0826
GraspMRA: High Temporal Resolution, Non-Contrast Enhanced, Time-Resolved 4D MR Angiography Using Golden-angle Radial Sparse Parallel Imaging
Li Feng1 and Lirong Yan2
1Department of Radiology, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 2USC Stevens Neuroimaging and Informatics Institute, University of Southern California, Los Angeles, CA, United States
1Department of Radiology, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 2USC Stevens Neuroimaging and Informatics Institute, University of Southern California, Los Angeles, CA, United States
Synopsis
Non-contrast enhanced 4D MRA has emerged as a promising approach in charactering flow dynamics. The major challenge of conventional 4D MRA is relatively long scan time. Recently developed 4D MRA combining golden-angle stack-of-stars acquisition and compressed sensing reconstruction can significantly shorten scan time. However, this method only exploits spatial sparsity based on individual frames. The current study aims to test the feasibility of a newly developed low-rank and sparsity-based image reconstruction method to highly accelerate 4D MRA. Our initial results suggest that higher acceleration rates can be achieved using GraspMRA without compromising image quality and temporal fidelity.
Introduction
Non-contrast time-resolved 4-dimensional MR angiography (4D MRA)1,2 enables non-invasive delineation of flow dynamics of blood vessels, which has shown great promise for evaluating cerebrovascular disorders3, such as arteriovenous malformation, stroke, and moyamoya disease. Conventional 4D MRA is typically acquired using a multi-phase segmented 3D Cartesian gradient-echo sequence with arterial spin labeling (ASL) preparation1,2, which generally requires relatively long scan time (5-10 minutes) to achieve sufficient spatial and temporal resolution. Recently, 4D MRA using golden-angle stack-of-stars acquisition with compressed sensing acceleration has been developed4, which offers high spatiotemporal resolution whilst shortening the acquisition time by three fold. However, the image reconstruction implemented in this method only exploits spatial sparsity in a frame-by-frame reconstruction manner. 4D MRA offers substantial temporal correlations that can be exploited to further push imaging accelerations and achieve higher temporal resolution. Therefore, the aim of this study was to develop a highly-accelerated 4D MRA technique termed GraspMRA, which employs Golden-angle Radial Sparse Parallel Imaging in conjunction with a recently proposed GRASP-Pro technique5. This technique is expected to further improve temporal resolution while preserving image quality.Methods
MRI data acquisition:The MRI experiment was performed on a 3T MRI scanner (Prisma, Siemens) using 20 channel head coil. 4D MRA of the brain was acquired using a golden-angle stack-of-stars sequence with bSSFP readouts. Relevant imaging parameters were: FOV= 256x256x48 mm3, spatial resolution=1x1x1.5 mm3, TE/TR=2.43/4.86ms, FA=20-35°, 500 views per shot and one shot per slice. A total of 32 slices were imaged to cover the main branches of circle of Willis with a total scan time of 3 minutes.
Image reconstruction:
The GRASP-Pro reconstruction5 was adapted for 4D MRA reconstruction in a slice-by-slice manner. The overall reconstruction workflow is shown in Figure 1. As shown in the cost functions (Figure 2), GRASP-Pro reconstruction consists of two separate steps. In the first step, a low-spatial-resolution image series (matrix size=64x64) was reconstructed, from which temporal basis functions were learned from the reconstructed images. In the second step, the full-resolution images were then reconstructed using subspace-based reconstruction based on the temporal basis learned from the first step. Such a reconstruction framework enables learning of spatiotemporal correlations from acquired k-space for reconstructing highly-accelerated MR data. More details about the GRASP-Pro reconstruction can be seen in ref [5]. The label and control data were reconstructed simultaneously to generate dynamic image series with two different temporal resolution, one with 10 consecutive spokes per frame and the other one with 20 consecutive spokes per frame. After image reconstruction, maximum intensity projection (MIP) was performed on the subtraction of reconstructed control and label images to delineate blood flow dynamics.
