0944
Improved gastric T2WI imaging by an TSE corrected HASTE sequence: a comparation study with conventional HASTE, TSE and BLADE-TSE sequences on 3T1The Fourth Hospital of Hebei Medical University, Shijiazhuang, China, 2MR Scientific Marketing,Siemens Healthcare, Beijing, China, 3MR Scientific Marketing,Siemens Healthcare, JINAN, China, 4The Fourth Hospital of Hebei Medical University, shijiazhuang, China
Synopsis
In this study, we evaluated the scan time and image quality of a serious of gastric T2WI imaging, including conventional TSE with cartesian acquisition (TSE), BLADE-TSE, conventional HASTE sequence and a new TSE corrected HASTE sequence (TSE-HASTE). We found that the HASTE sequences can provide comparable image quality to TSE sequences, while is insensitive to motion and susceptibility artifacts. For patients with poor respiratory movement, HASTE sequence may be used as a good replacement to the TSE sequences, and TSE-HASTE sequence may provide a better image contrast compared to conventional HASTE.
Objective
To optimize gastric T2WI imaging, we evaluated the image contrast, motion artifacts and scan time of the following four sequences: conventional turbo spin-echo (TSE) with Cartesian K-space coding scheme, BLADE-TSE, conventional half-Fourier acquisition single-shot turbo spin-echo (HASTE) sequence and a newly developed HASTE sequence corrected by a TSE reference scan (TSE-HASTE), which provide better tissue contrast than conventional HASTE.Methods
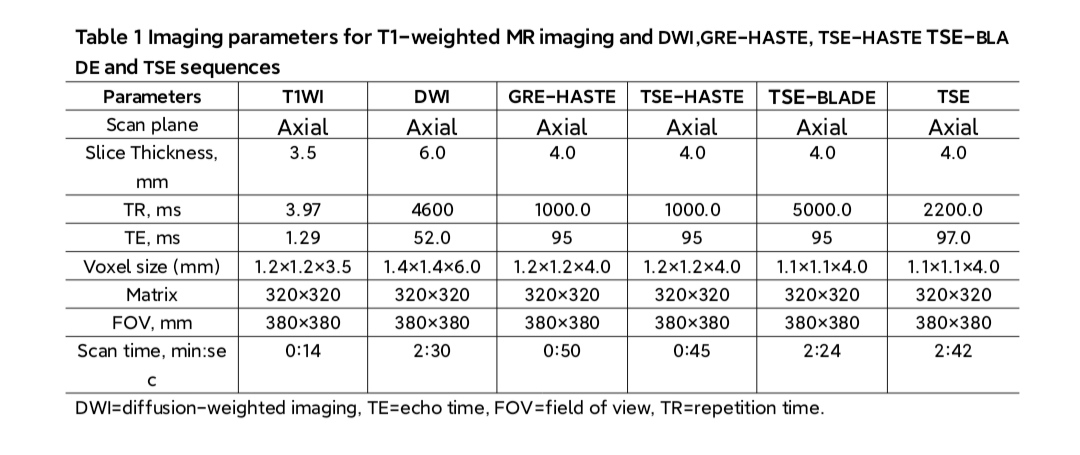
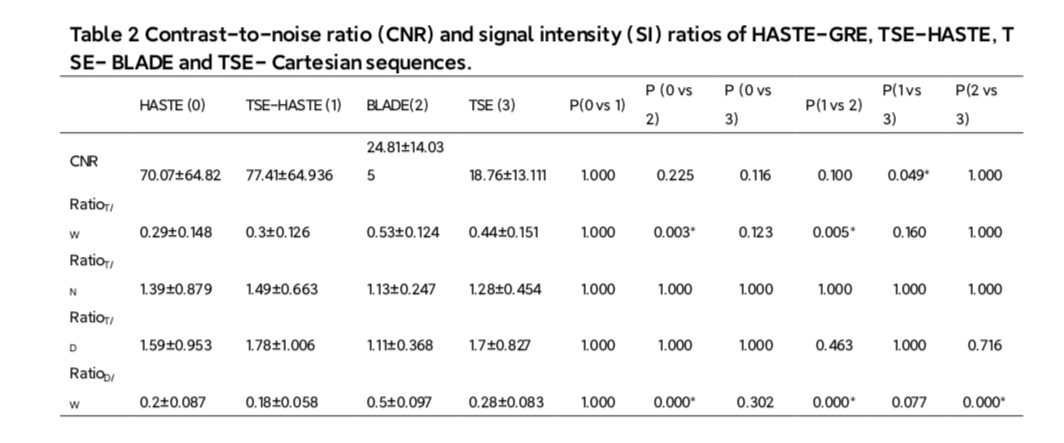
From October 2020 to December 2020, twenty-five patients (17 males, 8 females, mean age 62±3.52) with gastric cancer underwent gastric MRI scanning with the TSE, BLADE-TSE, conventional HASTE and TSE-HASTE sequences at a 3T MR scanner (MAGNETOM Vida, Siemens Healthcare, Erlangen, Germany), and the imaging parameters are listed in table 1. Blind to sequence type, two radiologists (5 and 8 years’ experiences in interpreting gastric cancers) independently evaluated the image quality of these images on the basis of a 5-point scale {subjective scoring:5= excellent (no problems were noticed in the image and the gastric cancer was clearly shown), 4 =good (the image suffered from only minor degradation and was suitable for the evaluation of the cancer), 3=moderate (image quality was not good but usable for the evaluation of the cancer), 2 = poor (image quality is seriously affected by artifacts,and is barely used for diagnosis ) and 1 = unacceptable (image quality precluded assessment of the cancer and the pancreas was barely shown)}. In order to quantitatively evaluate the performance of these sequences in diagnosing gastric cancer, the signal intensity (SI) of cancer, adjacent gastric wall, distant gastric wall and water in gastric cavity were measured respectively. The contrast-to-noise ratio (CNR) between cancer and adjacent gastric wall (RatioC/N), cancer and distant gastric wall (RatioC/D), cancer and water (RatioC/W), distant gastric wall and water (RatioD/W) were calculated. All the quantitative and qualitative parameters were analyzed with one-way ANOVA and Kruskal-Wallis 1-way ANOVA methods. One-way ANOVA was applied for group comparison with Bonferroni correction.Results
