1177
Time Domain Principal Component Analysis for Rapid, Real-Time MRI Reconstruction from Undersampled Data1Oncology, University of Alberta, Edmonton, AB, Canada, 2Medical Physics, Cross Cancer Institute, Edmonton, AB, Canada
Synopsis
A real-time acceleration method using Principal Component Analysis (PCA) was developed for use on hybrid MR-radiotherapy machines. Using principal components representative of the temporal changes of k-space in combination with incoherently undersampled data from past dynamic frames, the missing data from the current undersampled frame can be filled in. This allows for real-time fully-reconstructed images. Retrospective analysis on 15 fully-sampled lung cancer patients was used to test the method. Using metrics such as NMSE, pSNR and SSIM, image quality and temporal-robustness was assessed. Dice coefficient, centroid displacement and Hausdorff distance were used to test auto-contouring capabilities for target tracking effectiveness.
Introduction
The integration of real-time MR imaging with radiotherapy can allow for rapid adjustments to changing patient anatomy due to intrinsic motion such as respiration, organ motion, and unintentional patient motion. Several groups have developed hybrid MRI-radiotherapy machines in order to achieve this adaptive radiotherapy in real-time.1-3 Our group has developed a method of real-time imaging using Principal Component Analysis (PCA) in the time domain. The method involves a shifting window (consisting of the current frame and Nwin-1 previous dynamic frames) used to reconstruct the current real-time frame. The principal components (PCs) are calculated from a core set of phase encodes in central k-space and are frequently updated with the shifting window in order to best represent the current state of the anatomy. Previous work done within our group has looked into the use of PCA in the spatial domain for real-time imaging.4 In this work, the PCs were calculated from a database of 30 fully sampled images followed by undersampling of k-space during a simulated treatment. However, it was found that image quality degraded over time as the database become outdated. Our goal with this new method is to create a temporally robust acceleration method that is simple to implement.Methods
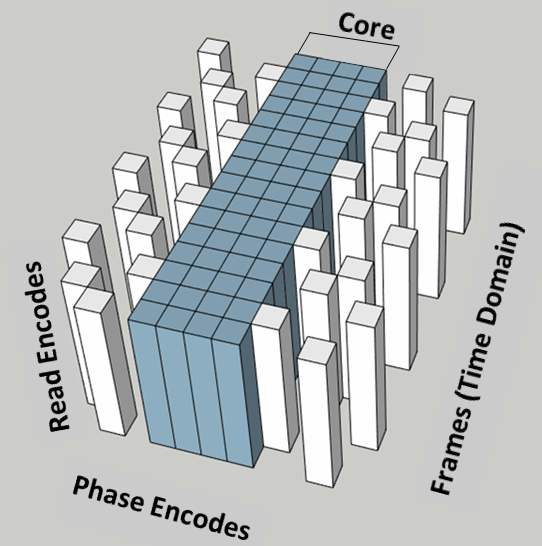
Fig.1 provides a visual representation of the process our method employs to acquire data and reconstruct a frame. A set of core data is used to calculate and continuously update the PCs used in reconstruction. This core k-space data refers to the central k-space (low-frequency) data that is acquired every frame (and never undersampled). The higher-frequency data is undersampled using a pseudo-random distribution of phase encodes in each frame. Fig.2 represents how k-space is sampled within the reconstruction window. The frames cycle through a pre-determined number of different complementary random distributions to ensure every phase encode is sampled once over a pre-determined number of frames. After each undersampled frame is acquired, the core data from the most-recent 60 frames is used to create a series of PCs that represent the time-dependent modulation of k-space. The most relevant PCs are then projected onto the sparsely-populated high-frequency data, using a pseudo-inverse function, to fill in unsampled phase encodes for the most-recent frame by extrapolation. The maximum number of PCs that can be used for fitting is dependent on the number of undersampled data points acquired within the reconstruction window. Testing was done retrospectively on 15 previously acquired fully sampled patient data sets using commercially available software (MATLAB R2019a, The MathWorks Inc., Natick MA, USA). The effects of acceleration were also tested. Acceleration rate is controlled by the number of complimentary patterns and the size of the core data. For our tests accelerations of 3,4,5,6 and 8 were tested. A subset of 6 of these patients was further used to test the auto-contouring capabilities of the reconstructed images from our method using auto-contouring software developed by our group.5Results
