1017
Simultaneous acquisition for magnetic resonance elastography and fat quantification of the liver1School of Biomedical Engineering, Shanghai Jiao Tong University, Shanghai, China
Synopsis
Magnetic resonance elastography (MRE) has been used for tumor detection and liver fibrosis evaluation. The existence of intratumoral fat suggests a lower risk of microvascular invasion of combined hepatocellular-cholangiocarcinoma. The combination of MRE and fat quantification can provide sufficient sensitivity to detect substantial macrovesicular hepatic steatosis or fibrosis. In clinical practice, MRE and fat quantification are scanned separately. However, this may cause slice mis-registration between MRE and fat quantification, and increase scan time. In this study, the feasibility of simultaneous acquisition for MRE and fat quantification was demonstrated. This technique can have several potential clinical applications without increasing scan time.
Introduction
Magnetic resonance elastography (MRE) has been applied clinically as a noninvasive method for tumor detection and liver fibrosis evaluation.1,2 The existence of intratumoral fat suggests a lower risk of microvascular invasion of combined hepatocellular-cholangiocarcinoma.3 The combination of MRE and MR fat quantification can provide sufficient sensitivity to detect substantial macrovesicular hepatic steatosis or fibrosis.4 In clinical practice, MRE and MR fat quantification are scanned separately.5 MRE is typically performed by using a motion-sensitizing gradient-echo sequence5, and fat quantification is typically performed by using a multi-echo chemical-shift imaging sequence6. However, the separated scans may cause slice mis-registration between MRE and fat quantification, and increase the total scan time. The aim of this study is to develop a technique for simultaneous acquisition for MRE and fat quantification without increasing scan time.Methods
