0812
Ultrafast motion-minimized shoulder MRI with a deep learning constrained Compressed SENSE reconstruction1Philips Japan, Tokyo, Japan, 2Tokyo Metropolitan Police Hospital, Nakano, Japan, 3Philips Healthcare, Best, Netherlands
Synopsis
Shoulder MRI is typically acquired with multiple number of signals averaged (NSA) in order to average out breathing motion artifacts. However, higher NSA leads to a longer scan time and patient discomfort. In this study, we investigated the use of a deep learning-based reconstruction algorithm to highly accelerate shoulder MRI. Adaptive-CS-Net, a deep neural network previously introduced at the 2019 fastMRI challenge, was expanded and presented here as a Compressed-SENSE Artificial Intelligence (CS-AI) reconstruction. The purpose of this study was to compare the image quality of shoulder MRI between reference and accelerated methods; SENSE, Compressed-SENSE, and CS-AI.
Introduction
Shoulder MRI is useful for assessment of shoulder disability and pain1. Typically, shoulder MRI is acquired with multiple number of signals averaged (NSA) in order to average out breathing motion artifacts over the course of the scan. However, higher NSA leads to a longer scan time and patient discomfort. Recently, integrating artificial intelligence (AI) into the MRI reconstruction has attracted much attention. This allows to further minimize scan time2. At the 2019 fastMRI challenge, a novel deep neural network was introduced as Adaptive-CS-Net and showed superior performance for reconstructing knee images from highly undersampled k-space data3–6. The Adaptive-CS-Net was expanded to multiple contrasts and anatomical areas and is presented here as Compressed SENSE AI (CS-AI) reconstruction. It is hypothesized that the acquisition time for shoulder MRI may be significantly shortened while maintaining image quality by using the CS-AI reconstruction algorithm. The purpose of this study was to acquire highly accelerated shoulder MRI using the CS-AI reconstruction and compare the image quality with the conventional method, SENSE, and compressed-SENSE (C-SENSE).Methods
The study was approved by the local IRB, and written informed consent was obtained from all subjects. A total of 2 volunteers were examined on a 3.0T whole-body clinical system (Ingenia Elition X, Philips Healthcare) using an 8-channel shoulder coil. Four multi-slice 2D sequences; proton density weighted (PDw), fat-suppressed PDw, T2-weighted (T2w), and fat-suppressed T2w were all acquired in the coronal and axial plane.The image quality was compared qualitatively between the reference method (commonly used sequence in the clinic based on C-SENSE) and accelerated methods: SENSE, C-SENSE, and CS-AI. The reference scan was acquired with C-SENSE acceleration factor=2 and NSA=2. The total scan time in the reference method for PDw, fat-suppressed PDw, T2w, and fat-suppressed T2w was 2:10min, 2:10min, 2:08min, and 1:51min, respectively. For the accelerated scans, data was acquired in two breath holds with acceleration factor=4 and NSA=1. The total scan time for PDw, fat-suppressed PDw, T2w, and fat-suppressed T2w was 40.0sec, 40.0sec, 38.9sec, and 35.2sec, respectively. The TR/TE for PDw, fat-suppressed PDw, T2w, and fat-suppressed T2w were 2500/30, 2500/30, 2778.8/80, and 3000/65, respectively. Following parameters were common to all examinations: FOV=160×160mm, 22 slices, voxel size=0.5×0.7×3mm, FA=90.
The CS-AI model used in this study is the extension of the previously introduced AI-based reconstruction algorithm, Adaptive-CS-Net5,6. In CS-AI, the iterative optimization procedure in the C-SENSE reconstruction chain is unrolled for a fixed number of reconstruction blocks. Each block consists mainly of Unet-like architecture, which performs as a denoiser. The model was trained on more than 700,000 images, including 2D and 3D data, and multiple contrasts and anatomical areas.
