0836
Faster fetal whole-heart anatomical and blood flow 4D cine MRI with k-t SWEEP1Biomedical Engineering Department, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Division of Pediatric Cardiology, The Hospital for Sick Children, Toronto, ON, Canada, 3Department of Congenital Heart Disease, Evelina Children's Hospital, London, United Kingdom
Synopsis
MRI of the fetal heart is challenging due to fetal motion and its small size. Previously, we have demonstrated a method for simultaneous 4D anatomical and blood flow imaging of the whole fetal heart. However, the acquisition takes at least 14 minutes, which is unfavourable for routine clinical usage. Here, we combine k-t SENSE with SWEEP excitation to acquire a continuous sequence of images through the heart. The removal of dummy pulses due to SWEEP excitation reduces our acquisition time by 17%. We also acquire one-third fewer frames compared to our conventional method, resulting in a 45% faster acquisition time.
Introduction
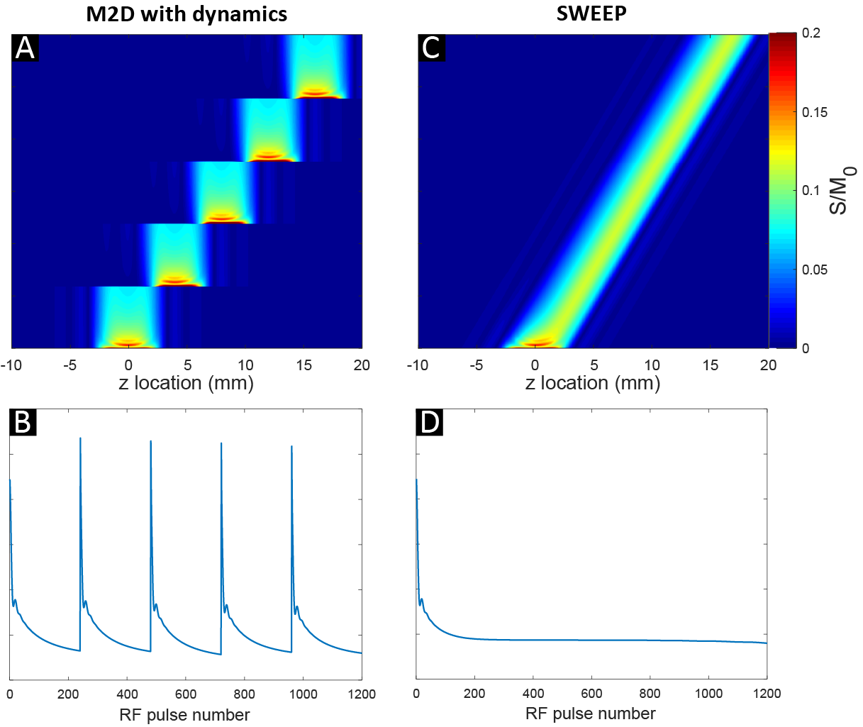
Fetal whole-heart cardiac MRI (CMR) has the potential to become an important complementary adjunct to prenatal ultrasound, particularly in complex cases of congenital heart disease [1]. We have previously shown a motion-corrected method for performing 4D anatomical [2] and blood flow [3] MRI in the fetal heart using k-t SENSE imaging [4] and slice-to-volume registration [5]. Our existing implementation [3] takes at least 14 minutes for data acquisition, which is impractical for routine clinical usage.Here, we combine k-t SENSE with a balanced steady-state free precession (bSSFP) SWEEP [6] excitation, which we name k-t SWEEP. A SWEEP excitation is performed by slowly, linearly increasing the centre frequency of the RF excitation pulse. This has the effect of sweeping the slice profile across the field-of-view (FOV) (Fig 1c), as opposed to a traditional multiple 2D (M2D) slice scheme where each excitation pulse within a slice excites the same fixed z-location (Fig 1b). Two advantages of k-t SWEEP over a k-t M2D approach are:
- After a transient period of unstable signal, a stable-state signal is maintained, which saves time by dispensing with dummy RF pulses.
- All acquired frames are spatially and temporally contiguous, which has various benefits: a) flexible data selection (k-t blocks) for reconstructions tailored to heart rate and motion estimation; b) robustness to sudden fetal movements due to adaptable data rejection; c) potential improvement in volumetric reconstruction due to the smoother representation of the FOV.