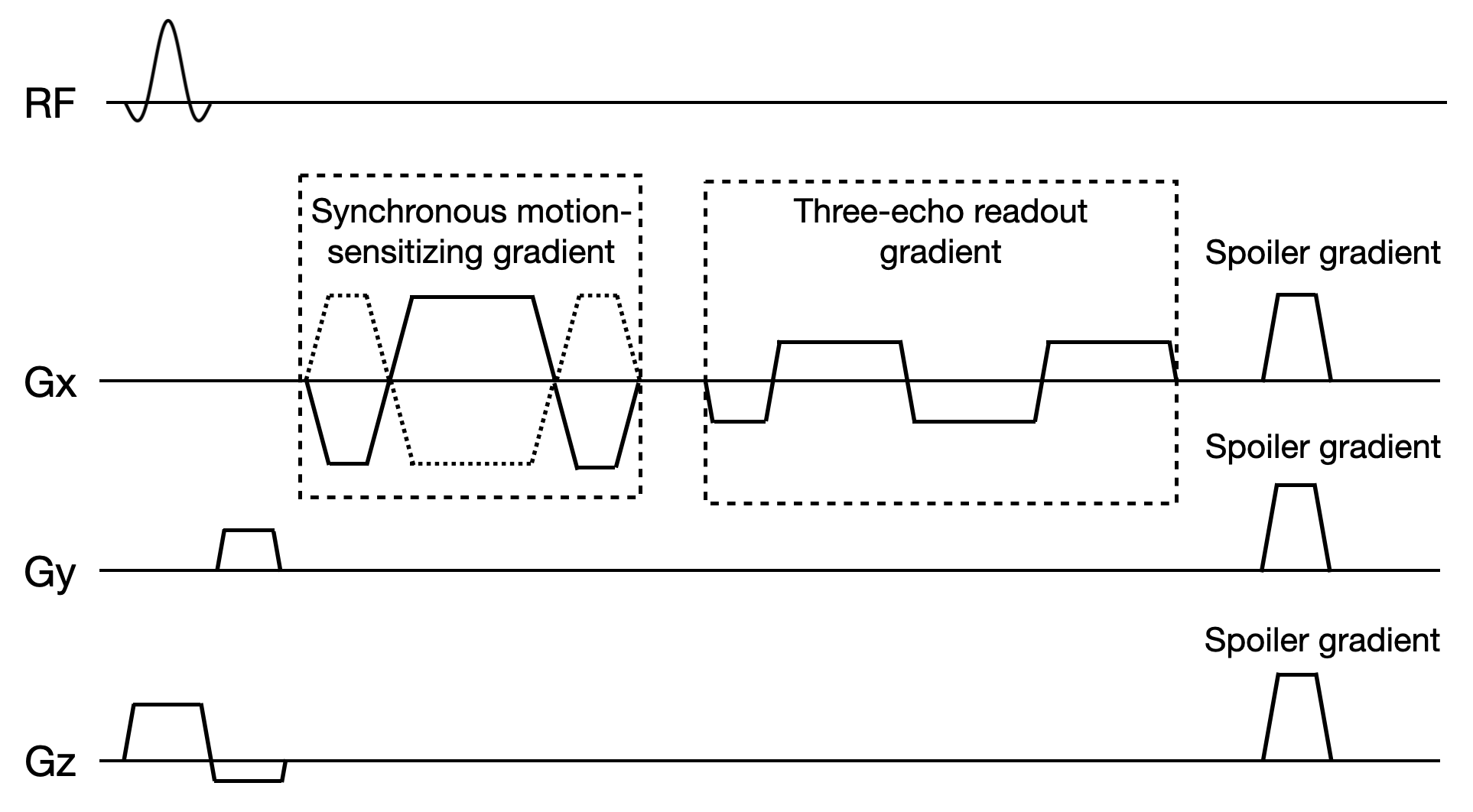
Six healthy volunteers with ages ranged from 23 to 25 years (median age 24 years) were scanned in this study. All scans were performed on a 3.0 T uMR790 scanner (Shanghai United Imaging Healthcare Co., Ltd., Shanghai, China). A 12-channel phase-array coil and a 12-channel knee coil were used for data acquisition in liver and lower-extremity, respectively. An electromagnetic actuator7 was placed on the subject’s right upper abdomen to transmit low-amplitude vibrations to the liver for the generation of hepatic shear waves. All subjects were instructed to hold breath for about 15 seconds at the end of expiration. A motion-sensitizing multi-gradient-echo sequence was developed for simultaneous acquisition for MRE and fat quantification. The diagram of the three-echo MRE sequence is shown in Figure 1. The first echo was used for MRE reconstruction. A three-point Dixon technique was used for fat quantification. The proposed sequence was also performed on lower-extremity to evaluate the difference of fat quantification between actuator turned off and on. The scan parameters were as follows: mechanical frequency = 100 Hz, number of phase offsets = 4, TR = 50 ms, TE = 13.42/14.54/15.66 ms, flip angle = 30◦, bandwidth = 700 Hz/pixel, slice thickness = 10 mm, number of readouts = 256 for liver and 192 for lower-extremity, FOV = 300 × 300 mm2 for liver and 150 × 150 mm2 for lower-extremity. GRAPPA was used to accelerate data acquisition with an acceleration factor of 2.Results
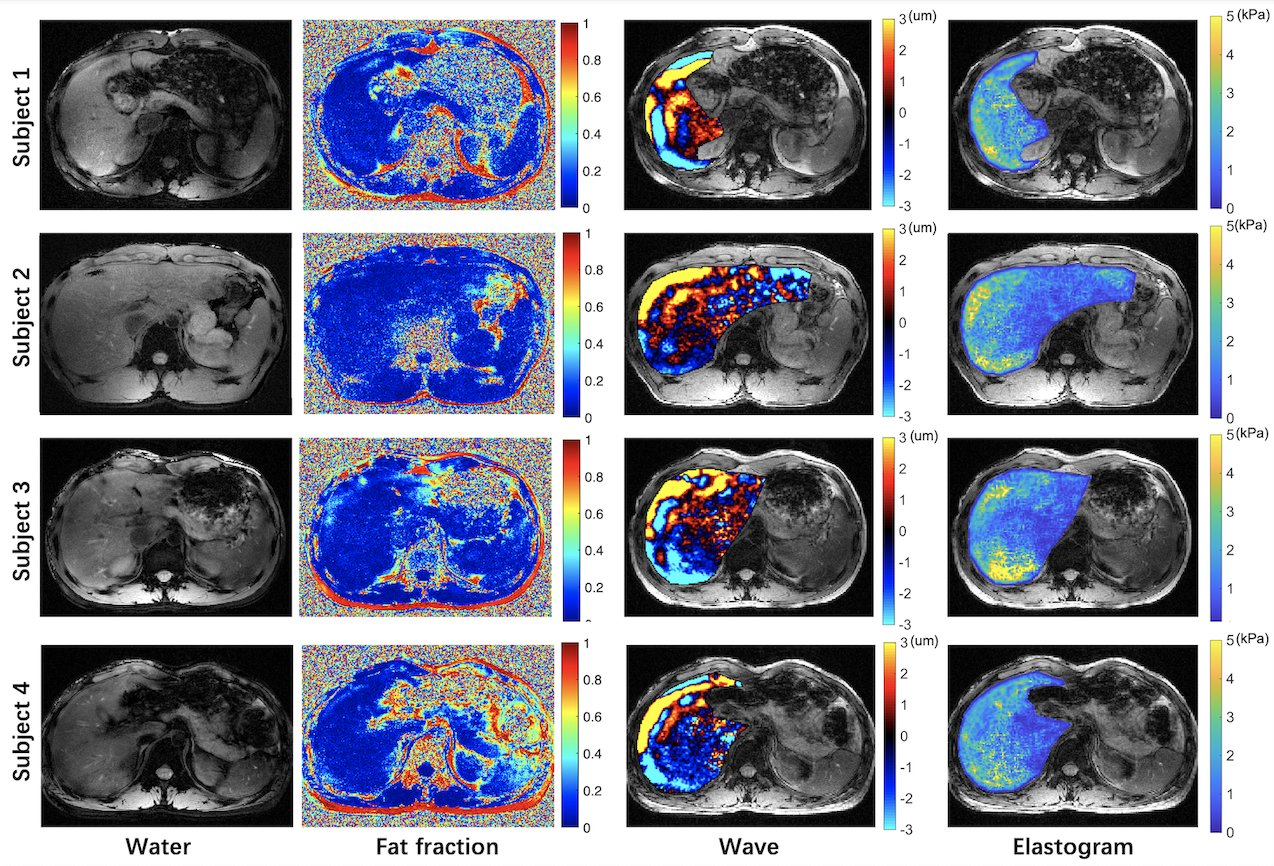
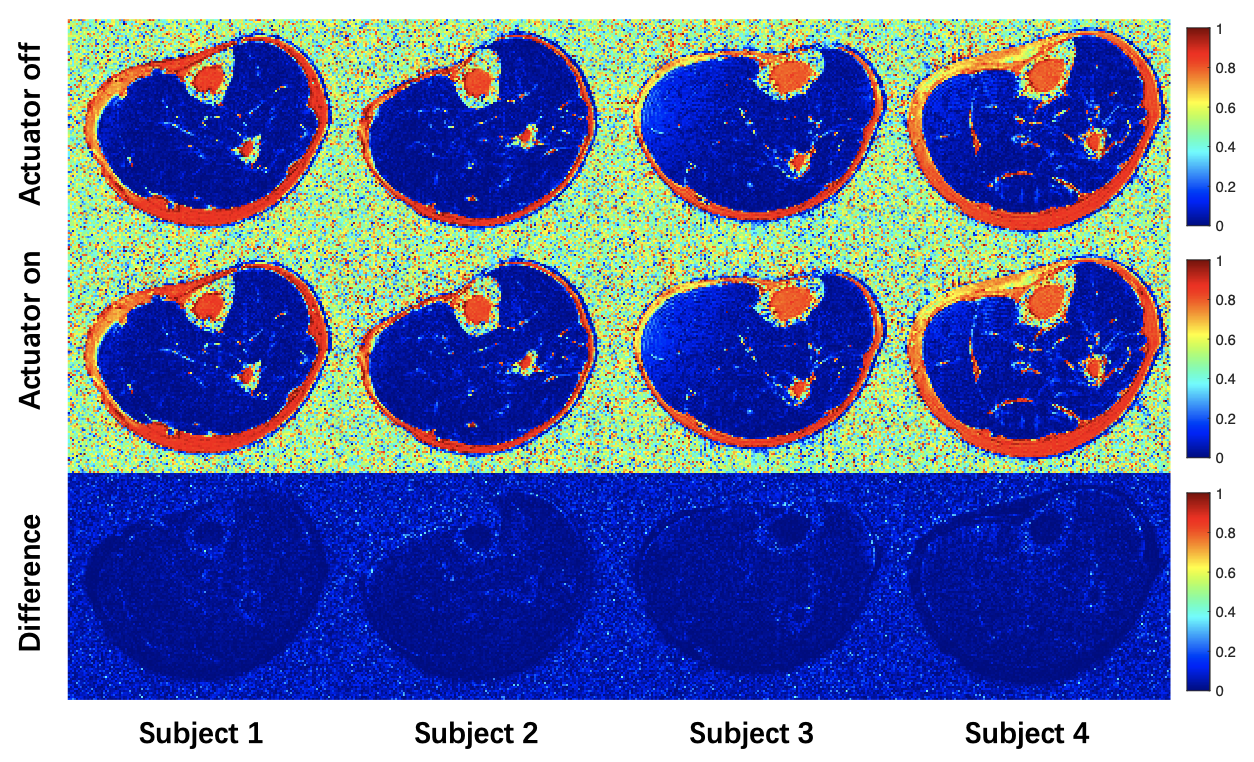
