0987
High resolution whole-heart coverage multiband first-pass myocardial perfusion MRI using the slice-L+S reconstruction method1Biomedical Engineering, University of Virginia, Charlottesville, VA, United States, 2Medicine, University of Virginia, Charlottesville, VA, United States, 3Electrical and Computer Engineering, University of Virginia, Charlottesville, VA, United States, 4Radiology, University of Virginia, Charlottesville, VA, United States
Synopsis
k-t undersampled multiband first-pass perfusion imaging provides in-plane and through-plane acceleration and potentially enables high spatial resolution and whole-heart coverage. Our slice-L+S work splits MB data consistency and enforcing L+S into two subproblems wherein MB data, in- and through-plane coil information and L+S properties of slices are systematically utilized. Here we compare slice-L+S to single-band L+S and slice-GRAPPA followed sequentially by L+S (seq-SG-L+S) using 3 retrospectively undersampled datasets. High resolution nine-slice data with multiband factor-3 and rate-3 undersampling were prospectively acquired in 4 patients. Slice-L+S showed better image quality demonstrated by quantitative results and scores from two cardiologists.
Purpose
First-pass MRI is routinely used to image myocardial perfusion1. However, achieving high spatial-temporal resolution, high slice coverage and high signal-to-noise-ratio is challenging2,3. k-t undersampled multiband (MB) methods may meet these challenges, and for this purpose we recently developed a slice-low rank plus sparse (slice-L+S) reconstruction model2 that integrates MB data consistency4 with low-rank plus sparse constraints. The purposes of the present study were to (a) compare MB slice-L+S with k-t undersampled single-band (SB) first-pass imaging using an L+S reconstruction and equal total acceleration factor, and (b) compare the integrated