1040
Brain Function in Obesity: A Pilot Study to Assess Effects of Bariatric Surgery1The University of Texas at Dallas, Richardson, TX, United States, 2The University of Texas at Arlington, Arlington, TX, United States, 3University of Texas Southwestern Medical Center, Dallas, TX, United States
Synopsis
Obesity is an ongoing epidemic that is associated with cognitive dysfunction and is a prominent precursor to a variety of neurogenerative diseases. Bariatric surgery is an effective and long-term weight loss strategy that can improve neurocognitive function. However, the mechanisms that drive these improvements are unknown. In this study, magnetic resonance imaging (MRI) is utilized to assess changes in cerebral metabolic rate of oxygen (CMRO2) levels in bariatric surgery candidates before and after their surgery. These values are compared with normal healthy weight controls of a similar age and reassessed after 2 weeks and 14 weeks.
Purpose
The purpose of this study was to assess the effects of bariatric surgery on cerebral metabolic rate of oxygen (CMRO2) and cognitive function in people with severe/class 3 obesity.Introduction
Obesity is a global epidemic that is linked to a variety of health concerns, which include cardiovascular disease, cancers, and decreased life expectancy. This disease is also associated with cognitive dysfunction and a variety of neurodegenerative and cerebrovascular diseases like Alzheimer’s, dementia, and stroke1-5. The link between obesity and brain function is poorly understood and is the focus of this work.Methods
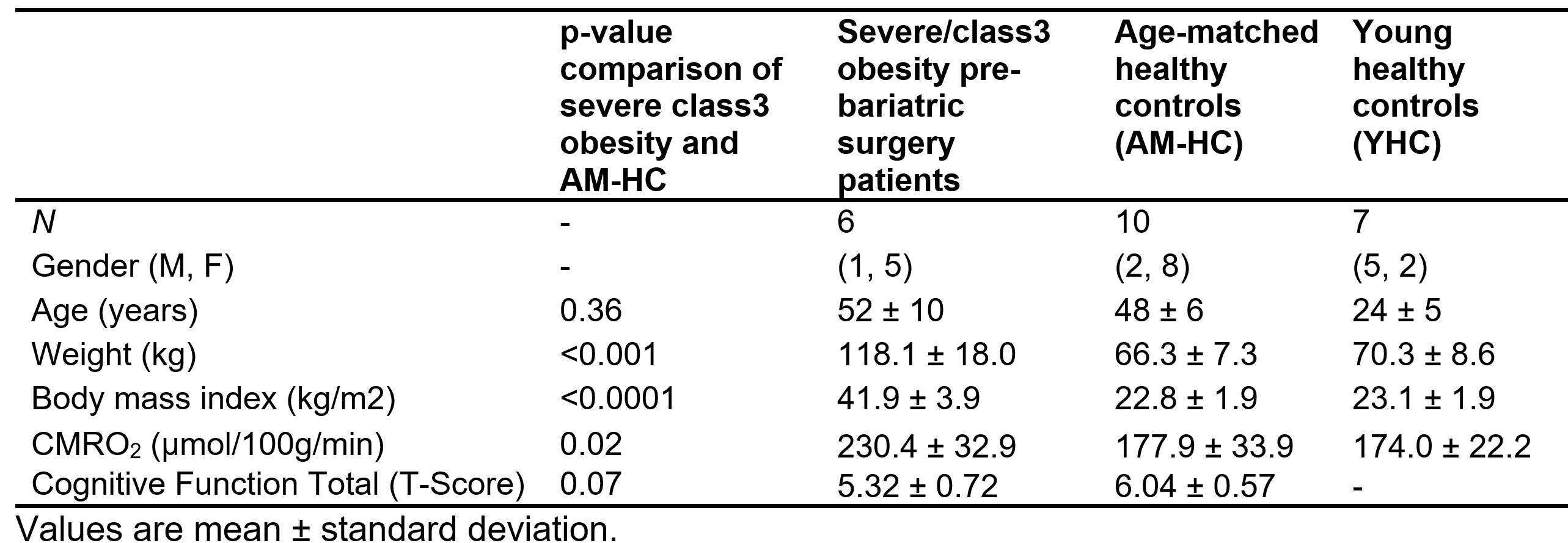
Six bariatric surgery patients with severe/class 3 obesity (52 ± 10 years, 5 females, 41.9 ± 3.9 kg/m2), 10 healthy weight age-matched controls (AM-HC) (48 ± 6 years, 8 females, 22.8 ± 1.9 kg/m2), and seven young healthy controls (YHC) (24 ± 5 years, 2 females, 23.1 ± 1.9 kg/m2) were recruited to this IRB approved study6. All participants granted informed consent.Body mass index (BMI) and CMRO2 were assessed in all participants. Additionally, cognitive function was assessed in the bariatric surgery patients and AM-HC using Integneuro computerized testing battery (Brain Resources Ltd., Australia). Cognitive function in multiple domains was tested and a composite score was generated from all domains.
CMRO2 was calculated using the Fick principle based on the arterio-venous difference in oxygen content7. MRI scans were performed on bariatric surgery patients to determine CMRO2, which was compared to that from AM-HC and YHC. CMRO2 was calculated using the equation: CMRO2 = CBF * (Ya – Yv) * Ca.