Methods
Image acquisitionImaging was performed on a 1.5T Philips Ingenia scanner. Three singleton pregnancies (gestational ages 29-32 weeks) were scanned with the k-t SWEEP method. A previous k-t M2D 4D reconstruction (GA 32+3 weeks) was used for comparison. For both k-t M2D and k-t SWEEP acquisitions, multi-planar stacks of 2D bSSFP slices were acquired using the following parameters: TR/TE 3.8/1.9ms, flip angle 60°, 8x k-t SENSE acceleration, field of view 400×304mm, voxel size 2.0×2.0x6.0mm. For the k-t M2D scans, typically 8-12 slices were acquired per stack, with (Ndyn =) 96 frames acquired per slice. For k-t SWEEP, the omission of dummy RF pulses reduced the acquisition time by 17%. The sweep rate (Rs) was 0.05%, which means that the slice profile moves 0.05% of the slice thickness per TR. This sweep rate was equivalent to performing a reduced k-t M2D acquisition with (Ndyn = ) 64 dynamics per slice covering the same FOV.
4D reconstruction
The k-t M2D data was reconstructed using our standard 4D framework [3]. For k-t SWEEP stacks, the contiguous k-space data could be subdivided into k-t blocks of any nominal number of frames for k-t SENSE reconstructions. For our initial approach, k-t SENSE was performed over k-t blocks of 64 frames, with a stride of 32 frames between each k-t block. The motivation for performing overlapping k-t reconstructions was: 1) more heart rate estimates could be calculated for each stack because one x-f space heart rate estimation can be performed per k-t block; 2) x-t image apodization was possible because overlapping k-t blocks led to multiple reconstructions of single z-locations, thus permitting removal of peripheral images from the k-t blocks.
Results
Fig 2 and Fig 3 show movies of k-t M2D and k-t SWEEP data, acquired in two different fetuses. Discrete spatial transitions (‘jumps’) can be observed as the k-t M2D acquisition switches slice locations (see also Fig 4B-C). With k-t SWEEP, the frames are temporally and spatially contiguous which gives a smooth progression through all frames (see also Fig 4F-G). k-t SWEEP reconstructions produced 4D magnitude (Fig 4H) and flow volumes (Fig 5B) which were of comparable quality to standard k-t M2D datasets (Fig 4D and Fig 5A), despite the reduction in acquired frames.Discussion
The proposed k-t SWEEP method enabled multi-stack imaging of the fetal heart without the need for time-consuming dummy scans. This, in combination with our chosen sweep rate, resulted in a 45% faster acquisition than our previous method. So far, we have demonstrated proof-of-principle that k-t SWEEP is compatible with our fetal CMR 4D framework and the quality of the cine volumes is very encouraging. There is much scope for further development. We have yet to determine the maximal sweep rate before 4D reconstruction becomes compromised, so an even faster acquisition may be possible. The continuous k-t data provided by the SWEEP scheme permits highly flexible k-t reconstruction strategies. k-t blocks are highly customisable which should improve reconstruction. Furthermore, k-t SWEEP is fully compatible with the self-calibrated k-t SENSE method we demonstrated last year [7], which will reduce the acquisition time by a further 50% making possible acquisition of whole heart 4D data in under 5 minutes. Altogether, these developments will enable a faster, 4D fetal CMR examination and pave the way for developing a higher resolution acquisition, which will provide more detailed representations of the complex structures and hemodynamics of the developing fetal heart.Acknowledgements
This work was supported by the Wellcome/EPSRC Centre for Medical Engineering [203148/Z/16/Z], Wellcome Trust IEH Award [102431]; the Engineering and Physical Sciences Research Council [EP/H046410/1]; and the Medical Research Council Strategic Fund [MR/K0006355/1]. The research was funded by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomasʼ NHS Foundation Trust and King’s College London and supported by the NIHR Clinical Research Facility (CRF) at Guy’s and St Thomas’. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.References
[1] Lloyd DFA, et al. Three-dimensional visualisation of the fetal heart using prenatal MRI with motion-corrected slice-volume registration: a prospective, single-centre cohort study. The Lancet 393.10181 (2019): 1619-1627.
[2] van Amerom JFP, et al. Fetal whole‐heart 4D imaging using motion‐corrected multi‐planar real‐time MRI. Magn. Reson. Med. (2019);82:1055–1072.
[3] Roberts TA, van Amerom JFP, et al. Fetal whole heart blood flow imaging using 4D cine MRI. Nat. Commun. (2020);11, 4992.
[4] Tsao J, Boesiger P, Pruessmann KP. k-t BLAST and k-t SENSE: dynamic MRI with high frame rate exploiting spatiotemporal correlations. Magn. Reson. Med. (2003);50:1031–42.
[5] Kuklisova-Murgasova M, et al. Reconstruction of fetal brain MRI with intensity matching and complete outlier removal. Medical Image Analysis 16.8 (2012): 1550-1564.
[6] Jackson LH, et al. Respiration resolved imaging with continuous stable state 2D acquisition using linear frequency SWEEP. Magn. Reson. Med. (2019);82.5: 1631-1645.
[7] Roberts TA, et al. Fetal whole-heart 4D blood flow MRI with self-calibrated k-t SENSE. Proc. Intl. Soc. Mag. Reson. Med. 28 (2020): 0096
Figures