Results and Discussion
4D MRA images were successfully reconstructed using GraspMRA with both 10 and 20 consecutive spokes per frame. Figure 3 shows several representative frames of MIP images in the transverse direction using 10 and 20 spokes, corresponding to temporal resolution of 50 ms and 100 ms, respectively. The dynamic passage of labeled blood through the cerebral vasculature was clearly depicted at both temporal resolutions. It is worth noting that comparable image quality without visible streaking artifacts was obtained by reducing the number of spokes from 20 to 10 for each frame. Time courses from six vascular ROIs from middle cerebral arteries (MCA) and posterior cerebral arteries (PCA) were extracted as shown in Figure 4. Closely matched time courses were observed between 10 spokes and 20 spokes, indicating that GraspMRA allows for a higher acceleration rate without compromising temporal fidelity. Furthermore, relatively shaper peaks were observed in the time courses of posterior cerebral artery (PCA) ROIs, suggesting GraspMRA with a higher acceleration rate could improve the temporal delineation of flow dynamics. This would be potentially useful to capture rapid flow events in clinical applications.Conclusion
This study tested the feasibility of GraspMRA, a technique for highly-accelerated 4D MRA using golden-angle radial sparse parallel imaging with subspace-based image reconstruction. The initial results suggest that 4D MRA with temporal resolution of up to 50 ms could be achieved with satisfying image quality using GraspMRA. Further study will be performed in future to fully validate the performance of GraspMRA and to evaluate its clinical utility in cerebrovascular diseases.Acknowledgements
This work is supported by grants of NIH K25AG056594 and R01NS118019 and BrightFocus Foundation A20201411S.References
- Yan L, Wang S, Zhuo Y, Wolf RL, Stiefel MF, An J, Ye Y, Zhang Q, Melhem ER, Wang DJ. Unenhanced dynamic MR angiography: high spatial and temporal resolution by using true FISP-based spin tagging with alternating radiofrequency. Radiology. 2010 Jul;256(1):270-9.
- Bi X, Weale P, Schmitt P, Zuehlsdorff S, Jerecic R. Non-contrast-enhanced four-dimensional (4D) intracranial MR angiography: a feasibility study. Magn Reson Med. 2010 Mar;63(3):835-41.
- Yu S, Yan L, Yao Y, Wang S, Yang M, Wang B, Zhuo Y, Ai L, Miao X, Zhao J, Wang DJ. Noncontrast dynamic MRA in intracranial arteriovenous malformation (AVM), comparison with time of flight (TOF) and digital subtraction angiography (DSA). Magn Reson Imaging. 2012 Jul;30(6):869-77.
- Zhou Z, Han F, Yu S, Yu D, Rapacchi S, Song HK, Wang DJJ, Hu P, Yan L. Accelerated noncontrast-enhanced 4-dimensional intracranial MR angiography using golden-angle stack-of-stars trajectory and compressed sensing with magnitude subtraction. Magn Reson Med.2018; 79:867-878.
- Feng L, Wen Q, Huang C, Tong A, Liu F, Chandarana H. GRASP-Pro: imProving GRASP DCE-MRI through self-calibrating subspace-modeling and contrast phase automation. Magn Reson Med. 2020 Jan;83(1):94-108.
