0838
Rapid T2-DIADEM Echo-Planar Imaging as an Alternative to T2-FSE: A Clinical Feasibility Study1Department of Radiology, Mayo Clinic, Rochester, MN, United States, 2A. A. Martinos Center for Biomedical Imaging, Department of Radiology, Massachusetts General Hospital, Charlestown, MA, United States, 3Department of Electrical Engineering and Computer Science, MIT, Cambridge, MA, United States, 4Department of Radiology, Stanford University, Stanford, CA, United States, 5Stanford University, Stanford, CA, United States, 6Department of Radiologic Technology, Faculty of Associated Medical Sciences, Chiang Mai University, Chiang Mai, Thailand
Synopsis
Rapid high-resolution echo-planar-imaging (EPI) with improved image quality could conceivably be utilized as a high-speed alternative to conventional T2-weighted fast-spin-echo imaging (T2-FSE). A variant of multi-shot EPI, DIADEM (distortion-free imaging: a double encoding method), was recently described (5) and shown to yield high quality, high resolution images free of spatial distortion. In this work, a T2-weighted DIADEM pulse sequence was optimized with self-calibrated, tilted-CAIPI reconstruction scheme and then comparatively evaluated to T2-FSE images of the brain in 24 human subjects by two neuroradiologists.
Introduction
