0980
Combined simultaneous multi-slice (SMS) bSSFP & compressed sensing (CS) for accelerated late gadolinium enhancement (LGE) imaging in the heart1King's College London, London, United Kingdom, 2School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 3IRCCS San Camillo Hospital, Venice, Italy, 4MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom, 5Siemens Healthcare GmbH, Erlangen, Germany, 6MR Research Collaborations, Siemens Healthcare Limited, Melbourne, Australia
Synopsis
SMS-bSSFP combined with compressed sensing was successfully used to acquire LGE images through the use of multiple single-shot dynamic acquisitions in one breath-hold. Instead of 1 slice per breath-hold, 3 slices could be acquired per breathhold.
Introduction
Late-gadolinium enhancement (LGE) imaging is the gold standard technique for non-invasive assessment of myocardial scar in cardiac MR (CMR) examinations (1). LGE imaging is typically performed using an inversion recovery sequence with segmented readout during breath-holding (2). Simultaneous multi-slice bSSFP acquisitions can be combined with pseudorandom under-sampling and compressed sensing (CS) reconstruction (SMS-bSSFP CS) to acquire multiple slices simultaneously using high spatio-temporal acceleration factors (3,4). In this study we sought to investigate the potential of SMS-bSSFP CS with high acceleration factor to enable LGE imaging with increased spatial coverage per breathhold.Methods
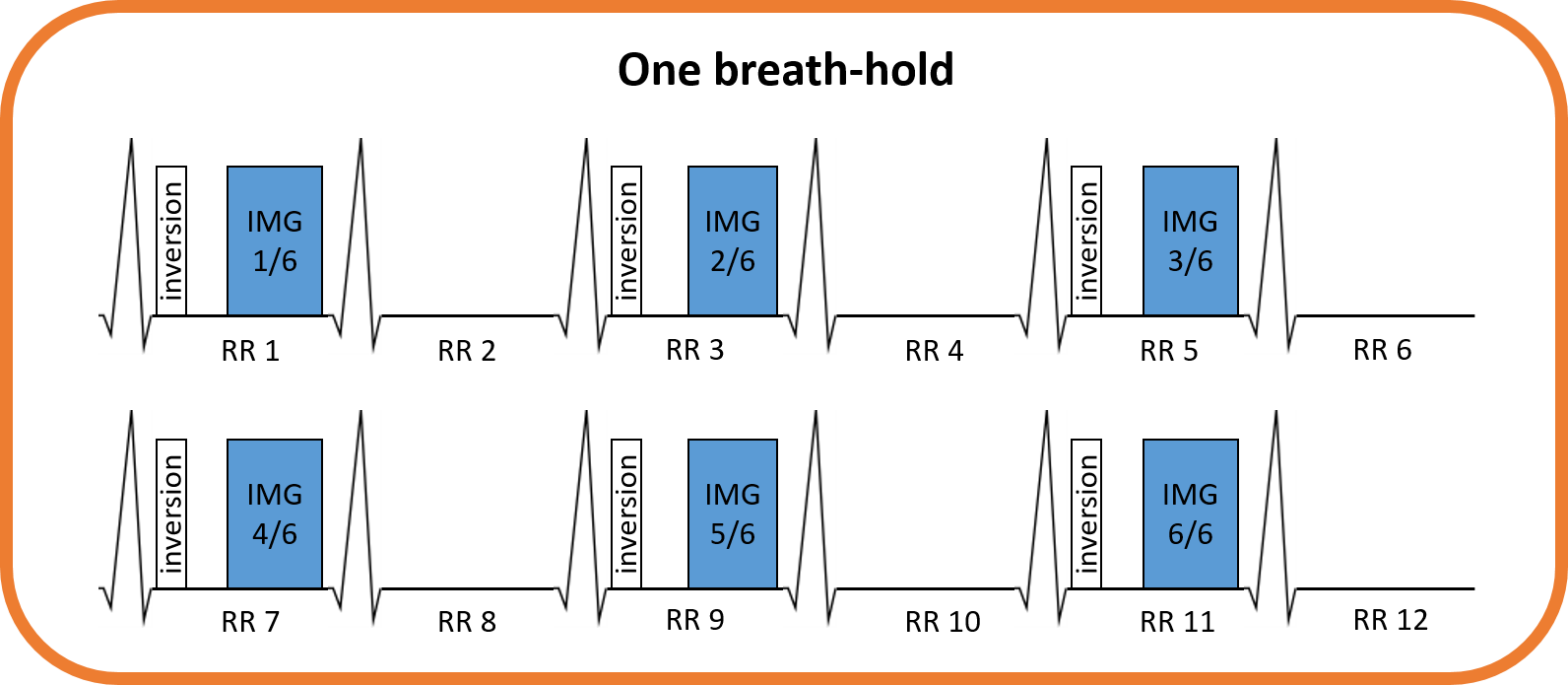
Proposed sequenceA diagram of the proposed prototype LGE sequence is shown in Figure 1. An inversion recovery ECG-triggered sequence is used with a 2-RR acquisition scheme to reduce sensitivity to heartrate variations. The acquisition module in a given heartbeat corresponds to a single-shot acquisition of 3 slices using SMS-bSSFP with pseudorandom undersampling. Dynamic acquisitions (N=6) were employed to allow multiple acquisitions of the same set of 3 slices in one breathhold of 12 heartbeats.