Results and Discussions
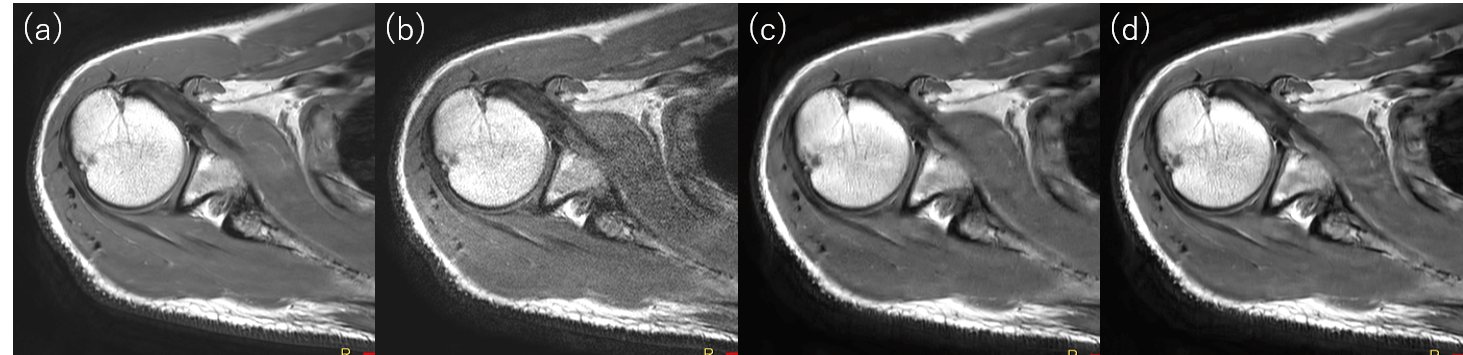
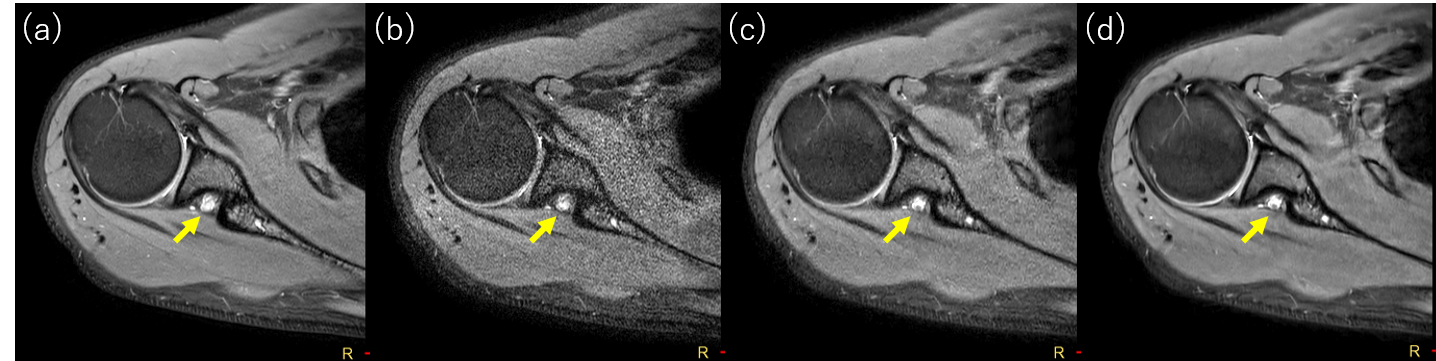
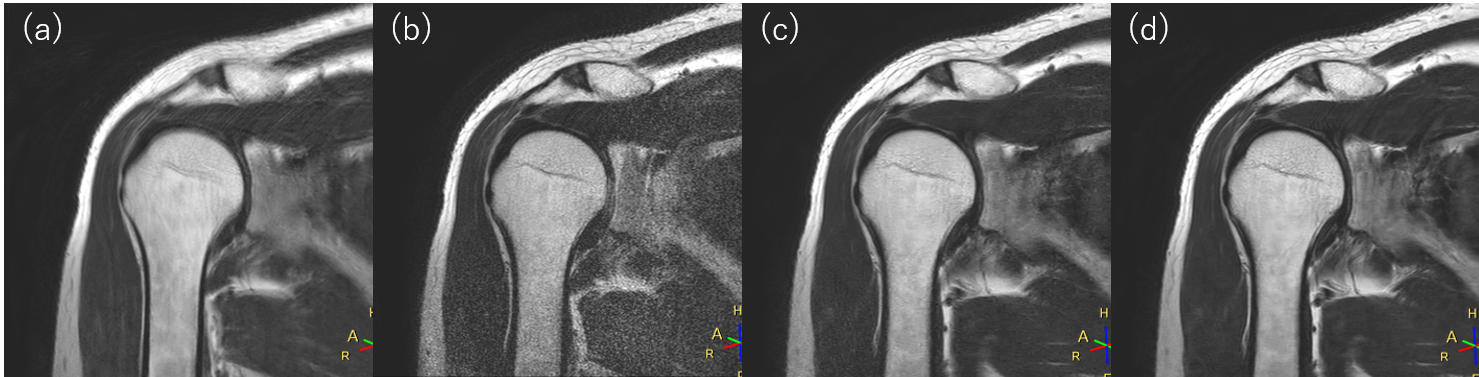
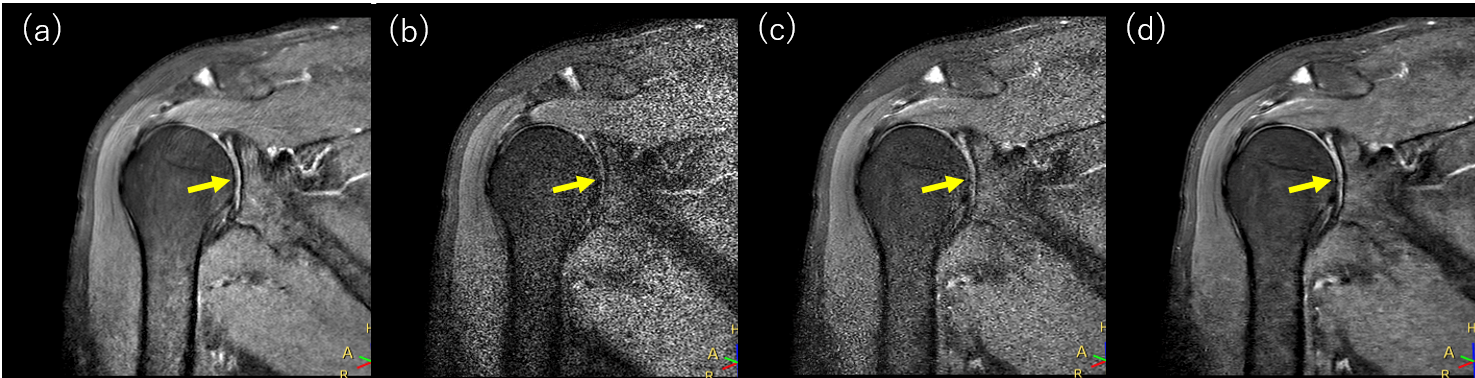
Overall, the CS-AI images demonstrated high denoising performance. In all sequences, the CS-AI showed image quality comparable to that of the reference method, which took more than a factor of 3 longer than the accelerated scans.Figure 1 shows the comparison of the reference, SENSE, C-SENSE, and CS-AI for PDw images. The reference method and CS-AI showed less noise than other methods. The CS-AI produced visually sharper images compared to SENSE and C-SENSE. Figure 2 shows the comparison of the reference, SENSE, C-SENSE, and CS-AI for fat-suppressed PDw images. Both the reference and CS-AI showed good image quality, but the CS-AI demonstrated a better depiction of small structures such as suprascapular nerve (arrow). This suggests that the scan acceleration with the noise reduction by CS-AI reconstruction may be useful for getting a high-quality image by minimizing the breathing motion. Figure 3 shows the comparison of the reference, SENSE, C-SENSE, and CS-AI for T2w images. The reference method showed an ambiguous appearance of edges compared to other methods likely owing to the prolonged scan time. The C-SENSE and CS-AI methods showed less noise compared to SENSE. Small structures may be better visualized in CS-AI than C-SENSE. Figure 4 shows the comparison of the reference, SENSE, C-SENSE, and CS-AI for fat-suppressed T2w images. The SENSE and C-SENSE images became very noisy and were not suitable for diagnosis. However, the CS-AI significantly reduced the noise and had a noise level comparable with the reference method. Due to the reduced noise, structures with high signal such as synovial fluid (arrow) were well depicted in the CS-AI as well as the reference.
