0744
Can pulmonary thin-section MRI with UTE<200μs be applied for lung cancer screening similar to CT?1Radiology, Fujita Health University School of Medicine, Toyoake, Japan, 2Joint Research Laboratory of Advanced Medical Imaging, Fujita Health University School of Medicine, Toyoake, Japan, 3Division of Functional and Diagnostic Imaging Research, Department of Radiology, Kobe University Graduate School of Medicine, Kobe, Japan, 4Canon Medical Systems Corporation, Otawara, Japan, 5Diagnostic Radiology, Hyogo Cancer Center, Akashi, Japan
Synopsis
No report has been found to compare the capability for lung cancer screening among pulmonary MR imaging with ultra-short TE (UTE), low-dose CT (LDCT) and standard-dose CT (SDCT). We hypothesized that pulmonary MR imaging with UTE has a similar potential to detect pulmonary nodules and evaluate Lung-RADS classification and can apply lung cancer screening as well as CT. The purpose of this study was to compare the capability for lung cancer screening among pulmonary MR imaging with UTE and both dose CTs.
Introduction
National Lung Cancer Screening Trail (NLST) and The Dutch-Belgian Lung Cancer Screening trial (NELSON) reported the reduction in mortality with the use of low-dose computed tomography (LD-CT) scan to screen high risk individuals (1, 2). Therefore, major organizations have adopted or considered to apply LDCT for lung cancer screening in high risk populations. In addition, American College of Radiology has designed Lung-RADS as a quality assurance tool to standardize lung cancer screening CT reporting and management recommendations, reduce confusion in lung cancer screening CT interpretations, and facilitate outcome monitoring (3). Since 2016 (4-6), pulmonary MR imaging with ultrashort TE (UTE) less than 200ms has been suggested as having a potential to detect nodule, evaluate lung parenchymal abnormality and play as substitution to LD-CT as well as standard-dose CT (SD-CT). However, no report has been found to compare the capability for lung cancer screening among pulmonary MR imaging with UTE, LDCT and SDCT. We hypothesized that pulmonary MR imaging with UTE has a similar potential to detect pulmonary nodules and evaluate Lung-RADS classification and can apply lung cancer screening as well as CT. The purpose of this study was to compare the capability for lung cancer screening among pulmonary MR imaging with UTE (UTE-MRI) and both dose CTs.Materials and Methods
110 candidates (64 males: mean age, 67 years and 46 females: mean age, 65 years) who hope to undergo lung cancer screening were examined with pulmonary UTE-MRI at a 3T system (Vantage Titan 3T, Canon Medical Systems Corporation, Otawara, Japan) by respiratory-gated 3D radial UTE pulse sequence (TR 4.0ms/ TE 110-192μs, flip angle 5 degree, 1x1x1 mm3 voxel size), SD-CT (270 mA) and LD-CT (60 mA) at 64-detector row CTs (Aquilion 64, Canon Medical) and 320-detector row CTs (Aquilion ONE, Canon Medical). According to SDCT findings, all nodules were divided into solid and part-solid nodules and ground glass nodules. In each patient, probability of presence at each pulmonary nodule was assessed on all three methods by means of 5-point visual scoring system by two board certified chest radiologists. In addition, all nodules were classified based on Lung-RADS on each method by same radiologists. To compare nodule detection capability, Jackknife alternative free-response receiver operating characteristic (JAFROC) analysis were performed among all methods. Then, detection rates were also compared among three methods by McNemar’s test. To evaluate Lung-RADS classification capability, inter-observer agreement of each method was evaluated by kappa statistics with χ2 test. In addition, inter-method agreements were also assessed by kappa statistics with χ2 test were performed. A p value less than 0.05 was considered as significant in this study.Results
Examples of SD-CT, LD-CT and UTE-MRI in Lung-RADS Category 2, 4A and 4X are shown in Figure 1. Results of JAFROC analysis are shown in Figure 2. Figure of merit (FOM) of all methods based on consensus reading (UTE-MRI: FOM=0.89, LD-CT: FOM=0.86, SD-CT: FOM=0.89) had no significant differences (F=0.13, p=0.89). In addition, true-positive ratio (TP) and false-positive rate per case (FPR) of all methods (UTE-MRI: TP, 0.93, FPR, 0.55; LD-CT; TP, 0.93, FPR, 0.68; SD-CT: TP, 0.93, FPR, 0.62) had no significant difference (p>0.05). Inter-observer agreement for Lung-RADS classification on each method is shown in Figure 3. Interobserver agreement of each method was as follows: UTE-MRI: κ=0.92, p<0.0001; LD-CT: κ=0.93, p<0.0001; and SD-CT: κ=0.96, p<0.0001. Inter-method agreements for Lung-RADS classification are shown in Figure 4. Inter-method agreements were also almost perfect (UTE-MRI vs. LD-CT: κ=0.86, p<0.0001; UTE-MRI vs. SD-CT: κ=0.87, p<0.0001; LD-CT vs. SD-CT: κ=0.95, p<0.0001)Conclusion
Pulmonary MR imaging with UTE has a potential to be applied for lung cancer screening as well as CT.Acknowledgements
This study was financially and technically supported by Canon Medical Systems Corporation.References
- National Lung Screening Trial Research Team, National Lung Screening Trial Research Team, Aberle DR, Adams AM, Berg CD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011; 365(5): 395-409.