Figures
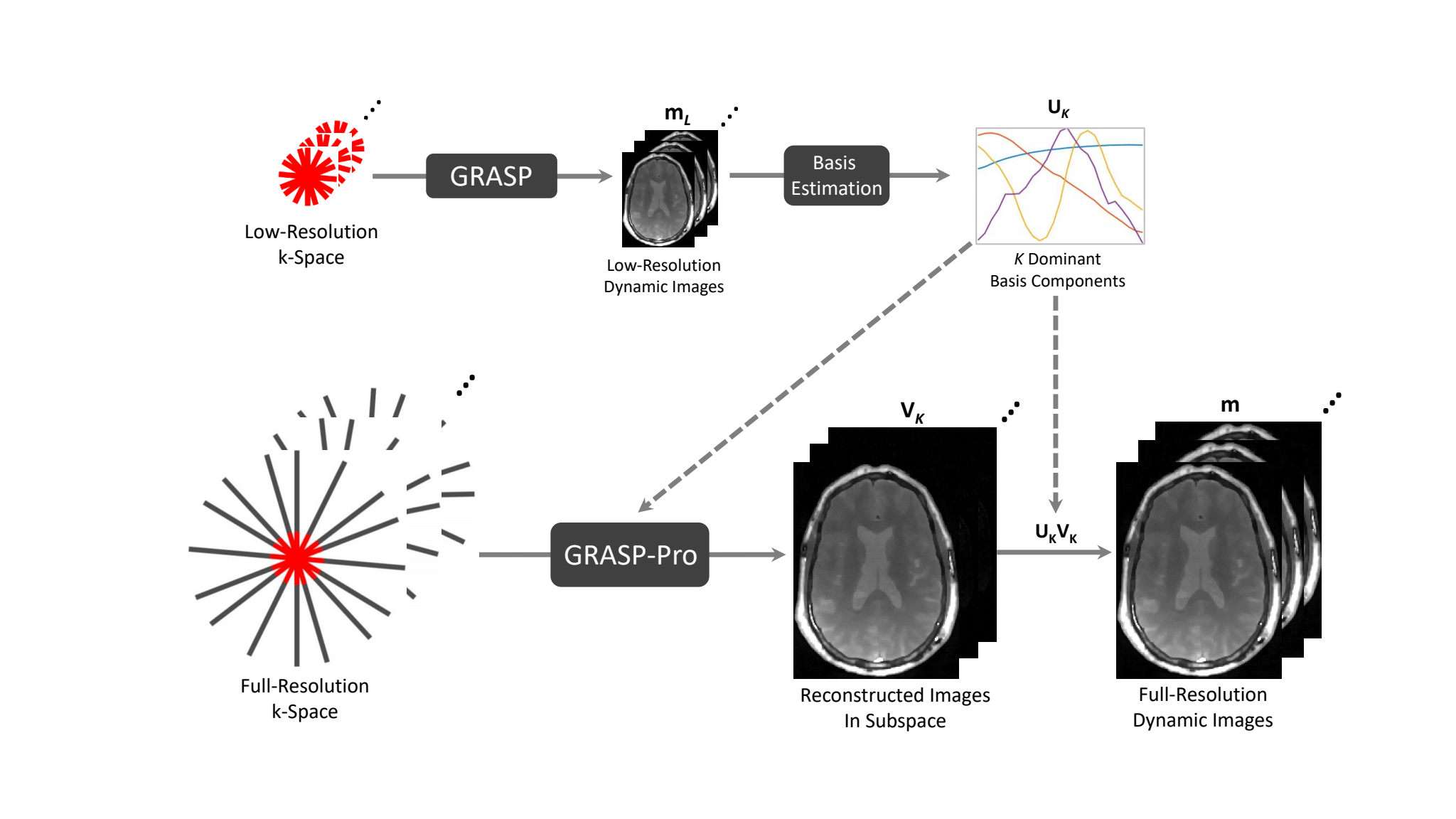
Figure 1. The flowchart of GRASP-Pro reconstruction. In an intermediate step, standard GRASP reconstruction is performed on the low-resolution portion of the sorted radial k-space for estimating temporal basis (U). In the second step, GRASP-Pro is then performed on the full-resolution radial k-space incorporating the pre-learned basis (UK with only the first dominant K basis components) to reconstruct VK, the coefficients to represent the fully-resolution image-series under UK. The final images m is then computed as UKVK.