Rapid (sub-minute) high-resolution echo-planar-imaging (EPI) with improved image quality is a potential high-speed alternative to conventional MR image such as fast- or turbo-spin-echo (FSE or TSE) sequence. Previous studies demonstrated that high-resolution EPI with reduced spatial distortion could be achieved with the benefits of high-performance gradients (700 T/m/s, 200 mT/m) on a compact 3T MRI1,2 and the image quality was further improved with multi-shot acquisition.3 However, there was still noticeable distortion in very high in-plane resolution (<1mm2) imaging even with a 4-shot acquisition.3 Recently, a novel variant of multi-shot EPI, termed DIADEM (distortion-free imaging: a double encoding method)4,5, was described to resolve the spatial distortion issue. Scan time was accelerated with the tilted-CAIPI (tCAIPI) reconstruction scheme.6 To adopt this approach as an alternative to T2-FSE, self-calibrated tCAIPI scheme avoiding additional calibration scan (~20 s) is proposed in this study. The clinical feasibility was evaluated in a pilot comparison study with radiological review of 24 subjects.Methods
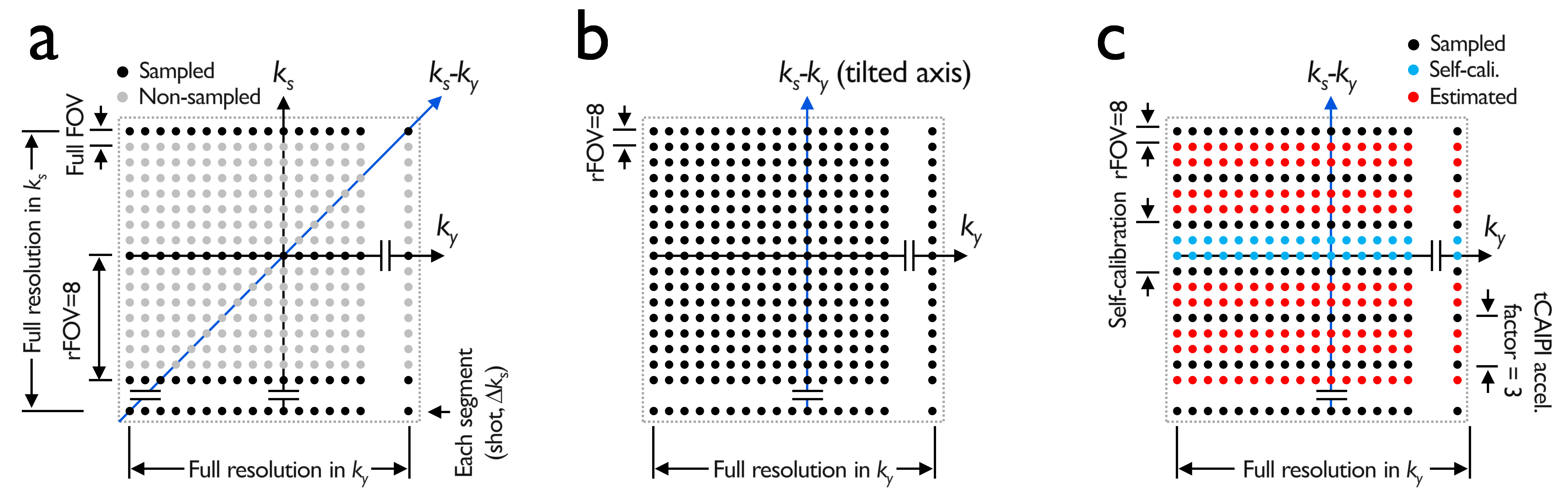
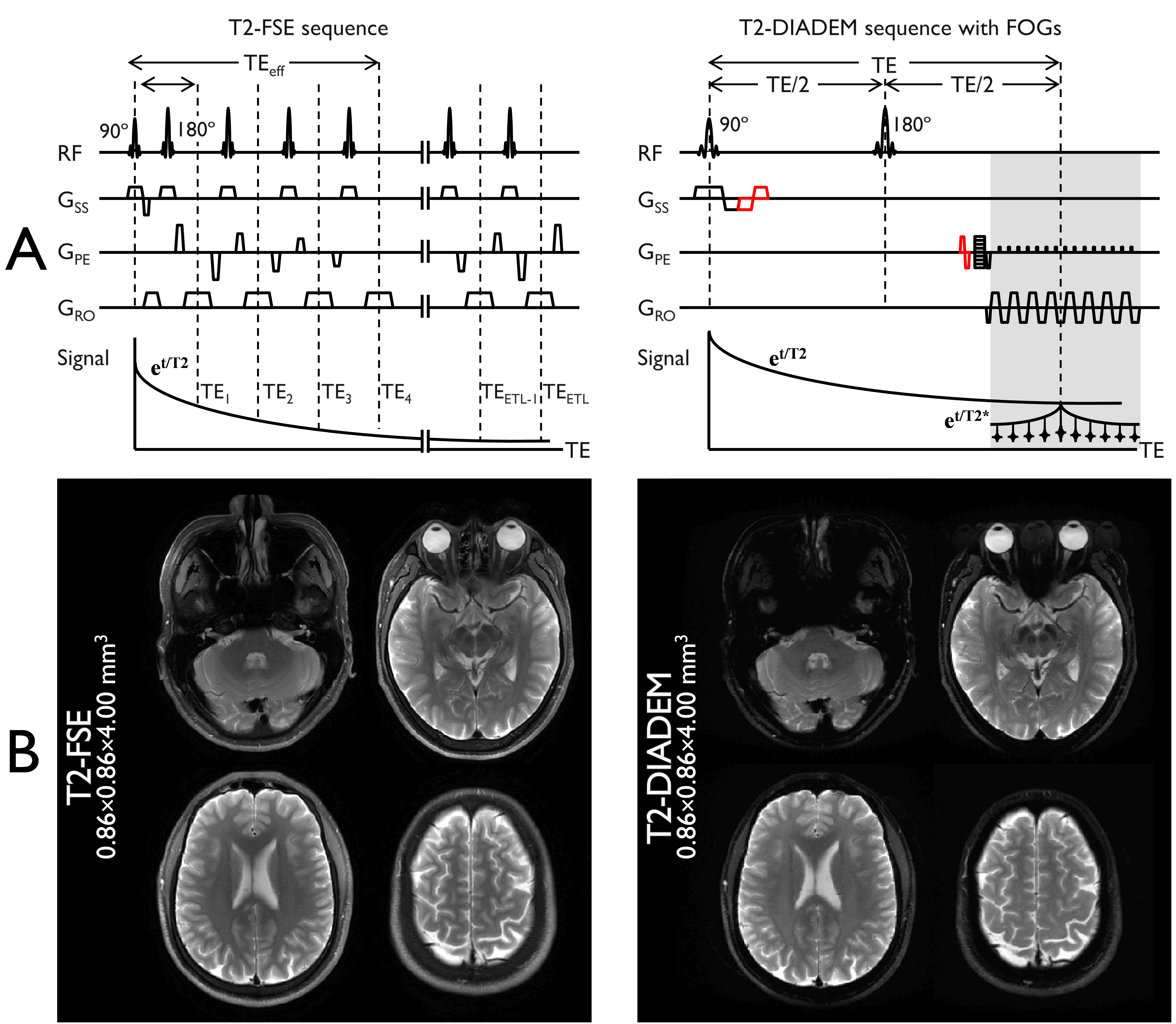
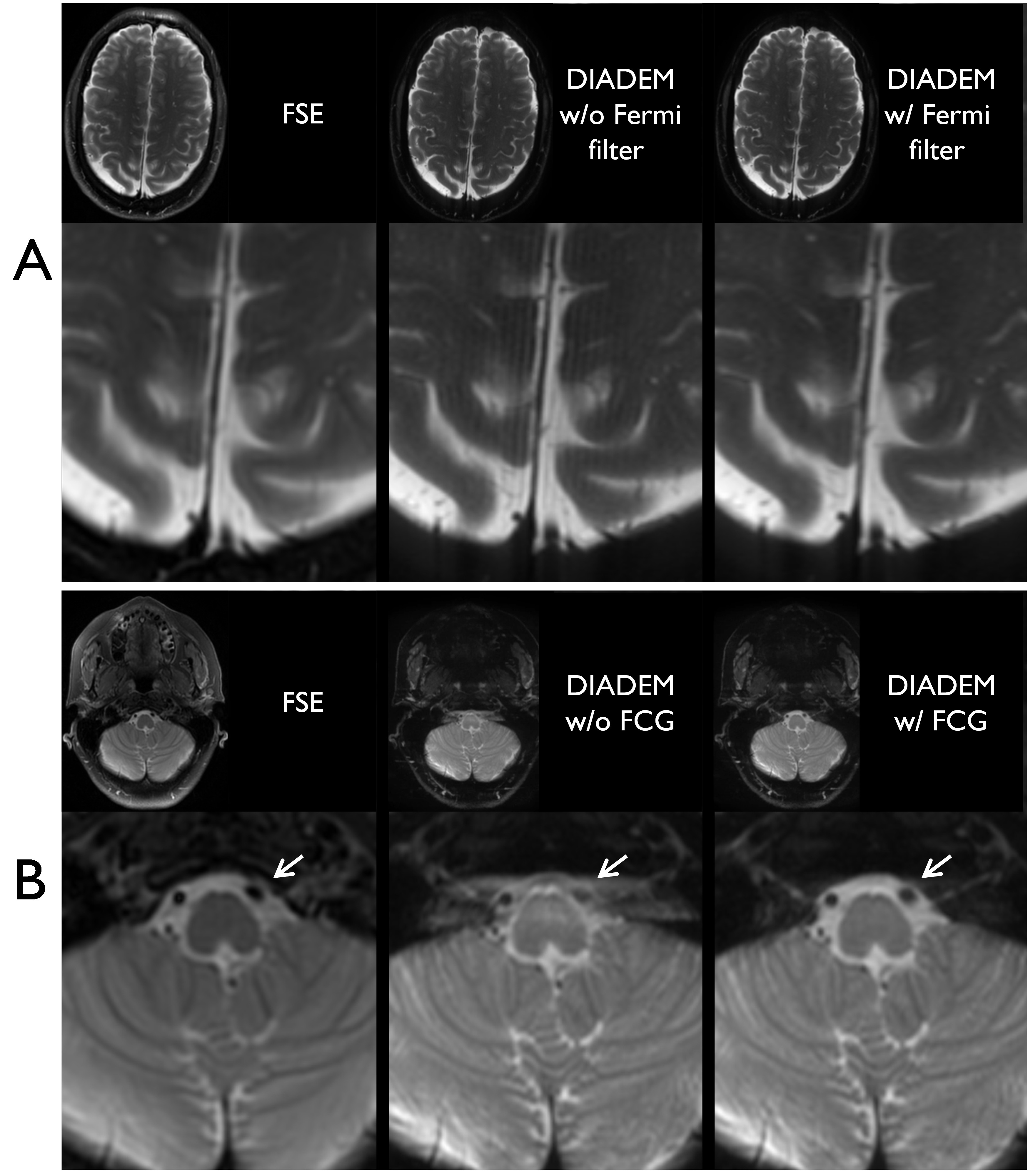