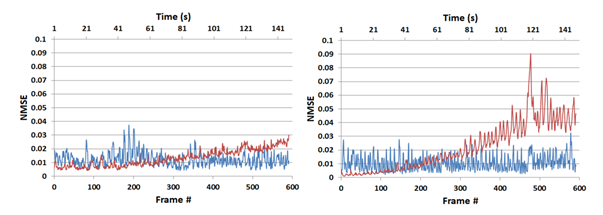
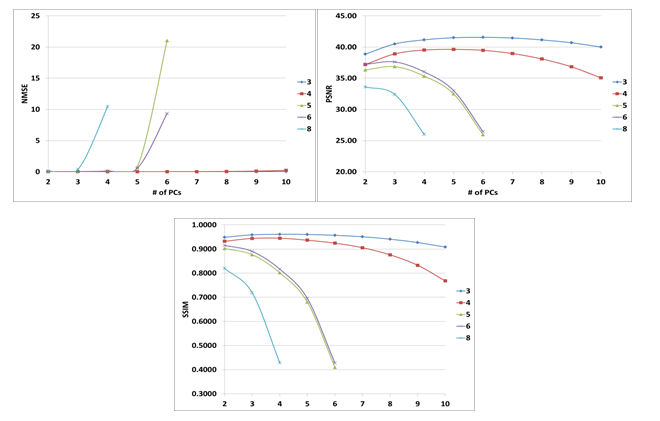
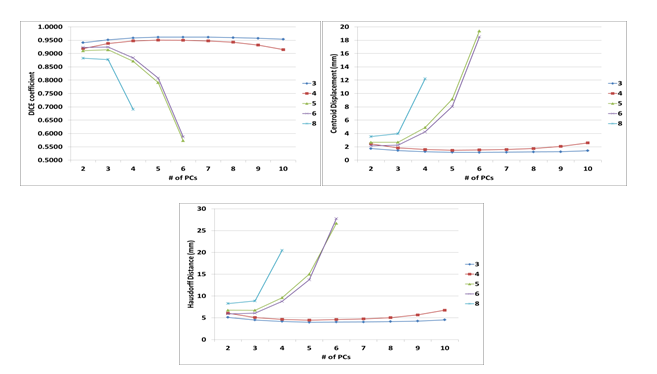
By assessing artifact level, using retrospectively undersampled lung images, the new reconstruction method results in images that better maintain their fidelity over time (2-4x smaller mean artifact level after 2 minutes) as shown in Fig.3, an improvement over the previous spatial method. The effect of acceleration and the number of PCs used for fitting (Npc) on image quality was also assessed. Fig.4 represents the changes in normalised mean square error (NMSE), peak-SNR (pSNR) and structural similarity SSIM with varying acceleration and Npc. The auto-contouring capabilities of the images reconstructed were measured using auto-contouring software developed within our group as well as with metrics such as the Dice coefficient, Hausdorff distance and centroid displacement.5 Fig.5 demonstrates the effects of acceleration and number of PCs kept for reconstruction on the auto contouring capabilities of our method.Discussion
Our method appears to remain robust over time. As Npc increases however, large noise spikes occasionally occur. This causes issues with image quality and auto contouring. This can be avoided by keeping Npc small. Further investigation is needed in order to determine the cause of these spikes and how to deal with them. This could allow for larger Npc which would increase motion detail. Fig.3 demonstrates that the spatial PCA method appears to work better initially however over time our time-domain method appears to be more robust. Optimization occurred on parameters such as Npc for reconstruction. This was done at various acceleration rates and was tested using image quality metrics and auto-contouring. As seen in Figs.4-5 the optimal number of PCs to be kept varies with acceleration. At lower acceleration values of 3 and 4 the optimal number of PCs appears to be 5. This number decreases with increasing acceleration likely due to the limit on Npc.Conclusion
This method of MRI reconstruction appears to be robust over time, but further investigation will be needed to assess the cause of intermittent artifact spikes. It is a method that requires little in terms of coil hardware or processing power to implement. Using optimal parameters can allow for real-time imaging at acceleration factors as high as 8x. Typical reconstruction times are ~50ms per frame (Intel® Core i5-2430M CPU @ 2.40GHz, 6GB RAM).Acknowledgements
The authors would like to acknowledge the financial contributions of the University of Alberta through the Antoine Noujam Graduate Entrance ScholarshipReferences
1. B. Fallone, B. Murray, S. Rathee, T. Stanescu, S. Steciw, S. Vidakovic, E. Blosser and D. Tymofichuk, "First MR images obtained during megavoltage photon irradiation from a prototype integrated linac-MR system," Med Phys, vol. 36, no. 6, pp. 2084-2088, June 2009.
2. D. Winkel, G. H. Bol, P. S. Kroon, B. van Asselen, S. S. Hackett, A. M. Werensteijn-Honingh, S. Mook, G. J. Meijer, J. Hes, M. Willemsen-Bosman, E. N. de Groot-van Breugel, I. M. Jürgenliemk-Schulz and B. W. Raaymakers, "Adaptive radiotherapy: The Elekta Unity MR-linac concept," Clinical and Translational Radiation Oncology, vol. 18, pp. 54-59, 2009.
3. P. J. Keall, M. Barton and S. Crozier, "The Australian magnetic resonance imaging-linac program," Radiother Oncol, vol. 18, pp. 203-206, 2014.
4. B. Dietz, E. Yip, J. Yun, B. G. Fallone and K. Wachowicz, "Real-time dynamic MR image reconstruction using compressed sensing and principal component analysis (CS-PCA): Demonstration in lung tumour tracking," Med Phys, vol. 44, no. 8, pp. 3978-3989, 2017.
5. J. Yun, E. Yip, Z. Gabos, K. Wachowicz, S. Rathee and B. G. Fallone, "Neural-network based autocontouring algorithm for intrafractional lung-tumor tracking using Linac-MR," Med Phys, vol. 42, no. 5, pp. 2296-2310, 2015.
Figures