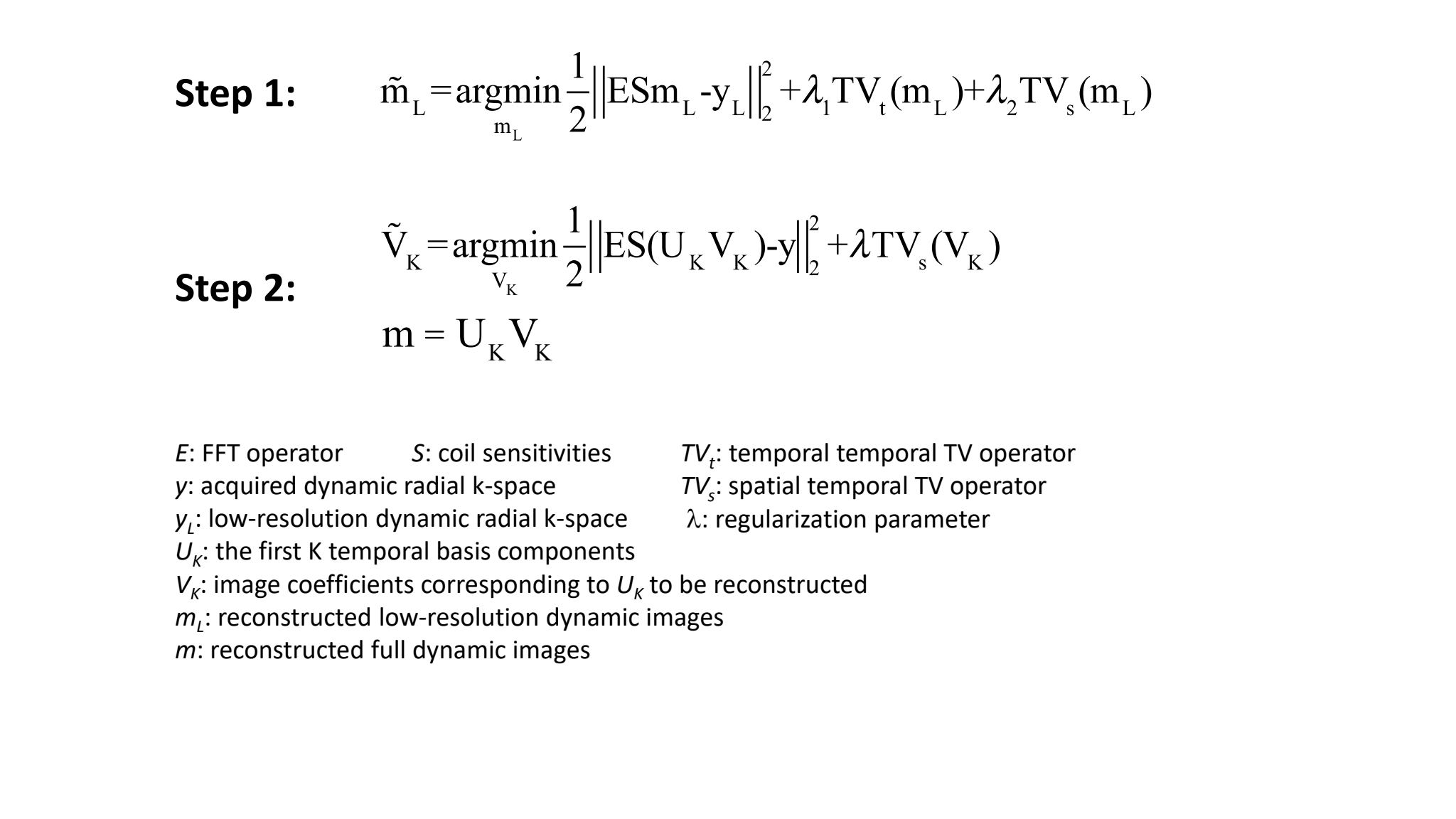
Figure 2. Cost functions for the GRASP-Pro reconstruction. Reconstruction in the step 1 employs standard GRASP reconstruction on low-resolution image series. Reconstruction in step 2 employs subspace and sparsity constraints to reconstruct only the coefficients corresponding to the dominant (K=6) basis components.