All experiments were conducted on the compact 3T scanner2,7,8 using a 32-channel head coil (Nova Medical, USA). Self-calibrated tCAIPI acquisition and reconstruction in DIADEM: Undistorted images without wrap-around artifact could be calculated from the DIADEM data even with a reduced field of view (rFOV) factor of 8, leading to a 32-shot acquisition for a 256x256 matrix size on the compact 3T with high-performance gradients3 that enabled a reduction in an effective echo-spacing of up to 209.3 ms (Fig. 1A). After considering this as the “full” acquisition (Fig. 1B), a further undersampling factor of 3 was applied with self-calibration (i.e., 2 additional shots at the k-space center in the spin-warp phase-encoding (SW-PE) dimension along with 7/8 partial Fourier, which resulted in an 11-shot accelerated acquisition (i.e., 32/3×7/8+2). Without additional 3D calibration data acquisition as suggested in previous studies, a 2D tilted-CAIPI reconstruction was applied along the tilted (i.e. ky-ks) axis with self-calibration included in the DIADEM acquisition (Fig. 1C). Radiological evaluation of T2-DIADEM relative to T2-FSE: After written consent and under an IRB-approved protocol, a pilot study of 24 subjects were scanned with standard clinical T2-FSE and proposed T2-DIADEM protocols at equivalent spatial resolution (0.86×0.86×4 mm3) and imaging matrix size (256×256×38). The acquisition times were 55 seconds and 1 minute 58 seconds, respectively. Those exams were reviewed by two board-certified neuroradiologists. Further artifact reduction: In radiological