- de Koning HJ, van der Aalst CM, de Jong PA, et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N Engl J Med. 2020; 382(6): 503-513.
- American College of Radiology. Lung CT Screening Reporting and Data System (Lung-RADS). Accessed at www.acr.org/Quality-Safety/Resources/LungRADS on 20 November, 2020.
- Ohno Y, Koyama H, Yoshikawa T, et al. Pulmonary high-resolution ultrashort TE MR imaging: Comparison with thin-section standard- and low-dose computed tomography for the assessment of pulmonary parenchyma diseases. J Magn Reson Imaging. 2016; 43(2): 512-32.
- Ohno Y, Koyama H, Yoshikawa T, et al. Standard-, Reduced-, and No-Dose Thin-Section Radiologic Examinations: Comparison of Capability for Nodule Detection and Nodule Type Assessment in Patients Suspected of Having Pulmonary Nodules. Radiology. 2017; 284(2): 562-573.
- Wielpütz MO, Lee HY, Koyama H, et al. Morphologic Characterization of Pulmonary Nodules With Ultrashort TE MRI at 3T. AJR Am J Roentgenol. 2018; 210(6): 1216-1225.
Figures
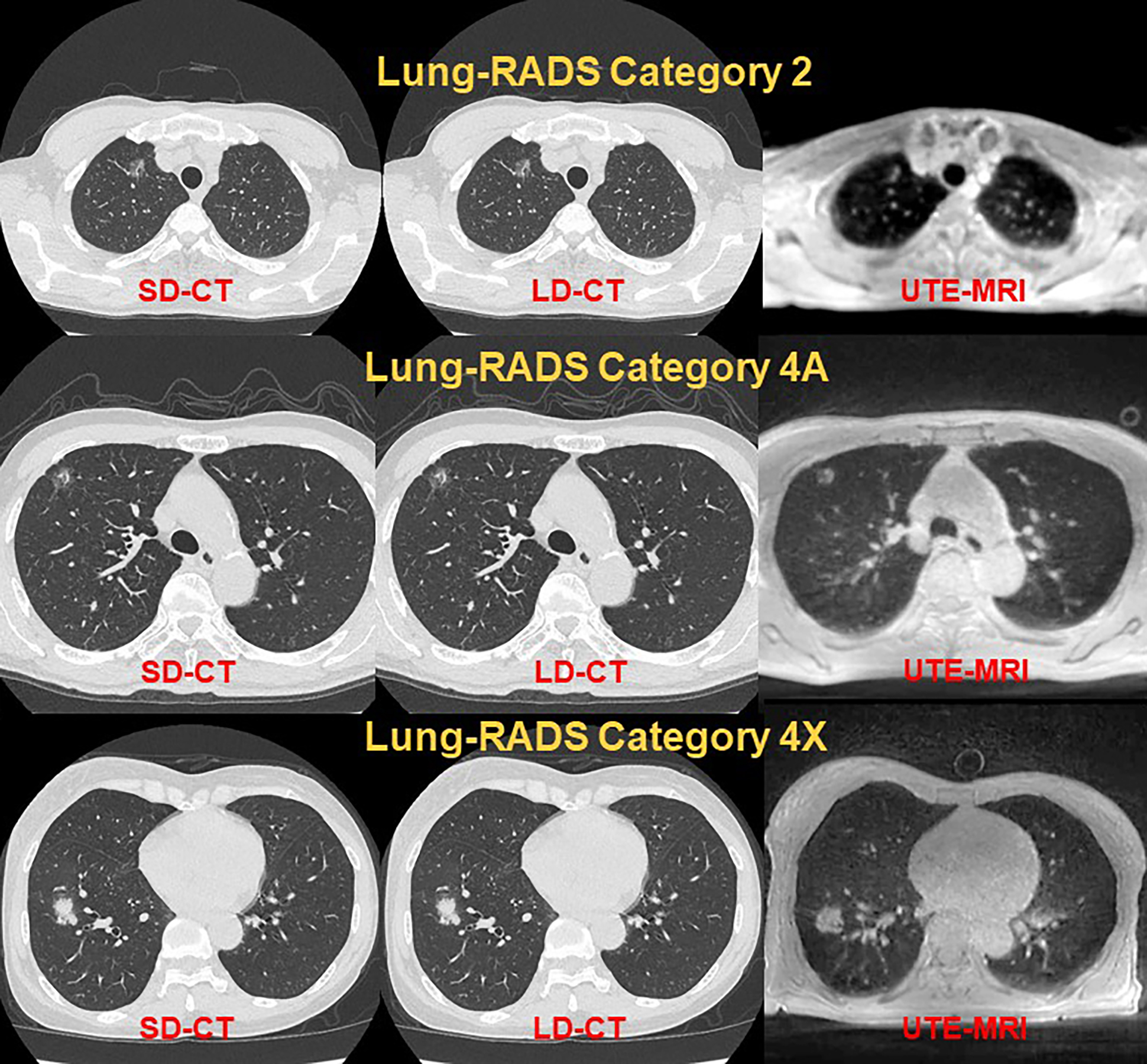
Figure 1. Examples for standard-dose (SD-CT: Left), low-dose CT (LD-CT: Middle) and pulmonary MR imaging with UTE (UTE-MRI: Right) in Lung-RADS Category 2 (1st line), catefory 4A (2nd line) and Category 4X (3rd line).
Each method has no difference of radiological findings as well as Lung-RADS classification in each subject.
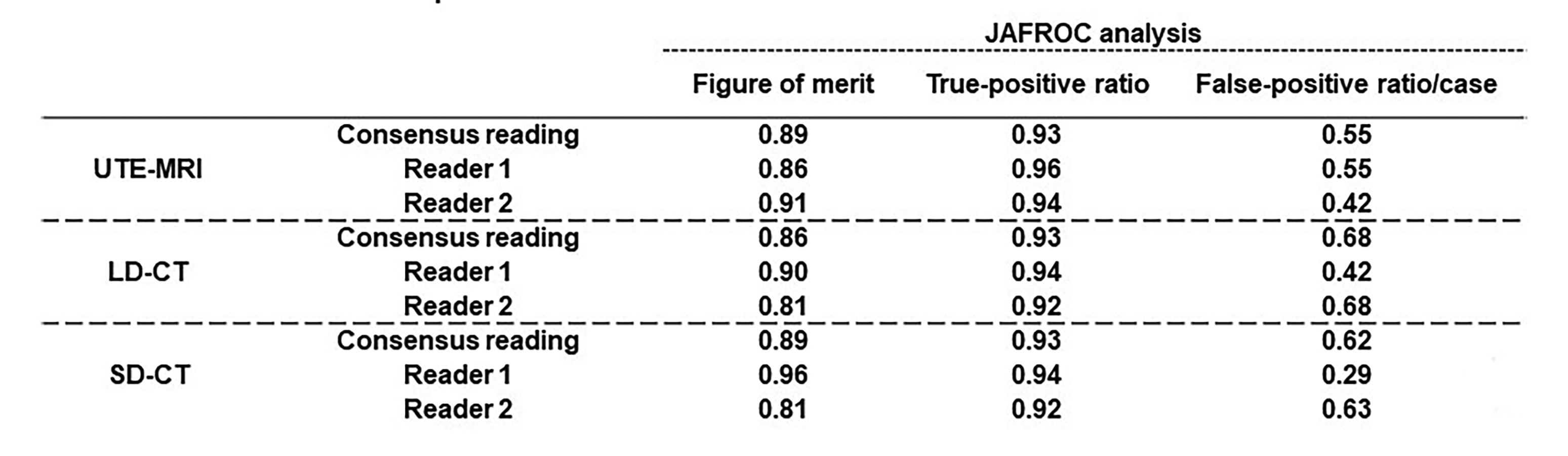
Figure 2. Results of JAFROC analysis for lung nodule detection.
