1173
Simplified Phase-Sensitive Inversion Recovery (PSIR) Reconstruction using Multi-dimensional Integration (MDI) for Elevated SNR1UIH America, Inc., Houston, TX, United States, 2United Imaging Healthcare, Shanghai, China
Synopsis
We applied MDI algorithm to classic PSIR reconstruction for cardiac imaging and demonstrated the feasibility and effectiveness of the approach for improved SNR in phase-sensitive contrast imaging. In comparison to the conventional reconstruction, the algorithm offers a simplified and fast pathway to achieve desired image contrast. Improved SNR in the T1W images in comparison to the conventional PSIR reconstruction was obtained.
Introduction
Phase-Sensitive Inversion Recovery (PSIR) reconstruction1,2 has been widely employed in T1-weighted (T1W) Inversion Recovery (IR) imaging where the preceding IR pulse gives rise to T1 contrast of tissues. As opposed to magnitude-reconstruction, PSIR reconstruction algorithm enables more pronounced T1 contrast as it takes into account the sign of the recovering longitudinal magnetization. In conventional PSIR reconstruction, the phase of reference images (acquired at long inversion time) is removed from T1W IR images, prior to which the complex images for coil channels need to be combined in a weighted sum to improve image SNR and accuracy of estimated background phase. The complex weights are computed via an estimate of relative coil sensitivities using the acquired reference images; and are consequently applied to both T1W IR and reference images, by which phase error in the sensitivity maps is canceled. This computation is performed in sophisticated steps such that the entire computation is rather costly. In addition, the complex combination over coil channels may be undesirable for optimal SNR. Here, we propose employing the convenient yet comprehensive Multi-dimensional Integration (MDI) algorithm3 to overcome the issues. Applying the MDI concept, the background phase of the reference images is individually removed from the T1W IR images on a channel-to-channel basis rather than a complex combination of all. This MDI PSIR reconstruction method is demonstrated herein with a patient dataset in examination of myocardial infarction. Within shorter reconstruction time, improved image SNR in comparison to the conventional reconstruction is achieved.Methods