slice-L+S reconstruction method with the sequential operations of split slice-GRAPPA followed by single-band L+S (seq-SG-L+S) for the reconstruction of k-t undersampled MB first-pass data. We focused on Cartesian imaging because it is the most widely used trajectory and we targeted rate-6-9 acceleration in order to cover 6-9 slices with 1.5mm×1.5mm in-plane resolution.Methods
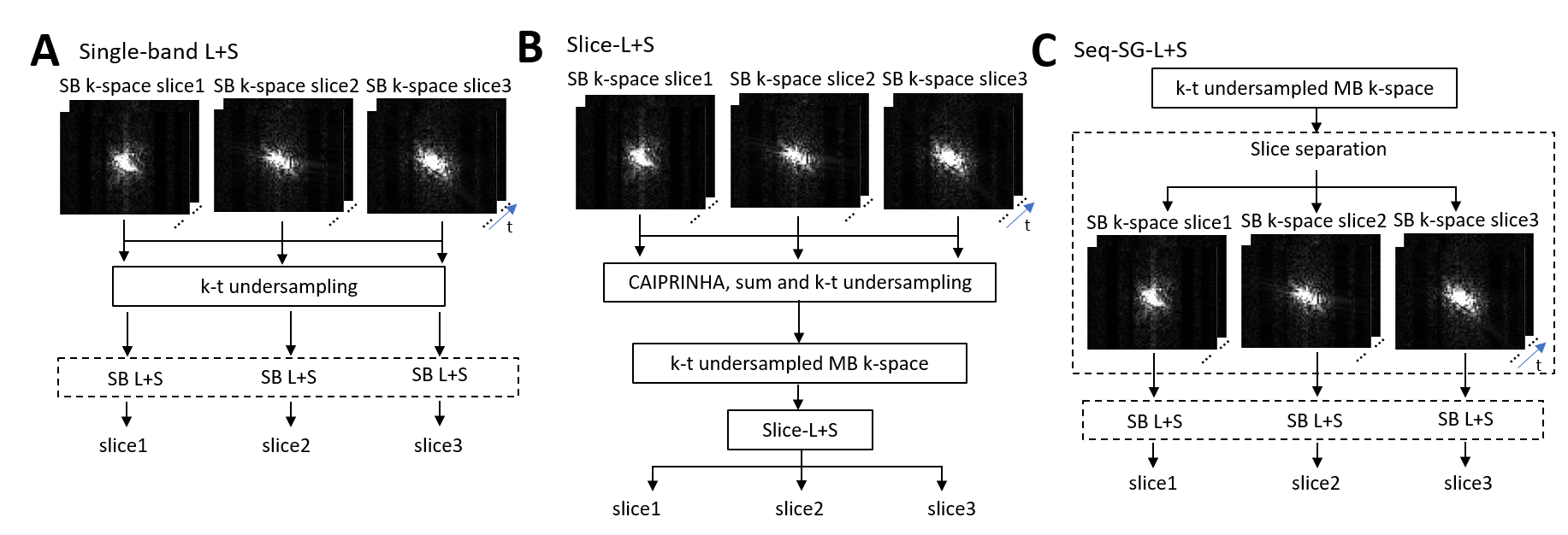
A saturation-recovery gradient-echo sequence was modified to use MB excitation with CAIPIRINHA5 phase modulation and Poisson-disk k-t undersampling. SB calibration data were acquired in the first heartbeat, and were used to calibrate ESPIRiT6 maps and split slice-GRAPPA kernels7 for each slice. Fully-sampled SB first-pass perfusion images were similarly acquired and used to retrospectively synthesize various k-t undersampled MB datasets (Figure 1). Imaging was performed on a 1.5T system (Aera, Siemens) using 20-34 receiver channels. Fully-sampled SB datasets from 3 patients were acquired using 3 slices and a spatial resolution of 3.3mm×3.3mm. To compare MB slice-L+S with SB L+S using an equal total acceleration factor, we retrospectively synthesized k-t undersampled MB and SB data from the fully-sampled SB data (Figure 1). The MB slice-L+S reconstruction used a MB factor of 3 (MB=3) and k-t underampling factors of 2 and 3 (R=2 and R=3), for total accelerations of 6 and 9. The SB L+S reconstruction used R=6 and 9 (MB=1). To compare the different MB reconstruction methods (slice-L+S vs seq-SG-L+S), we again retrospectively synthesized data and we additionally acquired 4 prospectively undersampled MB first-pass datasets. These acquisitions used MB=3, R=3, spatial resolution of 1.5mm×1.5mm, nine total slices, and a temporal footprint of 169ms per slice. The results of the MB (MB=3, R=2 and R=3) vs SB (R=6 and 9) comparisons were quantified using normalized