0683
Hyperpolarized 129Xe MRI Ventilation Texture Features to Characterize Long-haul COVID-19 Survivors1Robarts Research Institute, Western University, London, ON, Canada, 2Department of Medicine, Western University, London, ON, Canada
Synopsis
Persistent, long-term COVID-19 symptoms and pulmonary function abnormalities, beyond the acute infectious pulmonary disease phase, is now recognized in certain patients and referred to as long-haul or long COVID. We used hyperpolarized 129Xe MRI ventilation defect percent (VDP) and texture analysis to evaluate and characterize second-order 129Xe MRI ventilation texture features in a pilot study of participants with long-haul COVID-19. We observed statistically significant differences in 129Xe MRI VDP and ventilation texture features between COVID-19 survivors and volunteers who were not infected. Second-order 129Xe MRI ventilation texture features dichotomized long-haul COVID-19 and volunteers in the absence of qualitative VDP differences.
Introduction
COVID-19 infection may result in severe symptoms with potential permanent structural damage causing impaired lung function.1,2 In the past year, pulmonary imaging has focused on the diagnosis and monitoring of the COVID-19 infection. Both thoracic x-ray computed tomography (CT) and magnetic resonance imaging (MRI) have been used primarily as diagnostic tools, for identifying consolidation, ground-glass opacities and crazy-paving patterns.2,3 The pathologies and mechanisms that drive persistent symptoms and abnormal lung function in participants who experience long-haul COVID-19 are, as yet, not well-understood.4Hyperpolarized noble gas MRI ventilation abnormalities are common in patients with asthma, chronic obstructive pulmonary disease (COPD), cystic fibrosis and radiation-induced lung injury.5 Ventilation defect percent (VDP) can be used to localize and quantify the inhaled gas distribution abnormalities. Commonly used MRI ventilation defect segmentation methods binarize or cluster ventilated and poorly ventilated regions. However, this approach cannot quantify ventilation patchiness and texture differences. Texture features including gray-level run length matrices (GLRLM) can be used to quantify the differences in signal intensity across the ventilated regions of the lung.6 From these matrices, second-order texture features, such as short run emphasis (SRE), high gray-level run emphasis (HGRE) and short run, high gray-level emphasis (SRHGE), have been used to evaluate ventilation heterogeneity.7 Fine textures are described using short-run texture features while distributions of high-gray level texture features relate to the distribution of high signal intensities or ventilation.
Hyperpolarized 129Xe MRI texture features may provide information about the long-term pulmonary effects of COVID-19. Therefore, the objective of this pilot study was to evaluate and characterize long-haul COVID-19. To accomplish this we extracted 129Xe ventilation MRI of long-haul COVID-19 patients and a control group of never-infected participants. We used texture features of 129Xe MRI ventilation heterogeneity in this pilot study to determine the abnormal heterogeneity that distinguishes long-haul COVID-19 from other chronic lung diseases.
Methods
We evaluated 14 participants who survived COVID-19 infection and who attended a long-haul COVID-19 clinic, with persistent respiratory symptoms, within 3 months of COVID-19 infection and a control group of 14 participants without a history of chronic or recent acute respiratory infection. All participants provided written informed consent to an ethics board approved protocol that included thoracic CT and MRI as well as spirometry, oscillometry and multi-breath inert gas washout.Anatomical 1H and hyperpolarized 129Xe MRI were acquired using a 3.0 Tesla Discovery MR750 (General Electric Health Care, WI, USA) with broadband capability as previously described.8,9 Anatomical proton images were acquired using a fast-spoiled gradient-recalled echo sequence (total acquisition time, 8 seconds; TR msec/TE msec, 4.7/1.2; flip angle, 30°; field of view, 40 × 40 cm2; bandwidth, 24.4 kHz; 128 × 80 matrix, zero padded to 128 × 128; partial echo percentage, 62.5%; 15-17 sections; section thickness, 15 mm; no gap). Static ventilation images were acquired using a three-dimensional fast gradient-recalled echo sequence (total acquisition time, 14 s; TR msec/TE msec, 6.7/1.5; variable flip angle; field of view, 40 × 40 cm2; bandwidth, 15.63 kHz; 128 × 128 matrix; 14 sections; section thickness, 15 mm; no gap). Participants were instructed to inhale 1.0 L of gas (100% N2 for anatomical scan and 400 mL hyperpolarized 129Xe mixed with 600 mL 4He for hyperpolarized scan) to ensure volume matched images for segmentation. MRI was acquired under breath hold conditions. Images were segmented using a semi-automatic method that quantifies VDP using cluster analysis tools.5
We used the GLRLM method, modified for 129Xe MRI texture feature analysis, to calculate 11 second-order texture features.6,7 The signal-to-noise ratio (SNR) of each 129Xe MRI slice was determined such that the texture features were averaged for only those slices with a SNR value greater than 15.
