0801
Technical feasibility and imaging of transcranial MR-guided in-vivo Histotripsy treatment1Biomedical Engineering, The University of Michigan, Ann Arbor, MI, United States, 2Department of Neurosurgery, The University of Michigan, Ann Arbor, MI, United States
Synopsis
Feasibility of transcranial MR-guided histotripsy for an in-vivo large animal model is established. Eight juvenile pigs were treated using an in-house, 128 channel histotripsy array at a wide range of sites around the brain. Target localization was done using fiducials placed on the array using pre-treatment MR images. Lesions were generated in all the pigs and were visualized in post treatment MRI scans and histology. In acute treatment phase, treatment effects were visible on T2*,T2, T1/T2 FLAIR weighted images. This is the first study to exhibit feasibility of in-vivo transcranial MR-guided histotripsy treatment.
Introduction
Histotripsy is a focused ultrasound (FUS) based treatment method that relies on short duration, high amplitude pressure pulses to generate precise targeted cavitation in tissues1,2. In contrast to conventional high intensity focused ultrasound (HIFU) treatments that rely on thermal necrosis, histotripsy relies solely on a rapid expansion and collapse of generated bubbles. This rapid motion causes mechanical fractionation and liquefaction of tissues without any damage to neighboring tissues and negligible heating.The aim of this work was to study feasibility of in-vivo MR-guided transcranial histotripsy for brain treatment in a large animal model. As opposed to recent human trials of histotripsy to treat liver tumors that utilize ultrasound imaging guidance, the brain poses a unique