root mean squared error (nRMSE) and structural similarity (SSIM). The results of the slice-L+S and seq-SG-L+S reconstructions of synthesized data were quantified using nRMSE and SSIM, and those of the prospectively acquired undersampled MB data were scored by two cardiologists (1-5, 5 is best).Results
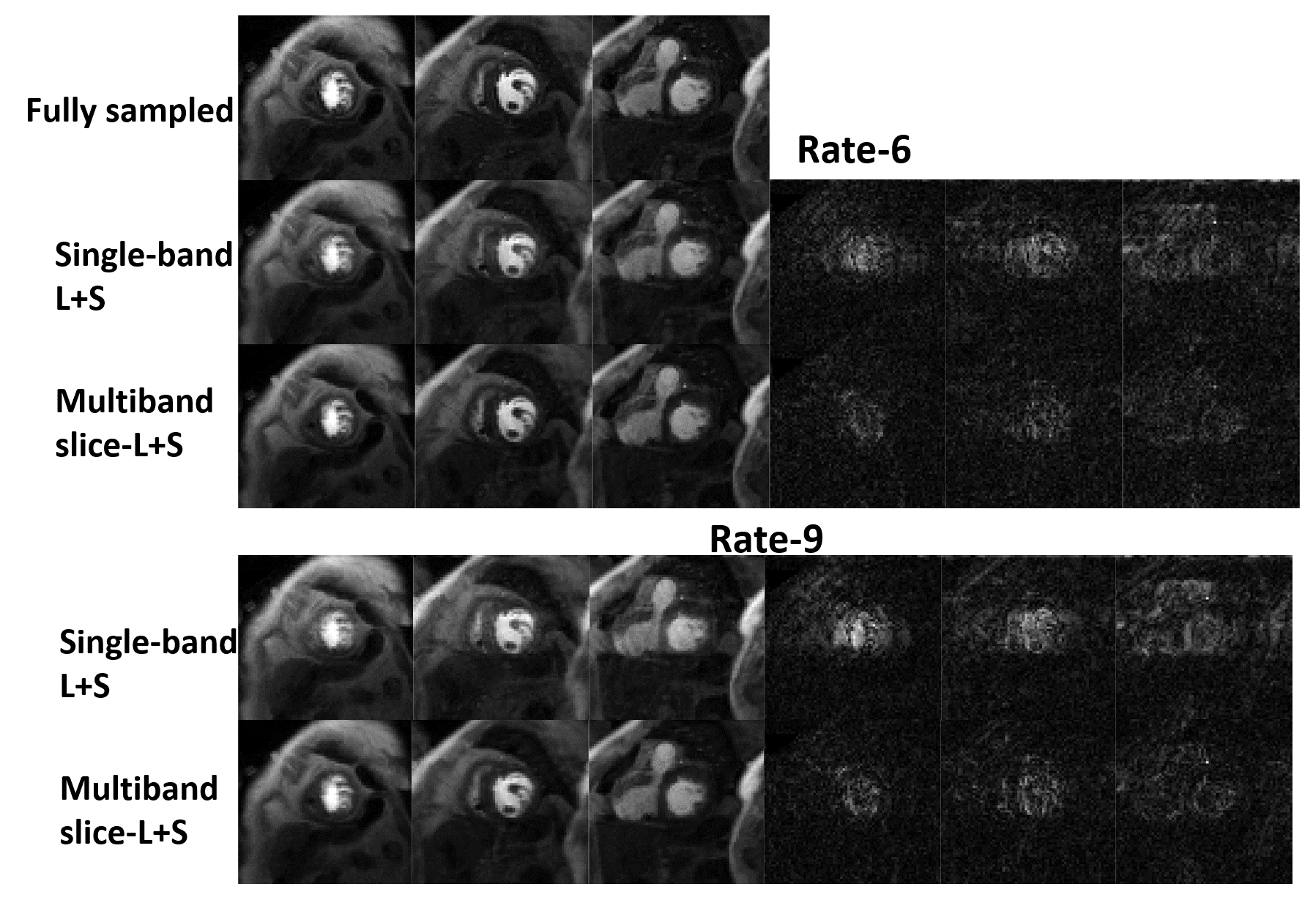
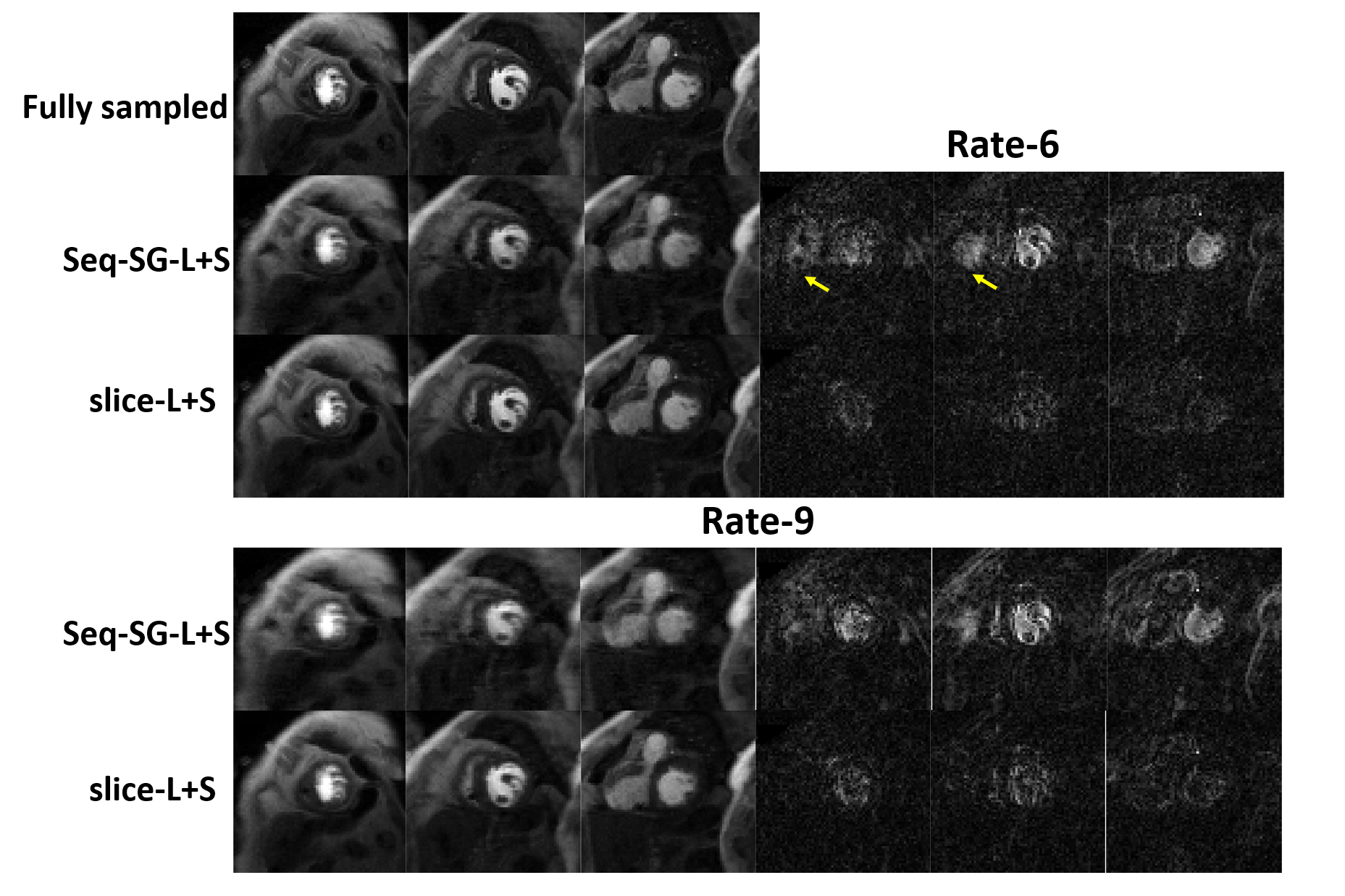
For the comparison of MB slice-L+S and SB L+S using an equal total acceleration factor, Figure 2 shows example reconstructions using both methods for total accelerations of rate 6 and rate 9. MB slice-L+S outperformed SB L+S in both cases. For rate 6, the mean nRMSE and SSIM of slice-L+S were 23% lower and 2.2% higher than SB L+S. At rate-9, the mean nRMSE and SSIM of slice-L+S were 27% lower and 4.8% higher than SB L+S. For the comparison of MB slice-L+S and MB seq-SG-L+S, Figure 3 shows example reconstructions using both methods for total accelerations of rate 6 (MB=3, R=2) and rate 9 (MB=3, R=3), demonstrating that slice-L+S produced lower overall artifacts. Example images and movies demonstrating the better image quality of slice-L+S vs seq-SG-L+S with MB=3 and R=3 are shown in Figures 4 and 5, demonstrating 9-slice coverage with 1.5mm×1.5mm spatial resolution. At rate-6, the mean nRMSE and SSIM of slice-L+S were 25% lower and 4.6% higher than seq-SG-L+S. At rate-9, the mean nRMSE and SSIM of slice-L+S were 32% lower and 8.6% higher than seq-SG-L+S. The cardiologist scoring results were 2.6 ± 0.58 vs 4.1 ± 0.73 (p<0.001) for seq-SG-L+S and slice-L+S, respectively, with very close agreement noted between observer ratings for the images (r=0.92, p=0.001).Discussion