review of the pilot data, Gibbs ringing artifacts were observed along the readout direction with DIADEM. To address this issue, a 1D Fermi filter was applied in k-space along the corresponding dimension. In addition, pulsation-induced flow effects caused phase shifts that vary between shots in DIADEM acquisition and resulted in ghost artifacts along the PE direction of the undistorted image. To reduce this artifact, flow compensation gradients (FCG) designed to null the velocity-dependent phase shifts were implemented into the DIADEM sequence (Fig. 2A). The reduction was confirmed by DIADEM scans with and without the FCG from additional three-subject exams.Results and Discussion
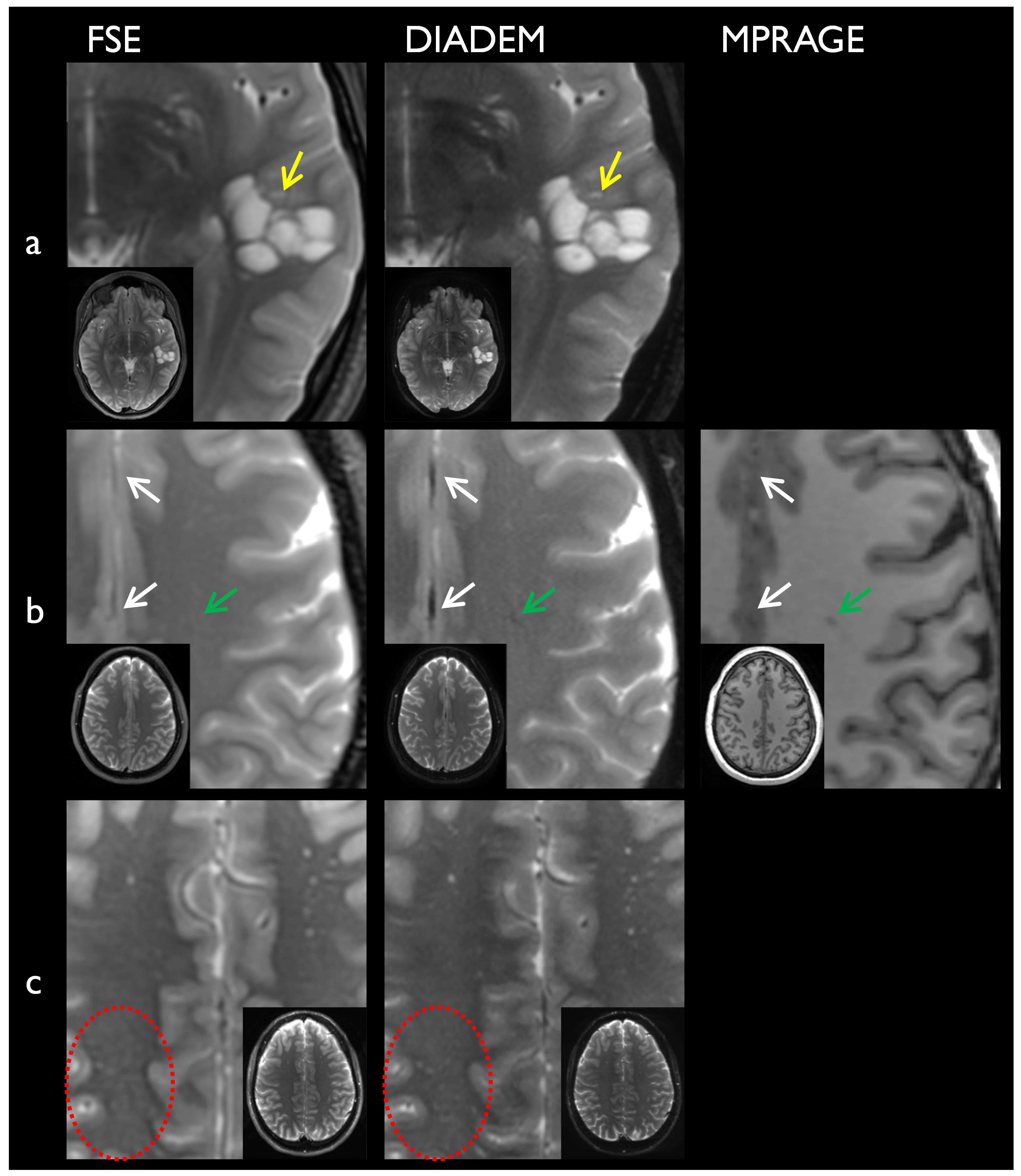
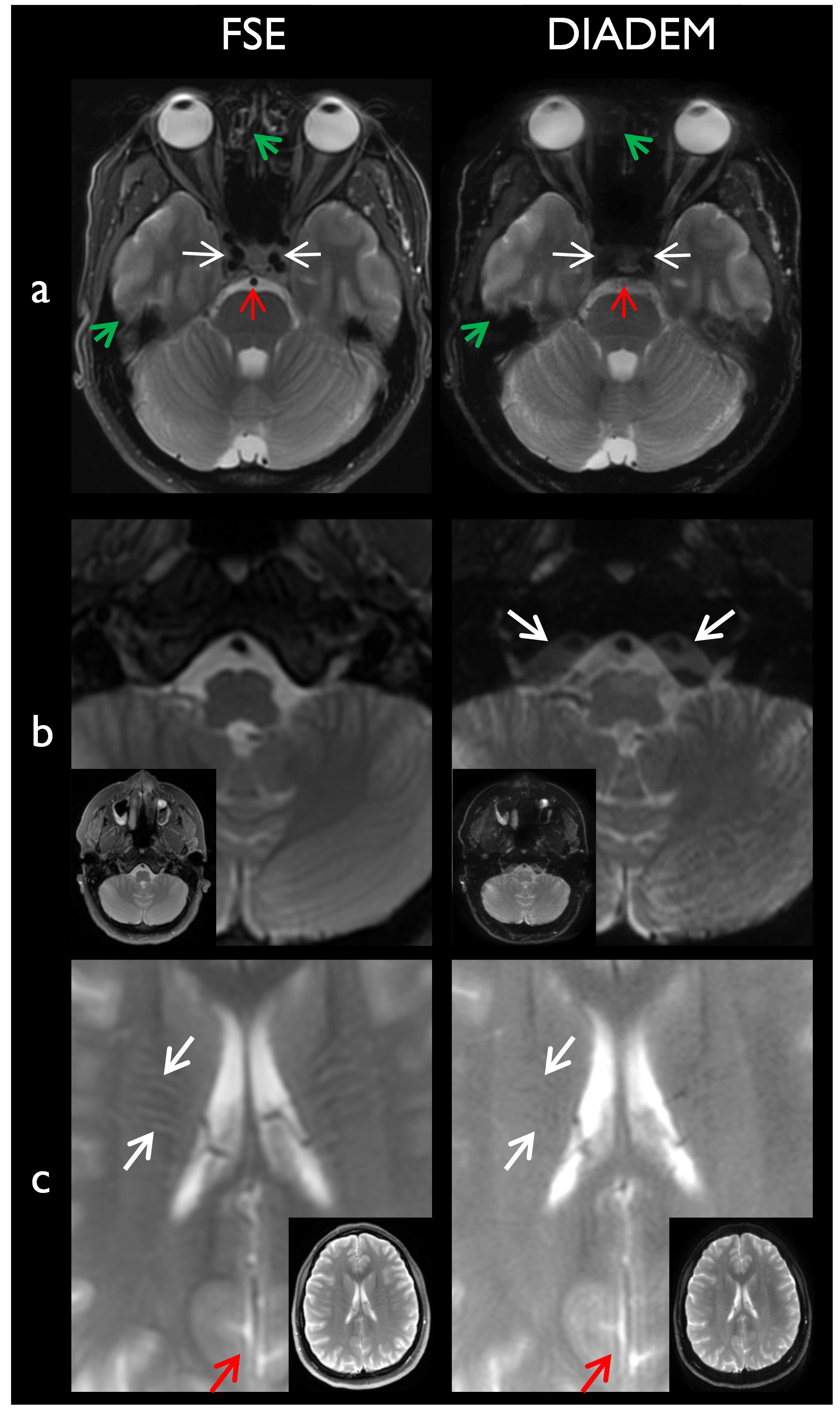
The acquisition time for the DIADEM is faster by a factor of 2.14 compared to the standard FSE acquisition. Despite this considerable acceleration, the spatial resolution and contrast were not compromised (Fig. 2B). Without any additional 3D calibration scan for 3D tilted-CAIPI reconstruction, in addition, the 2D tilted-CAIPI reconstruction was able to successfully unfold the DIADEM data only with four calibration lines (i.e. shots) at the k-space center in the SW-PE dimension (Fig. 1C). In radiological review, T2-DIADEM demonstrated better apparent spatial resolution relative to FSE, despite