challenge due to - 1. the presence of the skull that causes aberration and 2. millimeter precision required to steer clear of crucial regions in the brain. We investigate transcranial MR-guided Histotripsy (tcMRgHt) as a method for brain treatment. MRI is an ideal candidate for guiding the brain treatment due to its superior soft tissue contrast, high resolution, and multiple contrast mechanisms. MRI is also used for post-treatment analysis of treatment effects3. This is the first in-vivo study to establish the feasibility of in-vivo tcMRgHt treatment. We show that tcMRgHt can be used to localize the treatment region in various locations in the pig brain through an excised human skull and we study the acute response to the treatment.
Methods
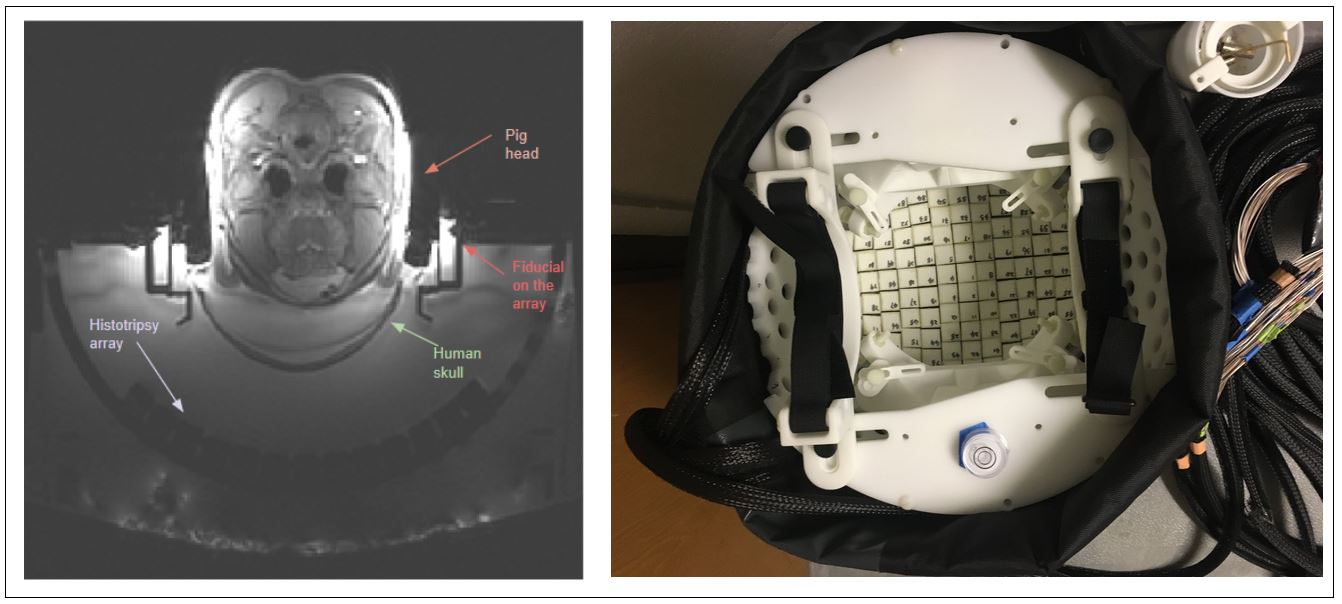
Under the University Committee on Use and Care of Animals approval, 8 juvenile pigs were treated for this acute study. Two days prior to treatment, a craniectomy was performed to surgically remove part of the pig skull and allow propagation path for the histotripsy pulses. The scalp was stitched back after the craniectomy and any remaining gas pockets were allowed to resorb back into the tissue. Histotripsy pulses were delivered using a custom built 128 channel, 700 kHz histotripsy array. The array was submerged in a 2% degassed saline solution and an excised human skull was placed over the pig head to emulate the effects of human skull. The complete experimental setup is shown in Figure 1. Prior to treatment, T2*- and T2- weighted images were taken to localize the treatment spot using fiducials constructed on the histotripsy array. Post treatment T2*,T2,T1 FLAIR and T2 FLAIR images were taken immediately after and 2-4 hours post treatment to observe acute treatment effects. Histological analysis was also performed to evaluate the effect of treatment.Results