Figure 2 shows the water images, fat fraction maps, wave images and elastograms in four out of six subjects as the other two subjects fail to produce proper wave images and elastograms. The wave images and elastograms were reconstructed in the liver. Figure 3 shows the fat fraction maps of lower-extremity with actuator turned off and on in four out of six subjects. The fat fraction maps with actuator turned off and on were visually comparable.Discussion
The proposed multi-echo MRE sequence enables simultaneous acquisition for MRE and fat quantification. Generally, there is 10 ~ 40 ms idle time between readout gradient and the next radio-frequency excitation in MRE sequence.5,8 This idle time was used in the proposed technique to acquire the multiple echoes without increasing TR. The first echo was used for MRE reconstruction, and the in-phase and out-of-phase echoes were used for fat quantification. In this feasibility study, four breath-holds were required in each subject. Any mis-registration of these breath-holds can result in degradation of MRE quality. In the two subjects who fail to produce proper wave images and elastograms, considerable mis-registration was observed among the four breath-holds. It is desirable to speed up data acquisition so that single breath-hold is sufficient for both MRE and fat quantification in the future. It can be expected that the failure rate can be substantially reduced with improved acquisition techniques.Conclusion
In this preliminary study, the feasibility of simultaneous acquisition for MRE and fat quantification was demonstrated. This technique can have several potential clinical applications without increasing scan time. These applications include the risk evaluation of microvascular invasion of combined hepatocellular-cholangiocarcinoma, and the detection of substantial macrovesicular hepatic steatosis or fibrosis.Acknowledgements