The SMS-bSSFP module was performed with multiband (MB) factor 3 (4) and uses CAIPIRINHA encoding (5), GC-LOLA correction (6), and pseudo-random undersampling (3). The pseudorandom undersampling scheme was extended from MB2 (3) and includes full sampling of a central region and under-sampling of (peripheral) k-space lines while maintaining the required SMS-bSSFP phase cycling and k-space phase ramp. This pseudo-random undersampling was applied to each dynamic independently to achieve temporal incoherence. Images were reconstructed using a nonlinear iterative CS framework with L1 regularisation in the spatial and temporal wavelet domain (3,7). A low spatial regularisation factor (5×10-4) and high temporal regularisation factor (0.1) were used.
Experimental evaluation
Four patients were scanned at 1.5T (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany), 10 minutes after injection of contrast. Inversion times were individually determined to null the myocardial signal based on a prior Look-Locker scan. Each patient was scanned with two LGE sequences, each using a non-selective inversion-recovery 2 RR ECG-triggered bSSFP sequence in short axis orientation and the following parameters:
- Proposed SMS-bSSFP sequence: multiband factor: 3, in-plane under-sampling factor: 3.33, fully sampled k-space lines: 9, external reference lines: 176, dynamics: 6, TR/TE: 3ms/1.27ms, BW: 801 Hz/pixel, flip angle: 40°, matrix size: 240 (1.50x1.50 mm2 voxel size at 360x360mm2 FOV), slice thickness: 8mm, data acquisition window: 216 ms, dummy shots: 0, breathhold duration: 12 heart beats, 3 slices per breathhold, 3 slices acquired.