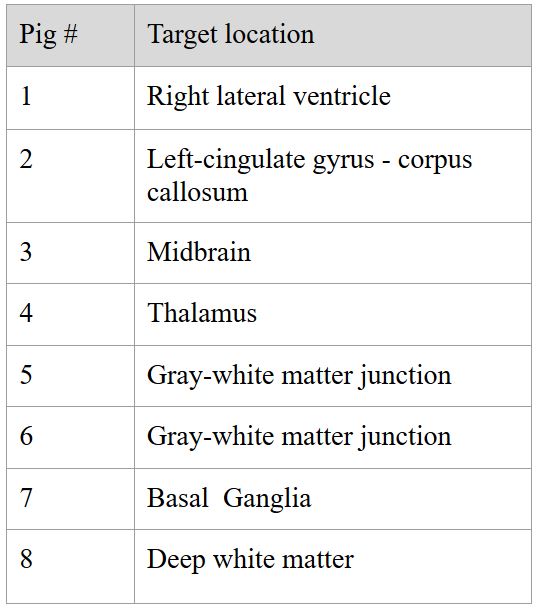
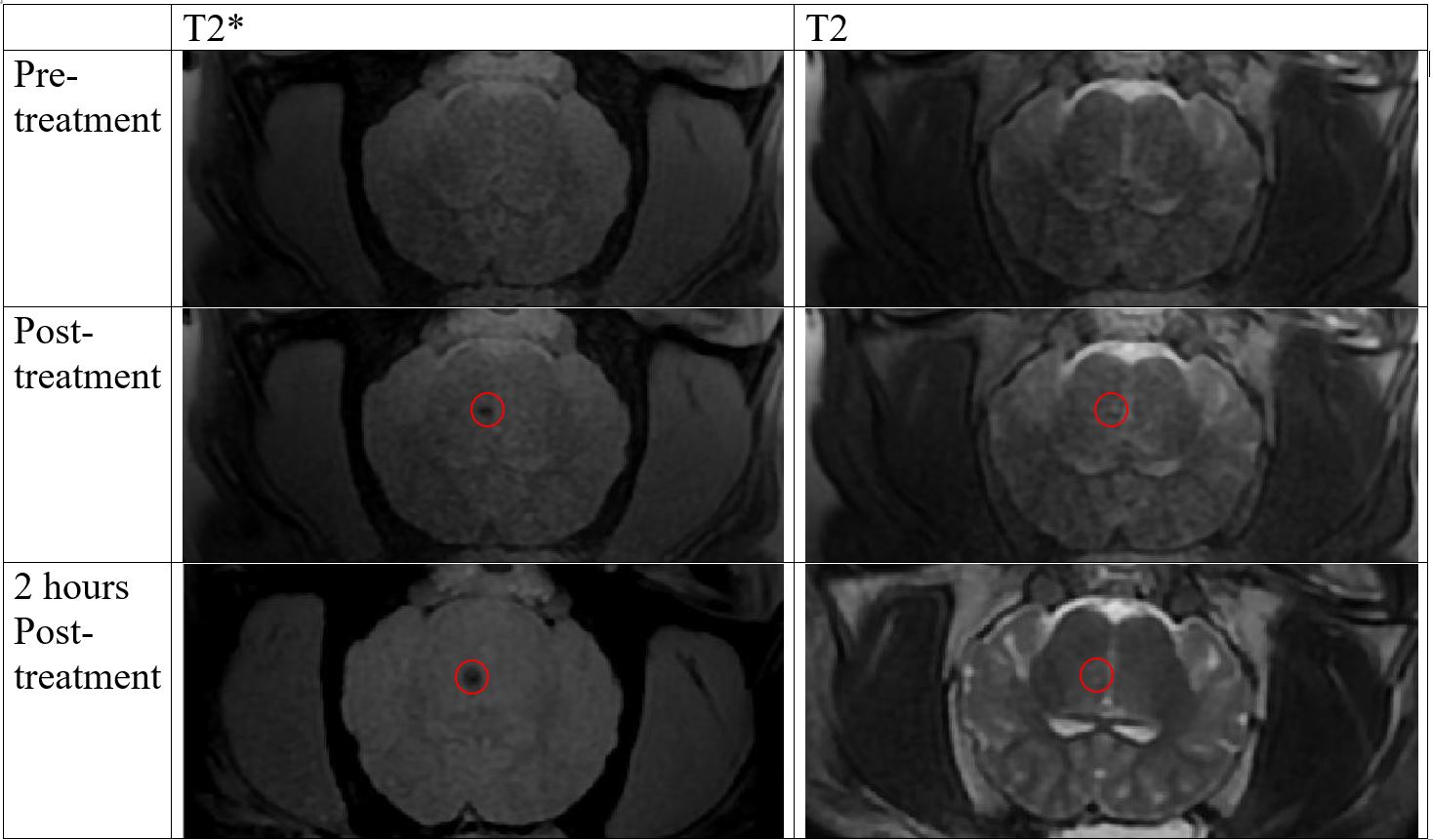
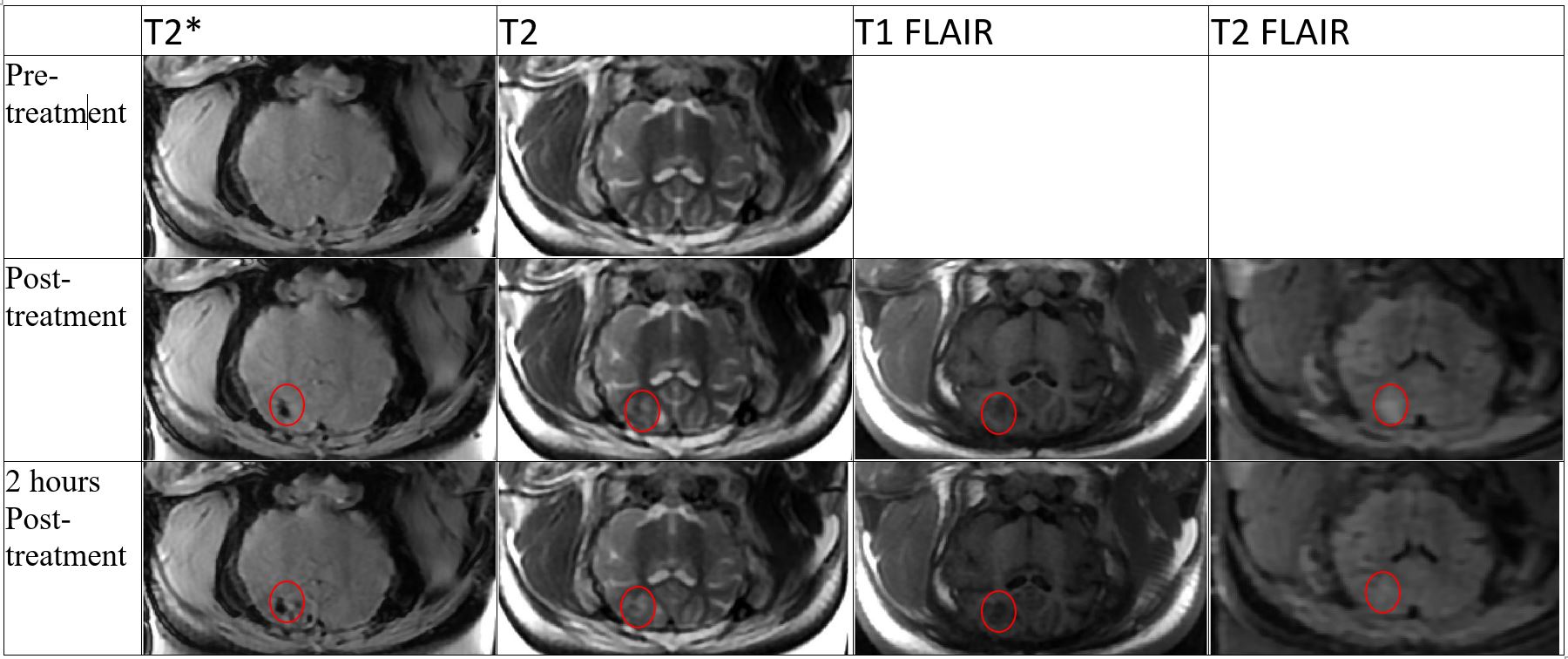
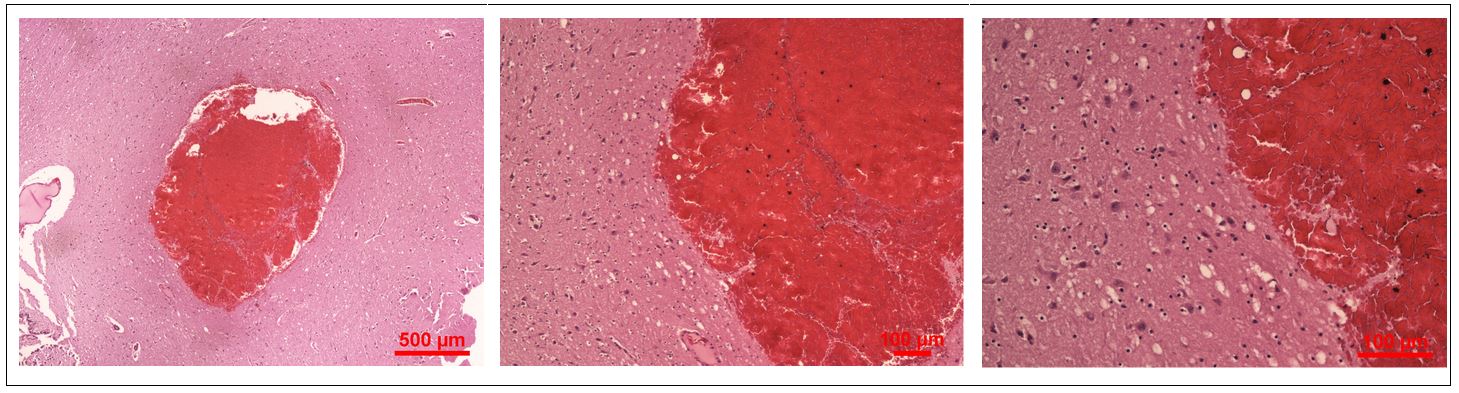
Histotripsy pulses were delivered at a Pulse Repetition Frequency (PRF) of 10 Hz to 3x3x3mm3 to 6x6x6mm3 grid with 1 or 1.5mm grid spacing and 50 pulses/location. The target locations are outlined in Table 1. Lesions were generated at the target locations in the brain and visualized on MR images for all 8 pigs. On T2 and T2 FLAIR images, histotripsy ablation zones contained hyperintense and hypointense regions compared to the surrounding brain tissue, associated with multiple effects, amongst liquefaction of tissue, swelling, lysed and non-lysed red blood cells (RBCs). On T2* images following the treatment, the treatment zone appeared hypointense due to presence of blood. This region is bigger than the actual ablation region due to ‘blooming artifact’ caused by the susceptibility change from iron in blood. Figure 2 shows the treatment with target location in the midbrain. For this treatment, the observed ablation zone was smaller than the target size since a part of the transducer was blocked by pig skull, and sufficient energy was not delivered to all treatment spots. Figure 3 displays the treatment at the gray-white matter junction. For this treatment, T2 shows a white and dark band, while T2* shows similar “blooming artifacts” around the treatment region. Figure 4 shows the histology corresponding to location and volume of the ablation zone on