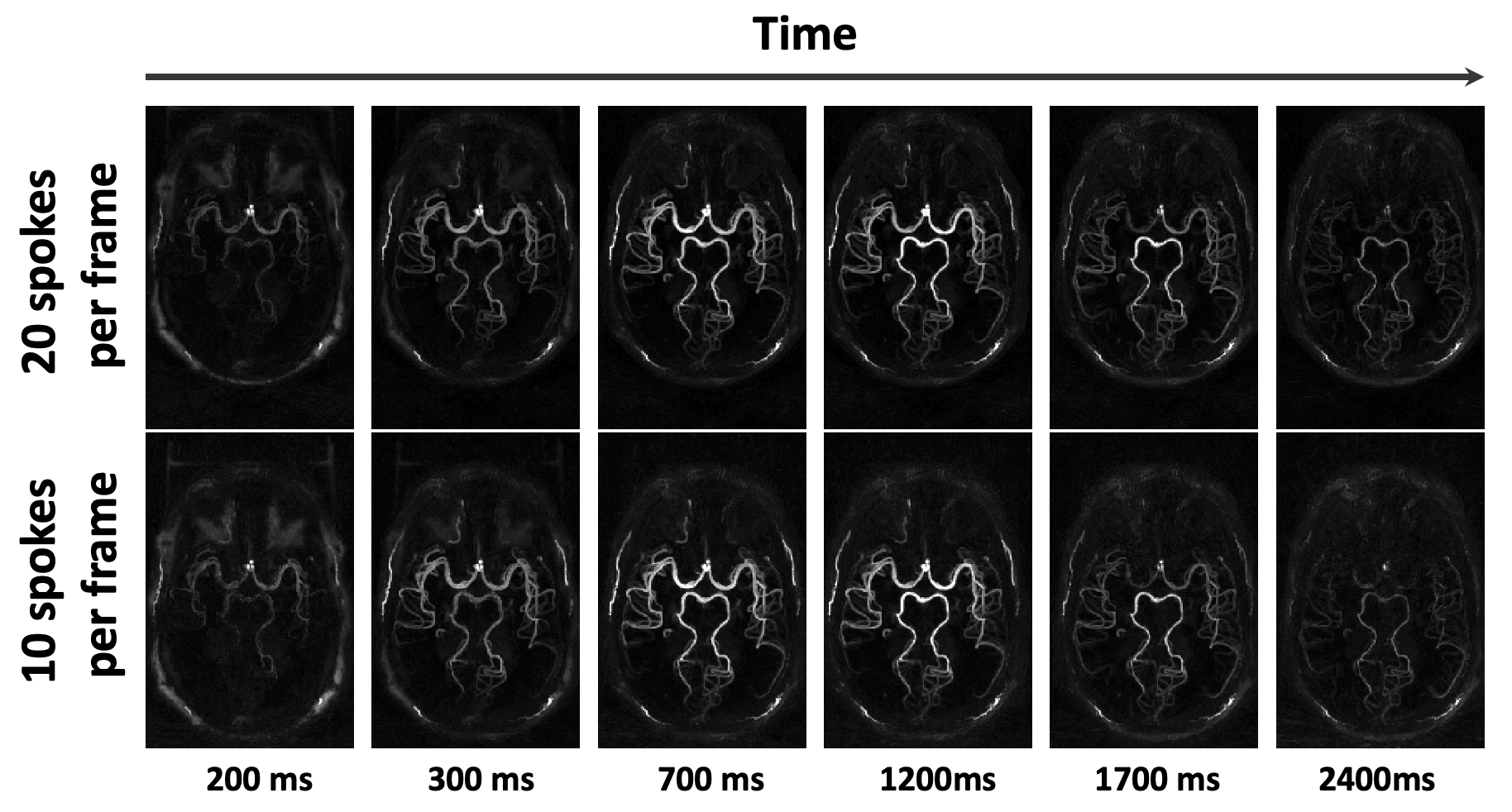
Figure 3. MRA MIP images at 5 representative phases with 10 and 20 spokes per frame, respectively. MIP images at the same TIs were shown for the two reconstructions for better comparison.