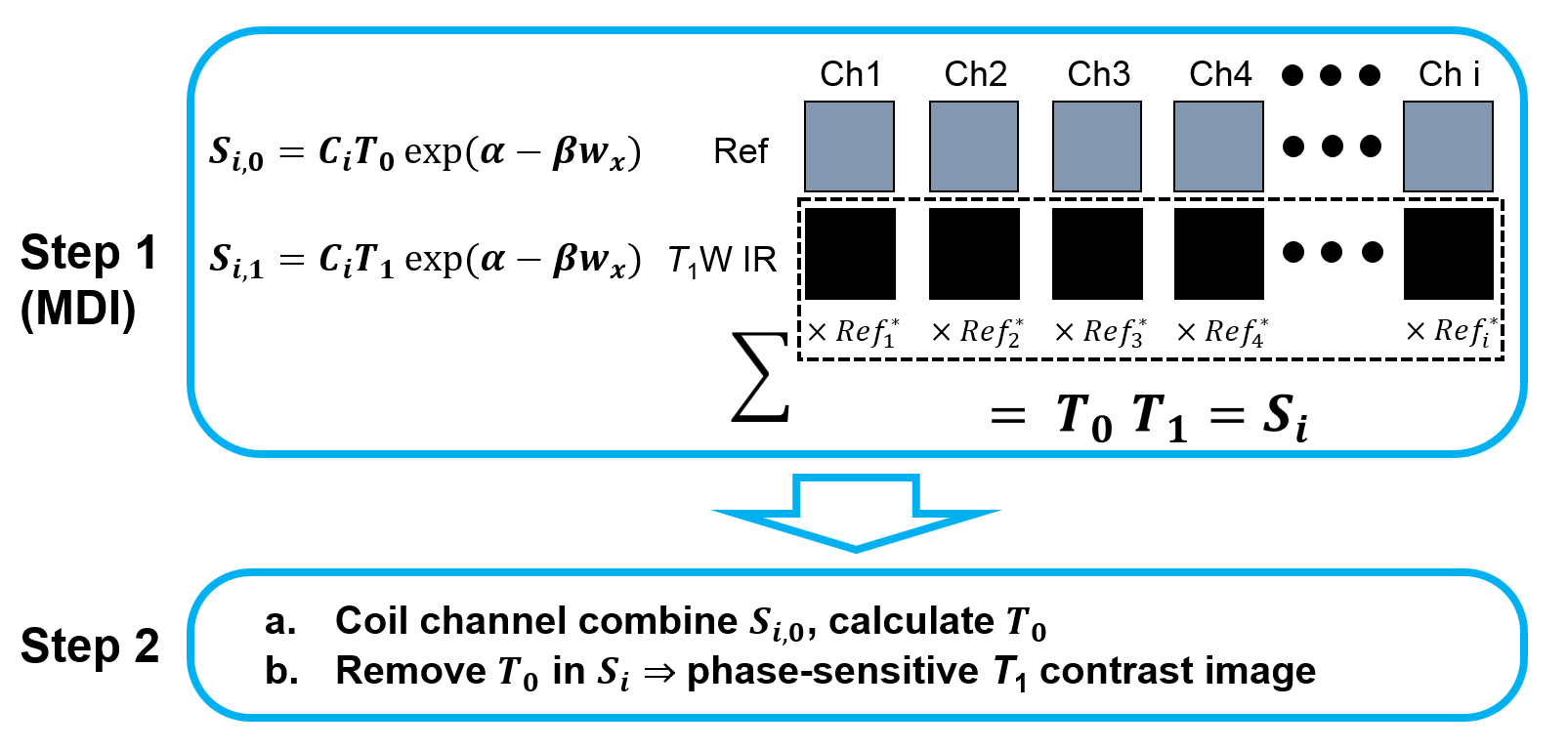
The echo signal during T1 inversion recovery can be expressed as $$\widetilde{f_{1}}(\omega_{x},\omega_{y}) = {f_{1}}(\omega_{x},\omega_{y})\exp\left\{i(\alpha-\beta\omega_x)\right\},$$ where the term $$$\exp\left\{i(\alpha-\beta\omega_x)\right\}$$$ signifies the background phase, in which $$$\beta$$$ and $$$\alpha$$$ are the phase shift terms. Specifically, $$$\alpha$$$ represents constant phase shift attributed to phase delay of electronics including low-pass/bandpass filters and other electronic channels; $$$\beta$$$ primarily arises from gradient ramps, eddy currents, and frequency-dependent phase delay of electronics. For the T1W IR and reference images, the signal is described by $$S(\omega_{x},\omega_{y}) = C_iT_j\exp\left\{i(\alpha-\beta\omega_x)\right\},$$ where $$$C$$$ represents coil channel sensitivity weight; $$$i$$$ denotes channel index; $$$T$$$ is the signal weight as a function of flip angle and T1, note that it contains the phase-sensitive contrast of interest; and $$$j$$$ labels the image section (0 for reference and 1 for T1W IR).The MDI PSIR reconstruction method is illustrated in Figure 1. In step 1, for each channel the T1W IR image is multiplied by the complex conjugate of the reference image to remove the background phase, followed by a complex summation over all channels. The outcome is the product of the $$$T$$$ weights of IR and reference images. Consequently, in step 2, the reference images from all channels are then combined (e.g. by SOS), hence the $$$T_0$$$ weight is calculated. Then $$$T_0$$$ is removed from $$$S_i$$$, yielding the real part of the image, by which the contrast of interest is attained. For demonstration, a GRE acquisition preceded with a nonselective inversion pulse was performed with a patient at 3.0 T using a uMR 790 scanner (United Imaging Healthcare, Shanghai, China). Bandwidth was 300 Hz/pixel. Flip angles for the T1W IR and reference segments were 20° and 5°, respectively. TR/TE = 5.2/1.9 ms. An acquisition FOV of 320 mm×360 mm and matrix of 171×192 were applied. The thickness was 8 mm. Utilizing parallel imaging, 98 phase encodes were acquired in 8 heartbeats by collecting 28 lines of k-space per heartbeat, given two R-R intervals between inversion pulses.