MRI in Figure 2, demonstrating a mixture of acellular debris and RBC within the ablation zone with sharp boundary separating from the intact surrounding brain tissue.Since the aim of this work was to test the feasibility to perform tcMRgHt and imaging treatment effects, more experiments will be run to decipher the precise nature of effects that the histotripsy treatment causes on the MRI contrast mechanisms.
Conclusion and Discussion
This study demonstrates the in-vivo feasibility of tcMRgHt in a pig model. Histotripsy treatment was successfully delivered to various target locations in 8 pigs through an excised human skull. In this study, MRI fiducial markers on the histotripsy array were used to coregister the histotripsy focus to MR images for targeting. Future studies will use MR-thermometry with low heating and/or MR-ARFI to establish a target location before performing histotripsy treatment, as both methods have been used for HIFU targeting in the brain. We also plan to develop diffusion-weighted MRI to monitor histotripsy-induced cavitation and tissue effects during treatment.Acknowledgements
This work is supported by NIH Grant R01EB028309 and the Focused Ultrasound Foundation.References
1. Xu Z, Ludomirsky A, Eun LY, et al. Controlled ultrasound tissue erosion. Proc IEEE Ultrason Symp. 2003;1(6):732-735. doi:10.1109
2. Parsons JE, Cain CA, Abrams GD, Fowlkes JB. Pulsed cavitational ultrasound therapy for controlled tissue homogenization. Ultrasound Med Biol. 2006;32(1):115-129. doi:10.1016/j.ultrasmedbio.2005.09.005
3. Sukovich JR, Cain CA, Pandey AS, et al. In vivo histotripsy brain treatment. J Neurosurg. 2019;131(4):1331-1338. doi:10.3171/2018.4.JNS172652
Figures