0961
2D Cardiac MR T1 Cine Multitasking: Initial Clinical Experience1Department of Radiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China, 2UIH America, Inc., Houston, TX, United States, 3United Imaging Healthcare, Shanghai, China
Synopsis
Here we report our initial clinical experience using a prototype 2D cardiac MR T1 cine multitasking technique with inline reconstruction on a clinical scanner without breath-hold and ECG triggering. Its results were compared with routine clinical cardiac MR techniques in assessing lesions in a patient group.
Introduction
Cardiac Magnetic Resonance (CMR) is a non-invasive imaging technique and has been considered the gold standard with an extensive and growing evidence for the assessment of cardiac structure and function [1-2]. Clinical CMR includes multiple scans such as morphology, function, perfusion, delayed enhancement and parametric maps to provide comprehensive cardiac evaluation. Compared to MRI of other anatomies, CMR scans are usually complicated and time-consuming. Its wide use is further hampered by the need for repeated breath-hold, susceptibility to poor ECG triggering signal, and the requirement for substantial expertise from technologists and radiologists. Multitasking is an emerging technique that can resolve multiple ‘tasks’ at the same time [3-6] while using small amount of data. In its CMR application, multitasking has achieved high spatial resolution cardiac-phase-resolved myocardial T1 mapping, without breath-hold and ECG. Here we present our initial experience in evaluating a prototype 2D CMR T1 cine multitasking sequence with inline reconstruction on a clinical MR scanner on patients with heart diseases.Methods
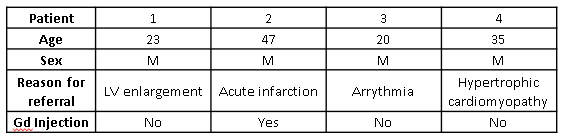
Sequence and reconstruction: A prototype 2D T1 cine multitasking sequence was developed following a previous application [3]. Imaging parameters were: FOV=270mm*270mm, matrix=160*160, slice thickness = 8mm, flip angle =5°, TE/TR=1.7/3.6ms, bandwidth=850Hz/pixel. A total of 24 inversion recovery modules were used with 806 radial spokes following each inversion recovery module and the scan time was 70 s. Inline reconstruction was performed on a standard clinical MR reconstruction console equipped with two 2.10GHz Xeon CPUs and 96G memory and typical reconstruction time was 5-6 min. Output of the prototype application include respiratory-motion-resolved image series, cardiac-motion-resolved image series, inversion recovery image series, and T1 cine maps.Study experiment: All data were acquired on a clinical 3T scanner (uMR780, United Imaging Healthcare, Shanghai, China). A total of 4 patients (Table 1) who were referred for CMR due to clinical findings were enrolled prospectively after IRB consent. One of the patients received single-dose Gd contrast injection. The following scans were performed for all patients: multitasking, dark-blood morphology with fast spin-echo (FSE), cine with balanced stead-state free procession (bSSFP), and T1 mapping with modified look-locker inversion recovery (MOLLI). For patients receiving contrast, phase-sensitive inversion recovery (PSIR) was performed after injection following clinical protocol, and three multitasking scans were performed before, 5 mins and 10 mins after injection, respectively. Multitasking images were then compared with respective routine scan images for lesion identifications.