There were no significant differences of figure of merit, true-positive ratio and false-positive ratio/case among all methods.
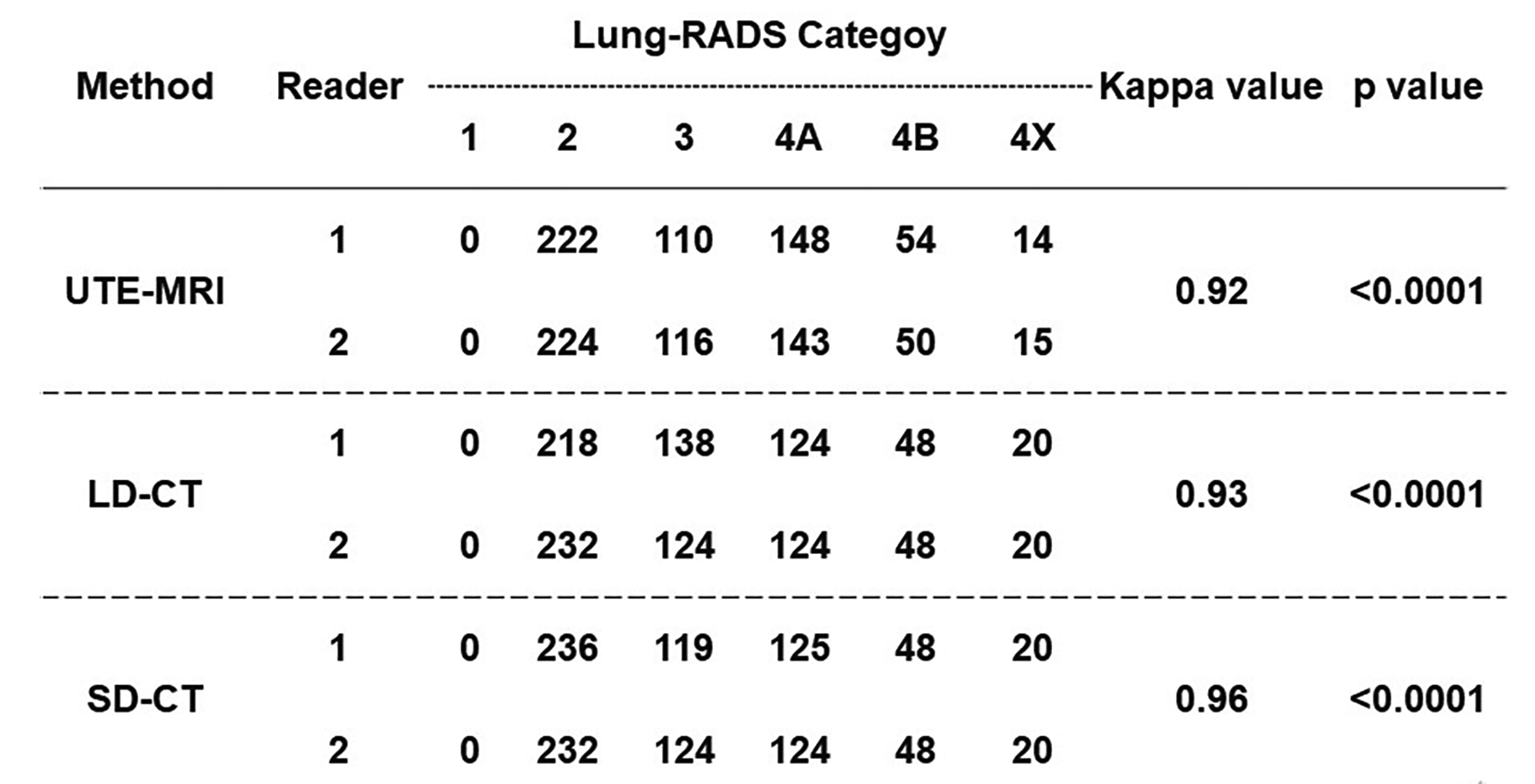
Figure 3. Inter-observer agreement of each method.
Inter-observer agreements of all methods are as follows: UTE-MRI, κ=0.92, p<0.0001; LD-CT, κ=0.93, p<0.0001; SD-CT, κ=0.96, p<0.0001.