Cerebral blood flow (CBF) represents the amount of blood flowing to the brain in mL/100g/min, and is quantified using the phase contract MRI technique. The imaging slice is placed perpendicular to the four arteries that carry blood to the brain: the left and right internal carotids and left and right vertebral arteries. The flux in these four major feeding arteries is measured using an in-house MATLAB script. Regions of interest (ROI) were drawn on these four arteries to obtain the integrated flux within each artery in the units of mL/min. The combined flux from the four arteries determines the total flux. To determine CBF in mL/100g/min, total brain volume, which is the sum of gray matter and white matter, was obtained from the T1-weighted image and normalized to the CBF. Ya (arterial oxygenation) was measured for each participant using a pulse oximeter. Yv (oxygenation in venous vessels) was measured using a technique called T2‐Relaxation‐Under‐Spin‐Tagging (TRUST) MRI8. An imaging slice was placed over the sagittal sinus that drains venous blood from the brain. T2 value for sagittal sinus blood was then estimated and converted to Yv using a calibration plot. Ca is the amount of oxygen molecules that a unit volume of blood can carry and is assumed from literature at 8.97 µmol O2 per ml of blood.
Results and Discussion
Bariatric surgery resulted in significant reduction in BMI (Figure 1a) and increase in cognitive function (Figure 1b). CMRO2 in the YHC was similar to values previously reported. Pre surgery bariatric surgery patients with severe/class 3 obesity had significantly higher (29.5%) CMRO2 compared to AM-HC (p = 0.02). Two weeks post-surgery, the CMRO2 value was still significantly elevated compared to the AM-HC (p = 0.003), suggesting that changes do not occur early in the post-operative course, independent of weight loss (Figure 2). However, fourteen-weeks post-surgery the CMRO2 in patients was not significantly different compared to the AM-HC. These results suggest that bariatric surgery was associated with normalization of the CMRO2 in patients with severe/class 3 obesity. The cognitive function total score was higher in the AM-HC compared to bariatric patients pre-surgery, but was not significant (p = 0.07), probably due to the small sample size (n = 6 bariatric patients). The patients with severe/class 3 obesity showed an increase in cognitive function following bariatric surgery and weight loss (Figure 1b). CMRO2 (p = 0.004) and CBF (p = 0.02) were observed to be significantly correlated with BMI by combining all subjects (YHC, AM-HC, severe/class 3 obesity patients at the pre-surgery stage) (Figure 3). We believe we are the first group to report a significant correlation between CMRO2 and BMI.Conclusion
These results suggest that bariatric surgery patients with severe/class 3 obesity have significantly higher CMRO2 than healthy weight counterparts, and that bariatric surgery and weight loss are associated with normalization in CMRO2. The higher CMRO2 may indicate that brain function of patients with severe/class 3 obesity is less efficient requiring more blood flow to perform similar functions compared with brain function of their age-matched healthy-weight counterparts. Cognitive function also improves with bariatric surgical weight loss in patients with severe/class 3 obesity. Overall, bariatric surgery is beneficial in losing weight and improving brain function. Future studies must assess if these benefits are durable and related to the type of surgery or magnitude of weight loss. The impact of non-surgical weight loss such as calorie restriction, anti-obesity medications, and exercise should be explored in future studies.Acknowledgements
No acknowledgement found.References
1. Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation. Mar 7 2017;135(10):e146-e603. doi:10.1161/CIR.0000000000000485
2. Spitznagel MB, Hawkins M, Alosco M, et al. Neurocognitive Effects of Obesity and Bariatric Surgery. Eur Eat Disord Rev. Nov 2015;23(6):488-95. doi:10.1002/erv.2393
3. Prickett C, Brennan L, Stolwyk R. Examining the relationship between obesity and cognitive function: a systematic literature review. Obes Res Clin Pract. Mar-Apr 2015;9(2):93-113. doi:10.1016/j.orcp.2014.05.001
4. Mitchell AB, Cole JW, McArdle PF, et al. Obesity increases risk of ischemic stroke in young adults. Stroke. Jun 2015;46(6):1690-2. doi:10.1161/STROKEAHA.115.008940
5. Gorospe EC, Dave JK. The risk of dementia with increased body mass index. Age Ageing. Jan 2007;36(1):23-9. doi:10.1093/ageing/afl123
6. Tucker WJ, Thomas BP, Puzziferri N, et al. Impact of bariatric surgery on cerebral vascular reactivity and cognitive function: a non-randomized pilot study. Pilot Feasibility Stud. 2020;6:21. doi:10.1186/s40814-020-00569-2
7. Thomas BP, Sheng M, Tseng BY, et al. Reduced global brain metabolism but maintained vascular function in amnestic mild cognitive impairment. J Cereb Blood Flow Metab. Apr 2017;37(4):1508-1516. doi:10.1177/0271678X16658662
8. Lu H, Ge Y. Quantitative evaluation of oxygenation in venous vessels using T2-Relaxation-Under-Spin-Tagging MRI. Magn Reson Med. Aug 2008;60(2):357-63. doi:10.1002/mrm.21627
Figures