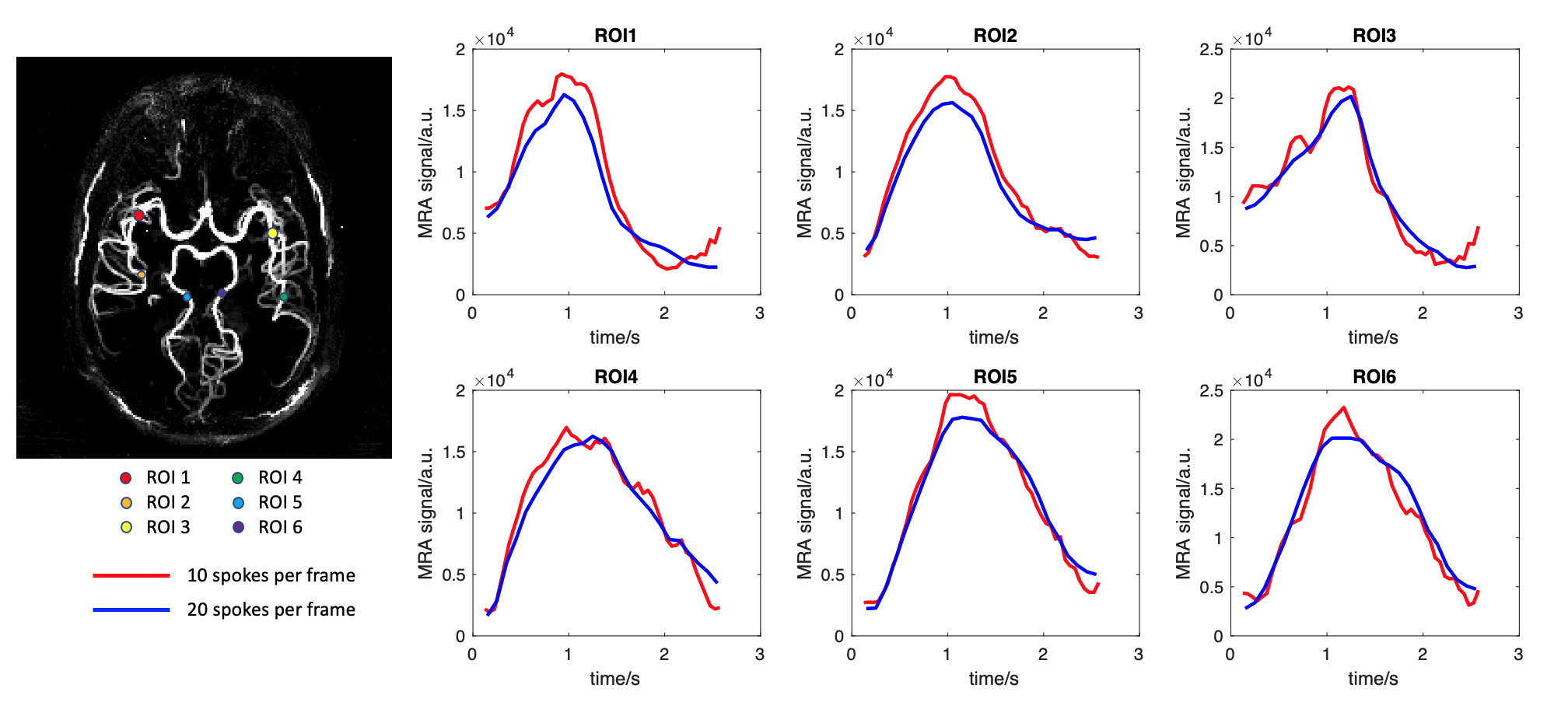
Figure 4. Time courses of MRA signal from 6 arterial ROIs with 10 spokes (red lines) and 20 spokes (blue lines) per frame, respectively. The locations of ROIs are shown on the left.