These results suggest that slice-L+S for the reconstruction of k-t undersampled MB first-pass images provides better image quality than L+S reconstructions of SB first-pass images with the same total accelerations of rate 6-9. Further, for undersampled MB first-pass imaging, the integrated slice-L+S method outperforms the sequential operations of split-slice-GRAPPA and L+S. Slice-L+S with MB=3 and R=3 at 1.5T provides high spatial resolution (1.5mm×1.5mm) and nine slices, as well as good image quality as judged by expert readers. In the future, additional datasets will be acquired and analyzed to confirm the present results.Acknowledgements
This work was supported by R01HL147104.References
- Kramer CM, Barkhausen J, Flamm SD, Kim RJ, Nagel E, Society for Cardiovascular Magnetic Resonance Board of Trustees Task Force on Standardized P. Standardized cardiovascular magnetic resonance (CMR) protocols 2013 update. J Cardiovasc Magn Reson 2013;15:91.
- Sun C, Robinson A, Schumann C, Salerno M, Epstein FH. Multiband first-pass perfusion MRI using slice-low-rank plus sparse. ISMRM 2020:1097.
- Otazo R, Candes E, Sodickson DK. Low-rank plus sparse matrix decomposition for accelerated dynamic MRI with separation of background and dynamic components. Magn Reson Med 2015;73(3):1125-1136.
- Sun C, Yang Y, Cai X, Salerno M, Meyer CH, Weller D, Epstein FH. Non-Cartesian slice-GRAPPA and slice-SPIRiT reconstruction methods for multiband spiral cardiac MRI. Magn Reson Med 2020;83(4):1235-1249.
- Breuer FA, Blaimer M, Heidemann RM, Mueller MF, Griswold MA, Jakob PM. Controlled aliasing in parallel imaging results in higher acceleration (CAIPIRINHA) for multi-slice imaging. Magn Reson Med 2005;53(3):684-691.
- Uecker M, Lai P, Murphy MJ, Virtue P, Elad M, Pauly JM, Vasanawala SS, Lustig M. ESPIRiT--an eigenvalue approach to autocalibrating parallel MRI: where SENSE meets GRAPPA. Magn Reson Med 2014;71(3):990-1001.
- Cauley SF, Polimeni JR, Bhat H, Wald LL, Setsompop K. Interslice leakage artifact reduction technique for simultaneous multislice acquisitions. Magn Reson Med 2014;72(1):93-102.
Figures