- Conventional sequence for reference: TR/TE: 2.8ms/1.14ms, BW: 801 Hz/pixel, flip angle: 45°, matrix size: 208 (1.73x1.73 mm2 voxel size at 360x360mm2 FOV), slice thickness: 8mm, data acquisition window: 191 ms, 3 shots per slice, 1 dummy shot, breathhold duration: 8 heart beats, 1 slice per breathhold, 3 slices acquired.
Results
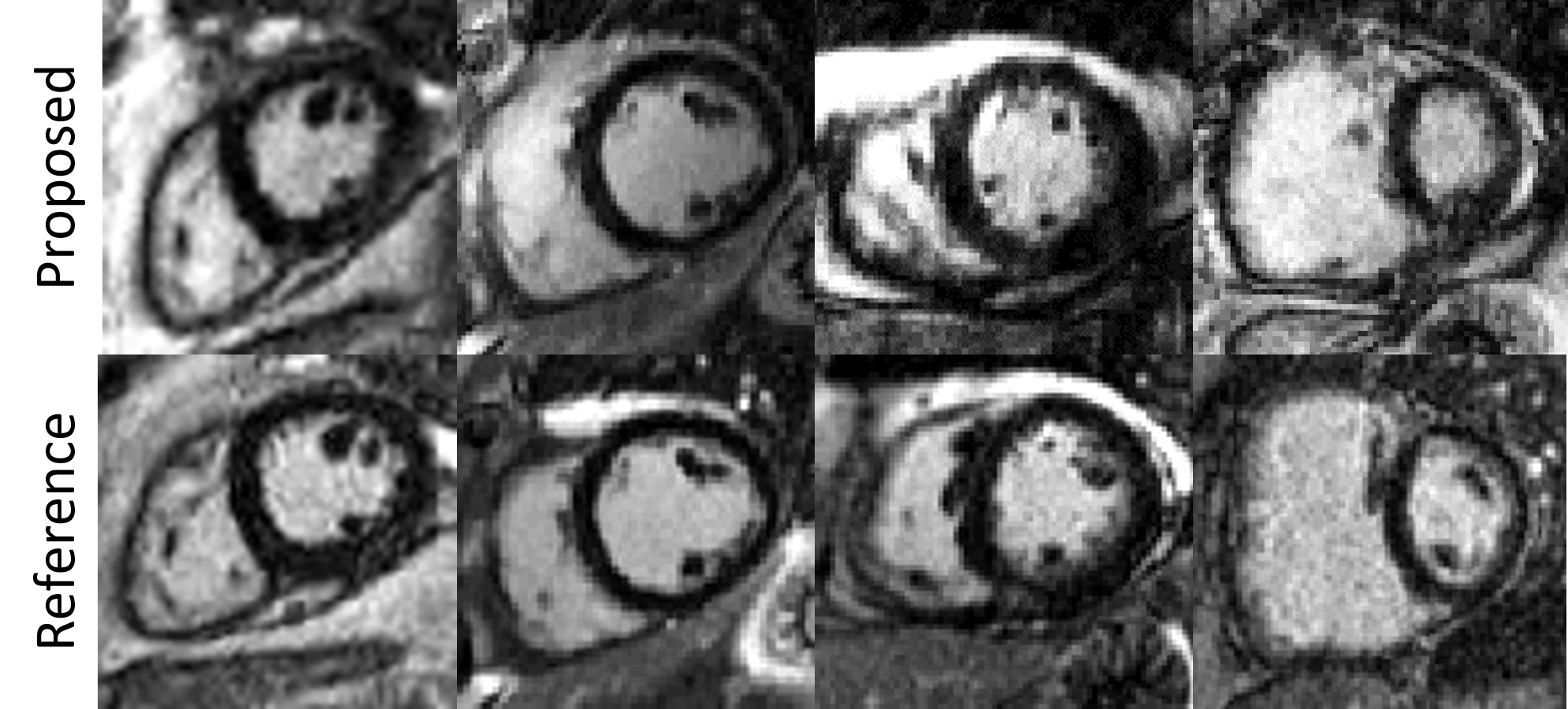
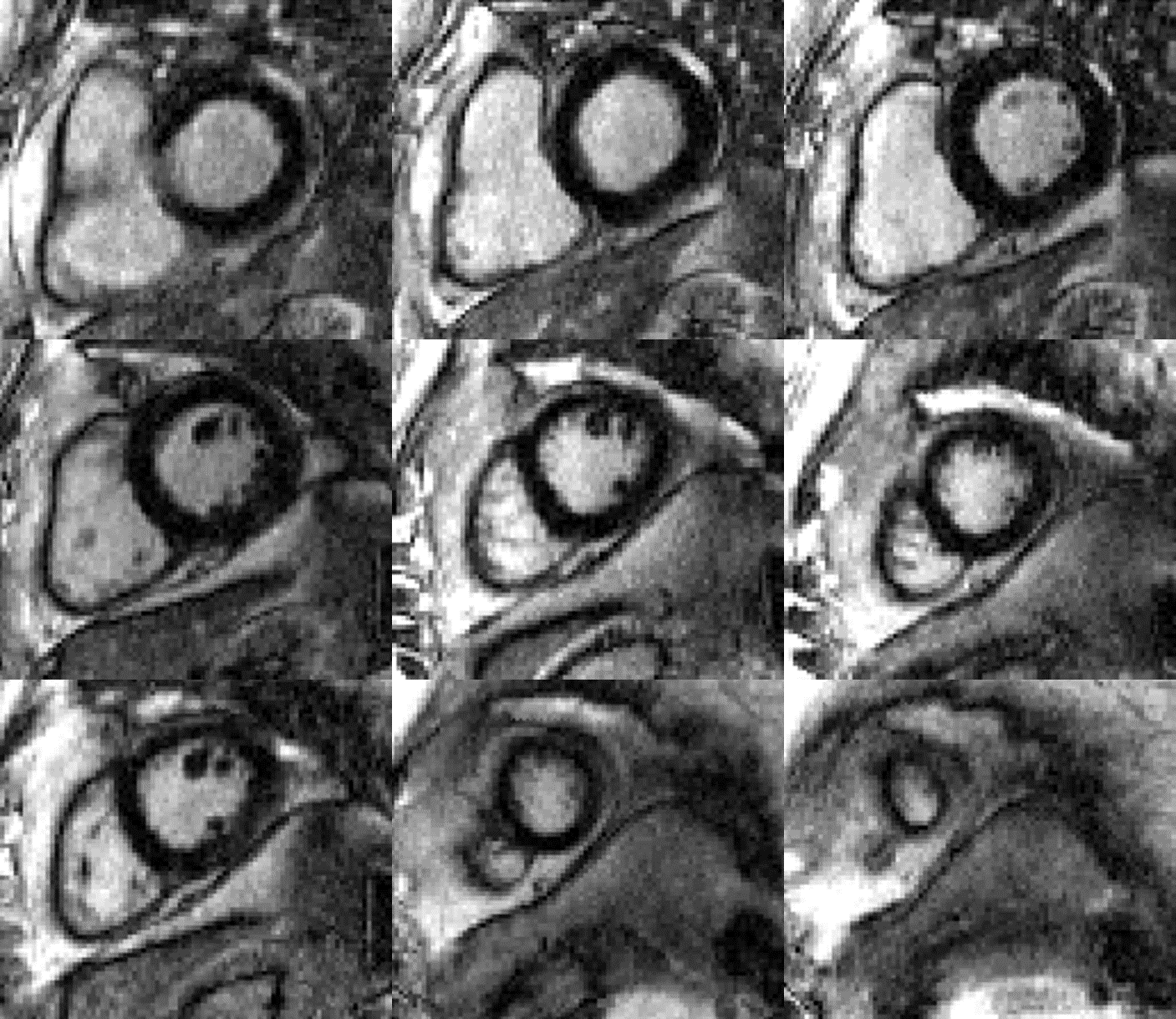
Examples of images acquired using the proposed and the reference method are shown in Figure 2. Similar visual quality was observed between both techniques. The quantified sharpness of both methods was comparable: 0.37±0.07mm-1 for the reference method vs 0.36±0.08mm-1 for the proposed approach. An example of full LV coverage in one subject, acquired with 4 breathhold acquisitions of the proposed LGE sequence is shown in Figure 3.Discussion
The proposed LGE sequence is a promising option for the accelerated acquisition of LGE images. For full LV coverage of 12 slices, 12 breathholds would be required in the conventional method, while 4 breathholds would suffice with the proposed approach. Assessment of this technique in a larger patient cohort, including patients with myocardial scar, is now warranted.Conclusion
SMS-bSSFP CS was successfully used to acquire LGE images through the use of highly undersampled multiple single-shot dynamic acquisitions in one breathhold. The proposed approach enables acquisition of 3 LGE slices in one breathhold, providing a 3 times acceleration over the standard LGE technique and no impact on myocardial sharpness.Acknowledgements
This work was supported by the Engineering and Physical Sciences Research Council (EPSRC) grant (EP/R010935/1), the British Heart Foundation (BHF) (PG/19/11/34243), the Wellcome EPSRC Centre for Medical Engineering at King’s College London (WT 203148/Z/16/Z), the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ National Health Service (NHS) Foundation Trust and King’s College London, and Siemens Healthineers. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.References