Results
Table 1 provides demographic and imaging characteristics for long-haul COVID-19 participants and the control group. Figure 1 provides 129Xe MRI ventilation patterns in the long-haul COVID-19 participants and control group. Figure 2 shows that there were significant differences in VDP, SRE, HGRE and SRHGE between the two groups.Discussion
129Xe MRI ventilation patterns in long-haul COVID-19 patients and the control group were not qualitatively different. However, the significantly greater SRE in COVID-19 participants suggested regions of heterogeneous or patchy ventilation. An increased HGRE in the COVID-19 group suggests patchy ventilation of greater intensity compared to the control group. A combination of these findings was concomitant with greater SRHGE in COVID-19 participants compared to controls, suggesting that the heterogeneous regions are more intensely ventilated in long-haul COVID-19 participants.Conclusion
Second-order 129Xe MRI ventilation texture features differentiate between long-haul COVID-19 and participants who were not infected and did not have a history of chronic pulmonary disease. Texture analysis provides information regarding the ventilation patterns of long-haul COVID-19 that cannot otherwise be determined. This new information will help frame a prospective study of patients with moderate and severe COVID-19 infection to identify those that may experience long-haul COVID-19.Acknowledgements
No acknowledgement found.References
1 Shaw, B. et al. Radiol Med (2020).
2 Ding, X. et al. Eur J Radiol 127, (2020).
3 Ates, O. F. et al. Acad Radiol 27, 1373-1378, (2020).
4 Nath, A. Neurology 95, 559-560, (2020).
5 Kirby, M. et al. Acad Radiol 19, 141-152, (2012).
6 Haralick, R. M. et al. IEEE Trans. Syst. Man Cybern. Syst. SMC-3, 12 (1973).
7 Zha, N. et al. Acad Radiol 23, 176-185, (2016).
8 Parraga, G. et al. Invest Radiol 42, 384-391, (2007).
9 Svenningsen, S. et al. J Magn Reson Imaging 38, 1521-1530, (2013).
Figures
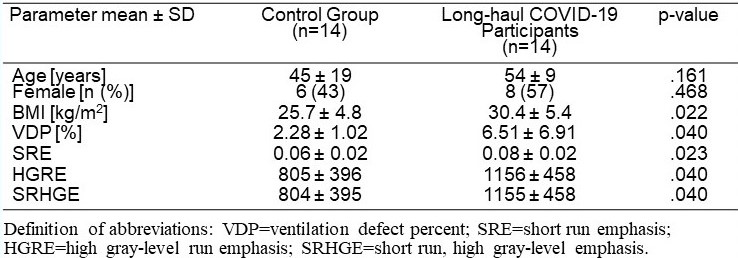
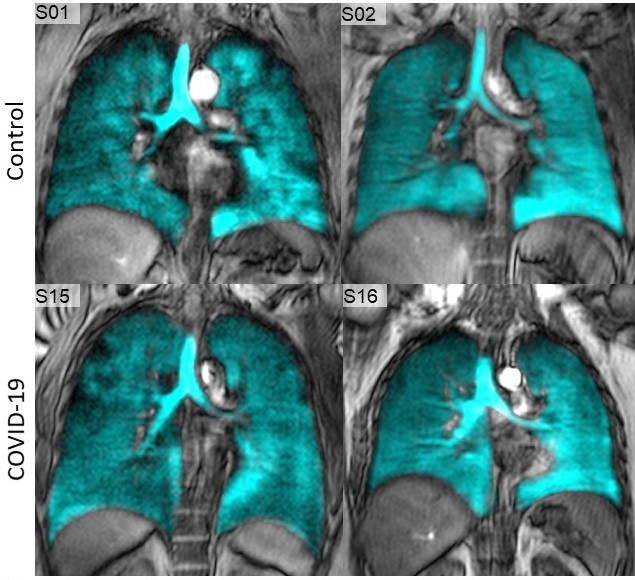
Figure 1: Qualitative results of ventilation comparison between control group and long-haul COVID-19 patients
Control group participants S01 and S02 have a VDP of 2% and 1%, respectively, while COVID-19 patients S15 and S16 have a VDP of 3% and 2%, respectively.
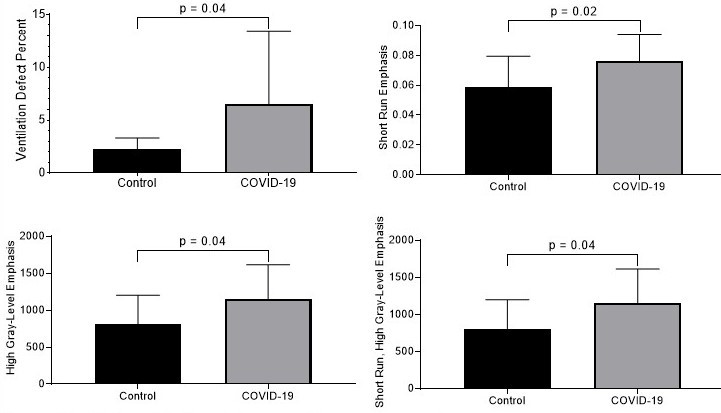
Figure 2: MRI ventilation heterogeneity measurements
Patients with long-haul COVID-19 have increased VDP (A), short run emphasis (B), high gray-level run emphasis (C) and short run, high gray-level emphasis (D) extracted from 129Xe MRI, compared to control group participants.