an equivalent acquisition matrix. This may be because the longer echo train length (i.e. 11) filling different k-space lines in FSE (Fig. 2A) causes more apparent T2 blurring. Due to stronger T2* weighting over the long readout acquisition window in DIADEM (Fig. 2A), T2-DIADEM provided superior depiction of iron-containing structures, e.g. in regions of globus pallidus, dentate nucleus, red nucleus, substantia nigra, and chronic microhemorrhage (Fig. 2B). While the strong T2* weighting was helpful to better identify small developmental venous anomaly and the multiple small T2 hyperintense perivascular spaces (Fig. 3), it also resulted in strong signal dropouts in the skull base (Fig. 4a). Due to its multi-shot nature of the DIADEM, in addition, greater CSF flow/pulsation artifacts were observed around the brainstem and within the ventricles, which made it difficult to evaluate flow void from basilar artery and cavernous internal carotid arteries on T2-DIADEM (Fig. 4). Interestingly, reduced gray-white matter contrast was shown only in periventricular regions on T2-DIADEM (Fig. 4c). With the radiologist’s feedback, Gibbs ringing and flow artifacts were additionally minimized with 1D Fermi filter and FCGs, respectively (Fig. 5). The overall radiologist impression was that the 55 second DIADEM acquisition would be a suitable alternative to T2-FSE in a rapid brain assessment protocol (e.g., for an uncooperative patient).Conclusion