1. Kim HW, Farzaneh-Far A, Kim RJ. Cardiovascular Magnetic Resonance in Patients With Myocardial Infarction. Current and Emerging Applications. J. Am. Coll. Cardiol. 2009;55:1–16 doi: 10.1016/j.jacc.2009.06.059.
2. Kramer CM, Barkhausen J, Bucciarelli-Ducci C, Flamm SD, Kim RJ, Nagel E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J. Cardiovasc. Magn. Reson. 2020;22:1–18 doi: 10.1186/s12968-020-00607-1.
3. McElroy S, Ferrazzi G, Nazir MS, et al. Combined simultaneous multislice bSSFP and compressed sensing for first‐pass myocardial perfusion at 1.5 T with high spatial resolution and coverage. Magn. Reson. Med. 2020;84:3103–3116 doi: 10.1002/mrm.28345.
4. Ferrazzi G, McElroy S, Neji R, et al. First-pass multi-contrast and multi-phase myocardial perfusion using simultaneous multi-slice imaging. In: 23rd Annual Meeting of SCMR. ; 2020. pp. 429–431.
5. Stäb D, Ritter CO, Breuer FA, Weng AM, Hahn D, Köstler H. CAIPIRINHA accelerated SSFP imaging. Magn. Reson. Med. 2011 doi: 10.1002/mrm.22600.
6. Stäb D, Speier P. Gradient-controlled local Larmor adjustment (GC-LOLA) for simultaneous multislice bSSFP imaging with improved banding behavior. Magn. Reson. Med. 2019;81:129–139 doi: 10.1002/mrm.27356.
7. Liu J, Lefebvre A, Zenge MO, Schmidt M, Mueller E, Nadar MS. 2D bSSFP real-time cardiac CINE-MRI: compressed sensing featuring weighted redundant Haar Wavelet regularization in space and time. J. Cardiovasc. Magn. Reson. 2013 doi: 10.1186/1532-429x-15-s1-p49.
8. Larson AC, Kellman P, Arai A, et al. Preliminary investigation of respiratory self-gating for free-breathing segmented cine MRI. Magn. Reson. Med. 2005;53:159–168 doi: 10.1002/mrm.20331.
Figures