in the long diameter measurement, while 3D-iNerveVIEW was reliable on the short diameter and signal measurement. Regarding inter-rater reliability of the long diameter, T2-FFE was superior to the other sequences. T2-FFE was easy to detect the nerve because the contrast between the fat, vessels, and muscles inside and around the nerve was clear. However, the inter-rater reliability of T2-FFE in short diameter was lower than 3D-iNerveVIEW. Because the signals of the nerve and muscle are comparable, so the boundary is unclear when a nerve and a muscle are in close proximity.The long diameter of 3D-iNerveVIEW was moderately reliable. The vessels with incomplete signal suppression were misidentified as the nerve and might be included in measurements when the vessels running parallel to the sciatic nerve (Figure 5). In short diameter, the measurement was easy because the vessels parallel to the nerve do not run in the anterior and posterior side of the nerve, and the signal contrast between the nerve and neighbors is clear on 3D-iNerveVIEW.Since DWI-based sequences suppress background tissues including the vessels and show nerves as high signals5,6, the contrast of the nerves is clear. Therefore, DN and DTI showed substantial reliability in long diameter. However, DWI-based sequences have a relatively low spatial resolution and tend to look thicker than the real due to the influence of image distortion7,8, so that the measured diameters might not be feasible. Regarding inter-rater reliability of sciatic nerve signal, 3D-iNerveVIEW shows relatively high reliability. That might be because the nerves are visualized with a high signal on 3D-iNerveVIEW, and the signal values of nerves and muscles are visualized relatively uniformly. In T2WI and 3D-STIR, since the signal of the peripheral nerves and the vessels were similar and they could not be visually separated9,10, inter-rater reliability of sciatic nerve size and the signal value might be poor. pcDSDE showed a large amount of image distortion, resulting in a low degree of reliability in all items, suggesting that pcDSDE may not be suitable for imaging the sciatic nerve.CONCLUSION
MRN should be selected by understanding the characteristics and reliability of each sequence because peripheral nerve measurements among sequences were not always reliable. Although the 3D-iNerveVIEW appeared to have a relatively high inter-rater reliability, separating the nerves from the vessels is challenging yet. Care must be taken when measuring the nerve diameter.Acknowledgements
No acknowledgement found.References
1. Bäumer P, Dombert T, Staub F, et al. Ulnar neuropathy at the elbow: MR neurography-neurography-nerve T2 signal increase and caliber.Radiology 260:199-206:199-206,2011
2. Guggenberger R, Markovic D, Eppenberger P, et al. Assesment of median nerve with MR neurography by using diffusion-tensor imaging: normative and pathologic diffusion values.Radiology 265:194-203,2012
3. Yoneyama M, TAHARA T.Thomas C.Kwee, et al. Rapid High Resolution MR Neurography with a Diffusion-weighted pre-pulse, Magn Reson. Med. Sci. 2013;12(2):111-9.
4. Yoneyama M, Obara M, Ozawa Y, et al. High-Resolution 3D MR Neurography of the Wrist using Phase-Cycling Diffusion-Sensitized Driven-Equilibrium (pcDSDE). Proceeding in ISMRM2015.
5. Takahara T, Hendrikse J, Kwee TC, et al. Diffusion-weighted MR neurography of the sacral plexus with unidirectional motion probing gradients. Eur Radiol 2009;20: 1221-1226
6.Takahara T, Hendrikse J, Yamashita T, et al. Diffusion-weighted MR neurography of the brachial plexus: feasibility study. Radiology 2008; 249:653-660.
7. Eppenberger P, Andreisek G, Chhabra A, et al. Magnetic resonance neurography: diffusion tensor imaging and future directions. Neuroimaging Clin N Am 24:245–256
8. Zhao L, Wang G, Yang L, et al. Diffusion-weighted MR neurography of extremity nerves with unidirectional motion-probing gradients at 3 T: feasibility study. AJR Am J Roentgenol 200:1106–1114
9. Maravilla KR, bowen BC, et al. Imaging of the peripheral nervous system: evaluation of peripheral neuropathy and plexopathy. AJNR Am J Neuroradiol 1998;19:1011-1023.
10. Viallon M, Vargas MI, Jlassi H, et al. High-resolution and functional magnetic resonance imaging of the brachial plexus using an isotropic 3D T2 STIR (Short Term Inversion Recovery) SPACE sequence and diffusion tensor imaging. Eur Radiol 2008; 18:1018-1023.
Figures