Conclusion
In this study, we compared qualitatively the image quality of shoulder MRI between reference, SENSE, C-SENSE, and CS-AI reconstruction methods. Our results suggest that the CS-AI may be able to provide the image quality equivalent to the reference method in a significantly shorter acquisition time. The CS-AI allows to do regular shoulder MRI scans in 2 breath holds and this can be a preferable approach over the conventional averaging method to avoid motion artifacts. Further data collection is required to determine the advantage of CS-AI over other scan acceleration techniques.Acknowledgements
No acknowledgement found.References
1. Tashjian RZ. Epidemiology, Natural History, and Indications for Treatment of Rotator Cuff Tears. Clin Sports Med. 2012;31(4):589-604.
2. Hammernik K, Klatzer T, Kobler E, et al. Learning a variational network for reconstruction of accelerated MRI data. Magn Reson Med. 2018;79(6):3055-3071.
3. Knoll F, Zbontar J, Sriram A, et al. fastMRI: A Publicly Available Raw k-Space and DICOM Dataset of Knee Images for Accelerated MR Image Reconstruction Using Machine Learning. Radiol Artif Intell. 2020;2(1):e190007.
4. Knoll F, Murrell T, Sriram A, et al. Advancing machine learning for MR image reconstruction with an open competition: Overview of the 2019 fastMRI challenge. Magn Reson Med. 2020;(January):mrm.28338.
5. Pezzotti N, Yousefi S, Elmahdy MS, et al. An Adaptive Intelligence Algorithm for Undersampled Knee MRI Reconstruction. IEEE Access. 2020;8:204825-204838.
6. Pezzotti N, de Weerdt E, Yousefi S, et al. Adaptive-CS-Net: FastMRI with Adaptive Intelligence. arxiv. 2019;(NeurIPS).
Figures