Results
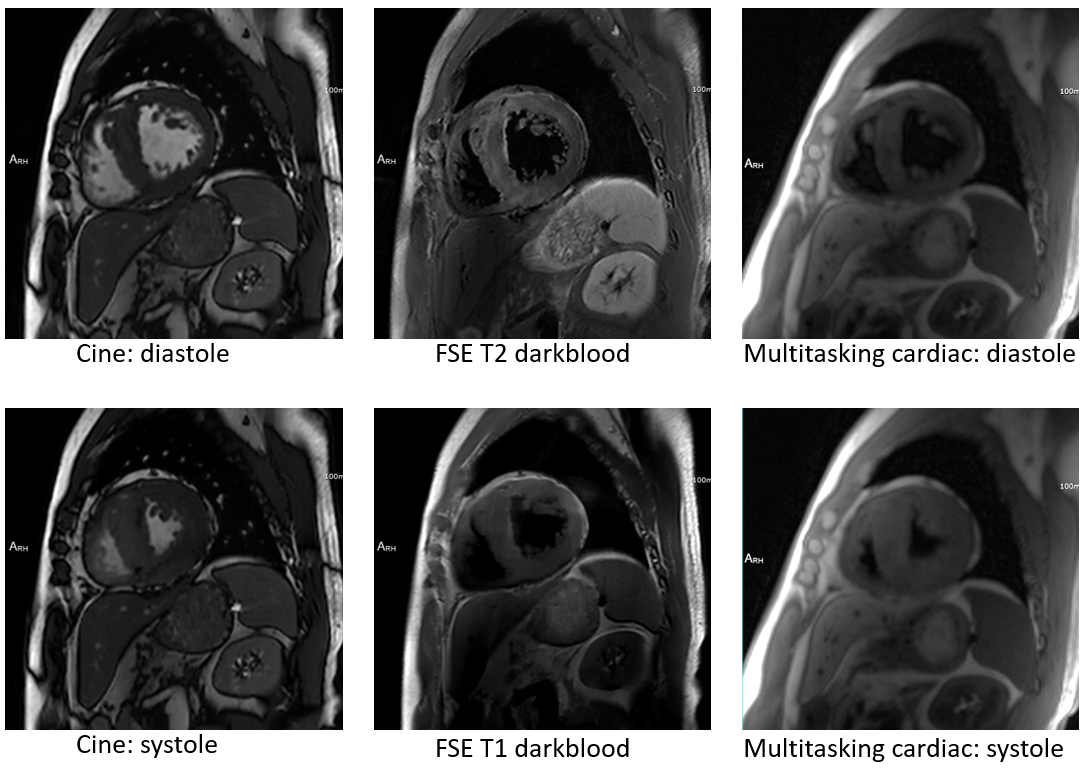
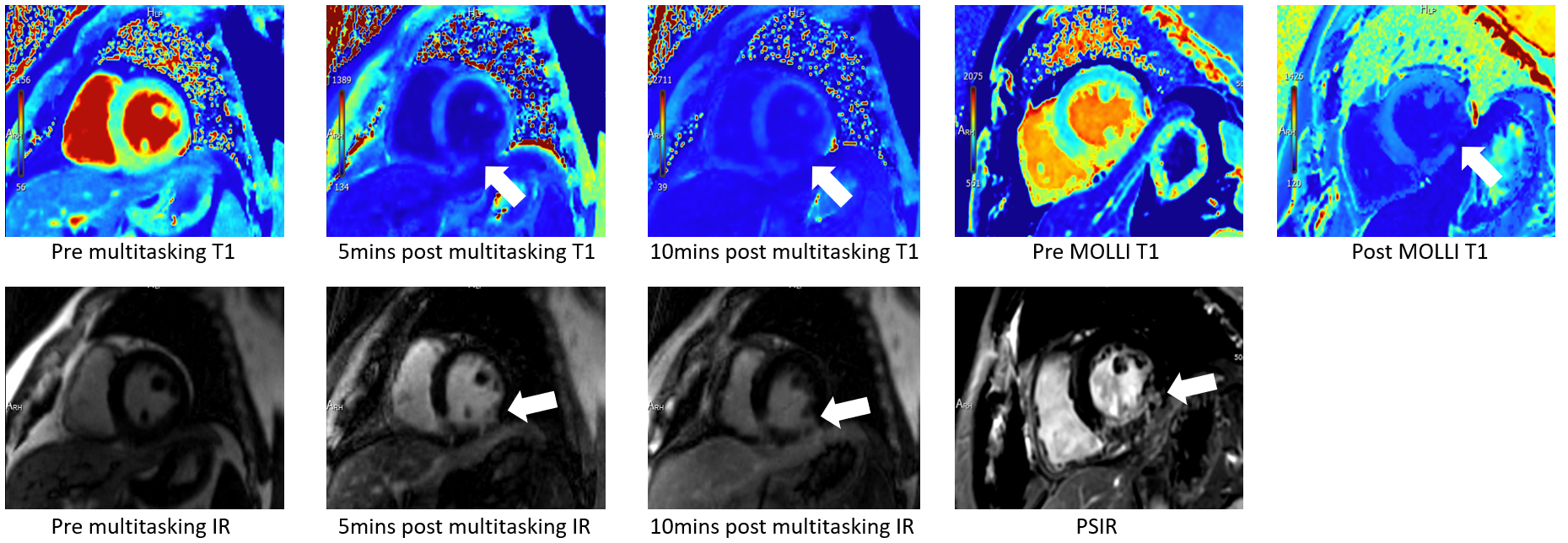
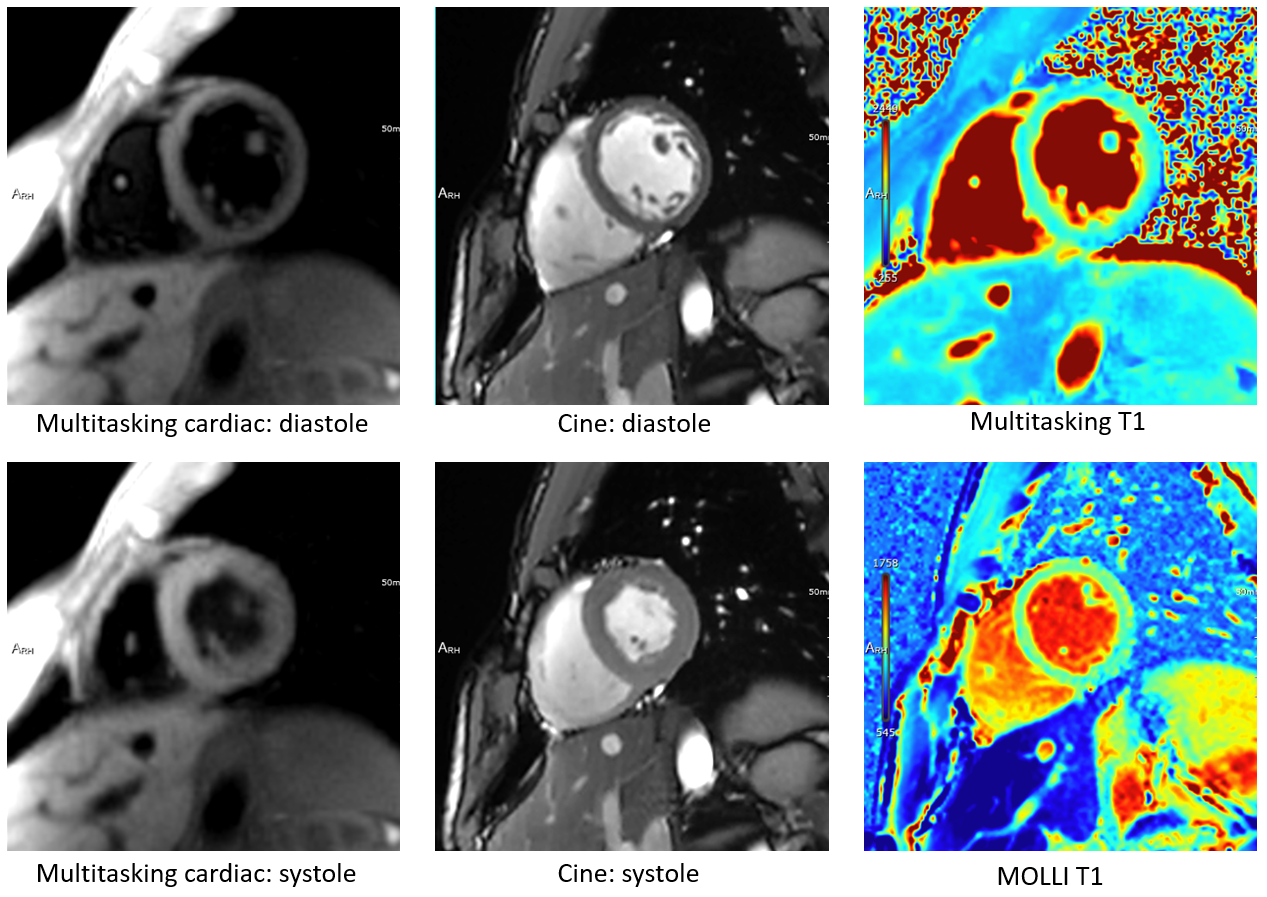
Images of a patient with hypertrophic cardiomyopathy are shown in Figure 1, in which multitasking images are of comparable quality to the cine images and dark blood FSE images in visualizing thickened ventricular wall. Images of a patient with acute infarction are shown in Figure 2, in which the infarct manifests as slightly increased T1 before, and decreased T1 after Gd injection, on both MOLLI and multitasking T1 maps. Meanwhile, by choosing appropriate inversion time to null the normal healthy myocardium, multitasking IR imaging can produce images with similar contrast to PSIR and the lesion region can be clearly identified on both multitasking IR images and PSIR image. Images of a patient with arrhythmia are shown in Figure 3, in which multitasking can produce cardiac-motion resolve images and T1 maps of good quality despite presence of arrhythmia.Conclusion and Discussion