Results
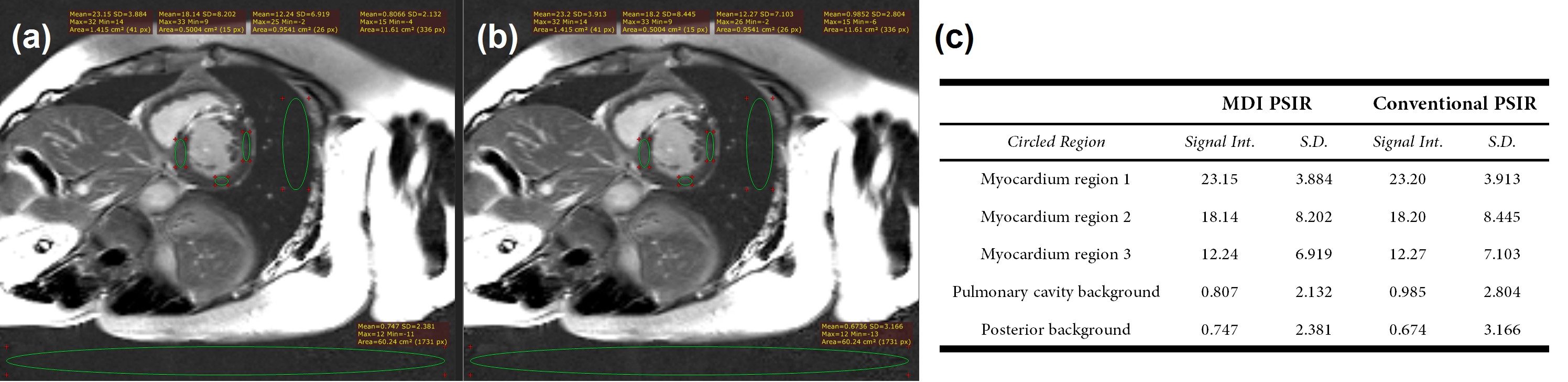
The MDI PSIR reconstruction procedure illustrated in Fig. 1 is substantially simplified compared to the traditional method,1 given that the inefficient combiner coefficient computation becomes unnecessary. Besides, in computing the flip angle and T1-associated weights for the reference images, the more convenient channel combination (e.g. SOS) was employed. Therefore, greatly improved reconstruction efficiency can be achieved.In Figure 2(a), with the new approach, the image signal intensity is almost completely maintained compared with that by the conventional reconstruction shown in Fig. 2(b). The background of consideration here is the gas-filled pulmonary cavity and the broad posterior region. In Fig. 2(c), the notable attenuation of standard deviations (SD’s) in both background regions, along with the slight reduction of SD’s for the myocardium regions, suggest mitigated noise fluctuation by MDI. Overall, the noise level is significantly suppressed using the MDI method, which leads to elevated SNR in this representation.
Discussion and Conclusion
We applied MDI algorithm in place of the classic PSIR reconstruction for cardiac imaging and demonstrated the effectiveness of the approach for fast reconstruction and improved SNR. As with other MDI applications,4 the fundamental concept is that any irrelevant data dimensions with the quantity of interest are processed individually for mapping the quantity or imaging with desired contrast. Without directly combining these dimensions, noise distribution remains unmodified such that no mapping/imaging bias is introduced. In comparison to the conventional reconstruction, the algorithm offers a simplified and fast pathway to achieving desired image contrast, along with a remarkable elevation of SNR. More importantly, the proposed reconstruction method can be conveniently extended to a variety of body parts that demand phase-sensitive T1 contrast, thus providing more insightful clinical value for diagnosis.Acknowledgements
No acknowledgement found.References
1. Kellman, Peter, et al. "Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement." Magnetic Resonance in Medicine 47(2002).
2. Park, HyunWook, et al. "Real-value representation in inversion-recovery NMR imaging by use of a phase-correction method." Magnetic Resonance in Medicine (1986).
3. Ye, Yongquan, et al. "MR relaxivity mapping using multi-dimensional integrated (MDI) complex signal ratio." ISMRM 27th Annual Meeting & Exhibition, Montreal, QC, Canada; 2019, p 4392.
4. Hu, Yichen, et al. “Noise reduction and ghosting alleviation in ASL perfusion measurement using multi-dimensional integration (MDI).” ISMRM 28th Annual Meeting & Exhibition, Sydney, NSW, Australia; 2020, p 6947.
Figures