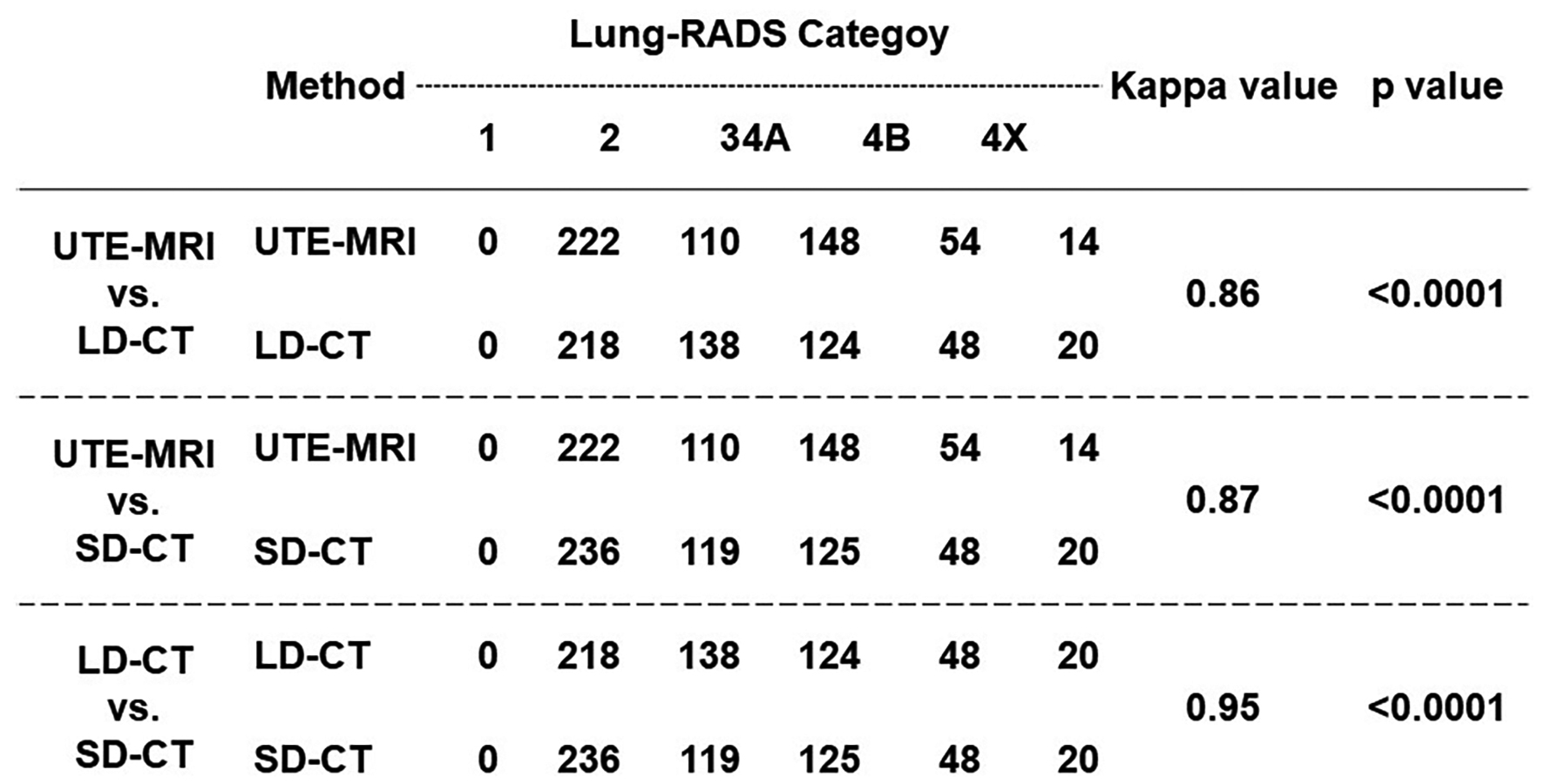
Figure 4. Inter-method agreement among all methods.
Inter-method agreements of all methods are as follows: UTE-MRI vs. LD-CT, κ=0.86, p<0.0001; UTE-MRI vs. SD-CT, κ=0.87, p<0.0001; LD-CT vs. SD-CT, κ=0.95, p<0.0001.