The subjective evaluation score of conventional HASTE and TSE-HASTE sequences were significantly higher than BLADE- TSE and conventional TSE sequence [(4.8±0.422) and (4.9±0.316) vs (2.6±0.966) and (2.3±1.059), P<0.001]. The images of TSE-HASTE sequence demonstrated highest scores than any other sequences. For the analysis of quantitative parameters, the CNRs of HASTE sequence are higher than TSE sequence. All images acquired with both sequences are adequate for diagnosis. No significant difference was observed in SI between conventional HASTE and TSE-HASTE sequence, but TSE-HASTE sequence showed slightly higher tissue CNRs .Discussion
The TSE T2WI sequence with respiratory gating technique can greatly reduce the influence of respiratory movements of stomach [1]. However, the application of respiratory gated TSE sequences is limited, as the patient’s breathing rhythm and respiratory rate cannot always be consistent. HASTE imaging provides rapid gastric image with less motion artifacts, but may naturally suffers from image blurring of the organs along the phase-encoding direction[2]. Recently, a newly developed TSE corrected HASTE sequence may improve image contrast as compared to conventional HASTE, which may potentially improve the cancer diagnosis.Conclusions
Although the SI of HASTE sequence is not better than that of TSE sequence, the HASTE sequence demonstrate good performance in gastric cancer diagnosis with much less motion artifacts and fast acquisition, which may help patients with poor respiratory curve or cannot hold breath.Acknowledgements
No acknowledgement found.References
[1] Bayramoglu S, Kilickesmez O, Cimilli T, Kayhan A, Yirik G, Islim F, Alibek S. T2-weighted MRI of the upper abdomen: comparison of four fat-suppressed T2-weighted sequences including PROPELLER (BLADE) technique. Acad Radiol. 2010 Mar;17(3):368-74. doi: 10.1016/j.acra.2009.10.015. Epub 2009 Dec 30. PMID: 20042352. [2] Kim AY, Han JK, Kim TK, Park SJ, Choi BI. MR imaging of advanced gastric cancer: comparison of various MR pulse sequences using water and gadopentetate dimeglumine as oral contrast agents. Abdom Imaging. 2000 Jan-Feb;25(1):7-13. doi: 10.1007/s002619910002. PMID: 10652914.Figures
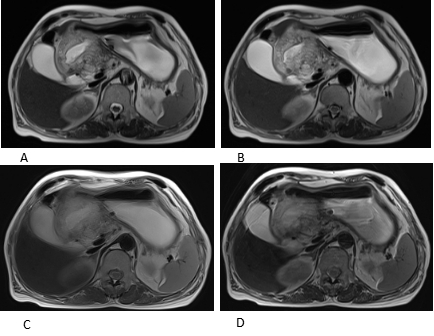
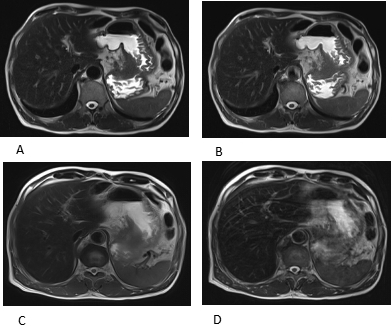
Fig 1, male, 56 years old with gastric cancer, (A) image acquired by TSE-HASTE with a subjective score of 5 points; (B) image acquired by conventional HASTE sequence sequence with a subjective score of 5 points; (C) image acquired by TSE- BLADE sequence with a subjective score of 3 points; (D) image acquired by conventional TSE sequence with a subjective score of 3 points.