Overall, T2-DIADEM performed well relative to T2-FSE in the 24 subjects evaluated. While DIADEM offers some advantages over FSE, it is still not a complete replacement for T2-FSE. In the current form, it would be most appropriate for use in a rapid brain assessment protocol. Further work is continuing to improve T2-DIADEM signal dropout and image artifacts.Acknowledgements
This work was supported by NIH U01 EB024450. The authors would like to thank Jennifer Myers and Erin Gray for their help in collecting the data.References
1. Tan ET, Lee SK, Weavers PT, Graziani D, Piel JE, Shu Y, Huston J, Bernstein MA, Foo TK. High slew‐rate head‐only gradient for improving distortion in echo planar imaging: Preliminary experience. Journal of Magnetic Resonance Imaging 2016;44(3):653-664.
2. Lee SK, Mathieu JB, Graziani D, Piel J, Budesheim E, Fiveland E, Hardy CJ, Tan ET, Amm B, Foo TKF. Peripheral nerve stimulation characteristics of an asymmetric head‐only gradient coil compatible with a high‐channel‐count receiver array. Magnetic resonance in medicine 2016;76(6):1939-1950.
3. Tan ET, Weavers PT, Gray EM, Hardy CJ, Schenck JF, Bernstein MA, Shu Y, Foo TK, Huston J. ISMRM 2017:p.234.
4. In MH, Posnansky O, Speck O. High-resolution distortion-free diffusion imaging using hybrid spin-warp and echo-planar PSF-encoding approach. NeuroImage 2017;148:20-30.