We evaluated the feasibility of a prototype 2D CMR T1 cine multitasking application on a small patient group on a clinical MR scanner with inline reconstruction and the images showed good agreement with respective routine techniques. In our initial experience, multitasking has the potential to replace certain sequences within routine cardiac protocols such as dark blood, cine, pre and post T1 mapping/ECV, and LGE, and thus reduce scan time and simplify the CMR workflow. In addition, because there is no breath-hold or ECG triggering needed, this can further facilitate clinical workflow by reducing repeated scan and broaden scans onto patients that are otherwise challenging for CMR, such as those with arrhythmia. Although the current reconstruction time of 5-6 min was faster than previously reported, further improvements in speed is warranted before it can be largely used in a clinical setting. Further evaluation on image quality and quantification results in a larger cohort is needed.Acknowledgements
This work was partially facilitated by a non-exclusive license agreement between Cedars-Sinai Medical Center and United Imaging Healthcare.References
[1] Hundley WG, Bluemke, DA, Finn, JP, et al. ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. Circulation 2010, 121(22), 2462–2508.
[2] Heckbert SR, Post W, Pearson GD, et al. Traditional cardiovascular risk factors in relation to left ventricular mass, volume, and systolic function by cardiac magnetic resonance imaging: The Multiethnic Study of Atherosclerosis. J Am Coll Cardiol 2006;48(11):2285-92.
[3] Shaw JL, Yang Q, Zhou Z, Deng Z, Nguyen C, Li D, Christodoulou AG. Free-breathing, non-ECG, continuous myocardial T1 mapping with cardiovascular magnetic resonance multitasking. Magn Reson Med. 2019 Apr;81(4):2450-2463.
[4] Christodoulou, A.G., Shaw, J.L., Nguyen, C. et al. Magnetic resonance multitasking for motion-resolved quantitative cardiovascular imaging. Nat Biomed Eng 2, 215–226 (2018).
[5] Wang N, Christodoulou AG, Xie Y, Wang Z, Deng Z, Zhou B, Lee S, Fan Z, Chang H, Yu W, Li D. Quantitative 3D dynamic contrast-enhanced (DCE) MR imaging of carotid vessel wall by fast T1 mapping using Multitasking. Magn Reson Med. 2019 Apr;81(4):2302-2314.
[6] Wang N, Gaddam S, Wang L, Xie Y, Fan Z, Yang W, Tuli R, Lo S, Hendifar A, Pandol S, Christodoulou AG, Li D. Six-dimensional quantitative DCE MR Multitasking of the entire abdomen: Method and application to pancreatic ductal adenocarcinoma. Magn Reson Med. 2020 Aug;84(2):928-948
Figures