The authors are thankful for the assistance of United Imaging Healthcare. Funding support from grant 31870941 from National Natural Science Foundation of China (NSFC) and grant 1944190700 from Shanghai Science and Technology Committee (STCSM) are acknowledged.References
1. Sofue K, Onoda M, Tsurusaki M, et al. Dual-frequency MR elastography to differentiate between inflammation and fibrosis of the liver: Comparison with histopathology. J Magn Reson Imaging. 2020;51(4):1053-1064.
2. Poterucha JT, Johnson JN, Qureshi MY, et al. Magnetic Resonance Elastography: A Novel Technique for the Detection of Hepatic Fibrosis and Hepatocellular Carcinoma After the Fontan Operation. Mayo Clin Proc. 2015;90(7):882-894.
3. Wang X, Wang W, Ma X, et al. Combined hepatocellular-cholangiocarcinoma: which preoperative clinical data and conventional MRI characteristics have value for the prediction of microvascular invasion and clinical significance? Eur Radiol. 2020;30(10):5337-5347.
4. Yoon JH, Lee JM, Suh KS, et al. Combined Use of MR Fat Quantification and MR Elastography in Living Liver Donors: Can It Reduce the Need for Preoperative Liver Biopsy? Radiology. 2015;276(2):453-464.
5. Kim M, Kang BK, Jun DW, et al. MR elastography of the liver: comparison of three measurement methods. Clin Radiol. 2020;75(9):715 e711-715 e717.
6. Armstrong T, Ly KV, Murthy S, et al. Free-breathing quantification of hepatic fat in healthy children and children with nonalcoholic fatty liver disease using a multi-echo 3-D stack-of-radial MRI technique. Pediatr Radiol. 2018;48(7):941-953.
7. Feng Y, Zhu M, Qiu S, et al. A multi-purpose electromagnetic actuator for magnetic resonance elastography. Magn Reson Imaging. 2018;51:29-34.
8. Kim DW, Kim SY, Yoon HM, et al. Comparison of technical failure of MR elastography for measuring liver stiffness between gradient-recalled echo and spin-echo echo-planar imaging: A systematic review and meta-analysis. J Magn Reson Imaging. 2020;51(4):1086-1102.
Figures