5. In MH, Tan ET, Trzasko JD, Shu Y, Kang D, Yarach U, Tao S, Gray EM, Huston III J, Bernstein MA. Distortion‐free imaging: A double encoding method (DIADEM) combined with multiband imaging for rapid distortion‐free high‐resolution diffusion imaging on a compact 3T with high‐performance gradients. Journal of Magnetic Resonance Imaging 2020;51(1):296-310.
6. Dong Z, Wang F, Reese TG, Manhard MK, Bilgic B, Wald LL, Guo H, Setsompop K. Tilted‐CAIPI for highly accelerated distortion‐free EPI with point spread function (PSF) encoding. Magnetic resonance in medicine 2018.
7. Weavers PT, Shu Y, Tao S, Huston J, Lee SK, Graziani D, Mathieu JB, Trzasko JD, Foo TKF, Bernstein MA. Compact three‐tesla magnetic resonance imager with high‐performance gradients passes ACR image quality and acoustic noise tests. Medical physics 2016;43(3):1259-1264.
8. Foo TKF, Laskaris E, Vermilyea M, Xu M, Thompson P, Conte G, Van Epps C, Immer C, Lee SK, Tan ET, Graziani D, Mathieu JB, Hardy CJ, Schenck JF, Fiveland E, Stautner W, Ricci J, Piel J, Park K, Hua Y, Bai Y, Kagan A, Stanley D, Weavers PT, Gray E, Shu Y, Frick MA, Campeau NG, Trzasko J, Huston J, 3rd, Bernstein MA. Lightweight, compact, and high-performance 3T MR system for imaging the brain and extremities. Magn Reson Med 2018;80(5):2232-2245.
Figures