0504
Spiral-in-out bSSFP Real-Time Cine on a High Performance 0.55T Scanner1Biomedical Engineering, University of Virginia, Charlottesville, VA, United States, 2Radiology & Medical Imaging, University of Virginia, Charlottesville, VA, United States, 3School of Medicine, University of Virginia, Charlottesville, VA, United States, 4Cardiovascular Branch, Division of Intramural Research, National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, MD, United States
Synopsis
This abstract describes a spiral-in-out bSSFP pulse sequence combined with a low rank plus sparse (L+S) image reconstruction for ungated real-time cine on a high performance 0.55T MRI scanner. Preliminary results show that the proposed method is a promising technique for real-time cardiac imaging with high image quality and excellent temporal resolution.
Introduction
Balanced steady-state free procession (bSSFP) is the standard sequence for assessing cardiac function using cardiac MR, because of its short acquisition time and high blood-myocardium contrast1. However, off-resonance phase accrual can produce undesirable banding artifacts in bSSFP, which limits the TR to 3-4ms at 1.5T and even shorter at 3T. Cardiac MRI at low field has recently gained increasing interest2-5. One key merit of low field MRI is a more homogeneous B0 field when compared to 1.5T or 3T scanners, which may extend the TR to 6~8ms to improve sampling efficiency. Therefore, low field offers great advantages for SNR-efficient acquisitions such as spiral and EPI trajectories with a longer readout in cardiac imaging4,5.Recently, we introduced and compared spiral-out and spiral-in-out bSSFP sequences6,7 for accelerated real-time cardiac MRI at 1.5T. The results demonstrated that a spiral-in-out bSSFP sequence combined with a L+S reconstruction8 yields ungated cardiac movies with high image quality and minimal temporal blurring, and can be an alternative to gated and breath-held CINE for the assessment of cardiac function. In this work, we developed a spiral-in/out sequence with an extended TR to acquire real-time spiral cine at 0.55T with high temporal resolution (~36ms) and spatial resolution (~1.7mm) within three seconds.
Methods
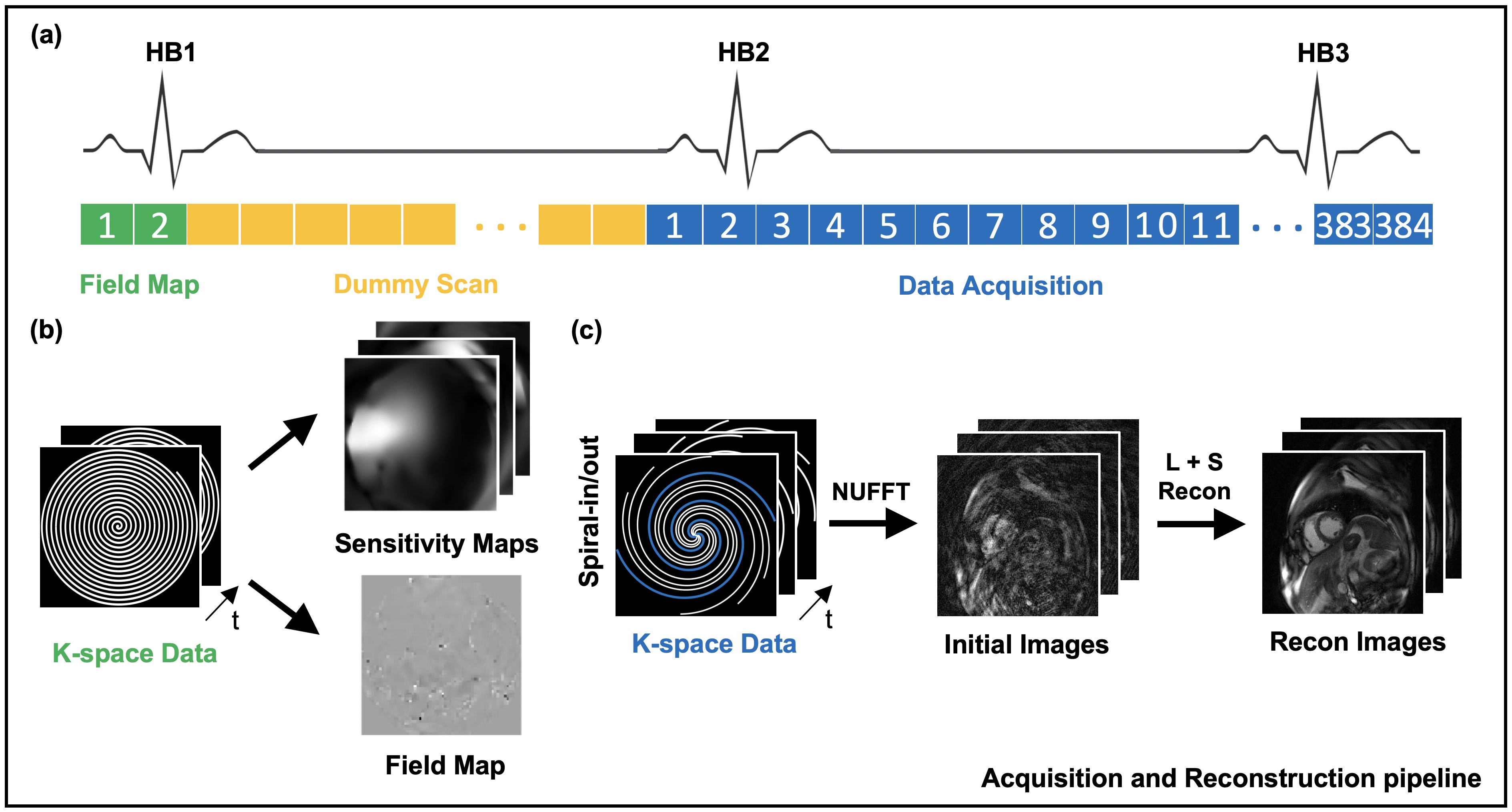
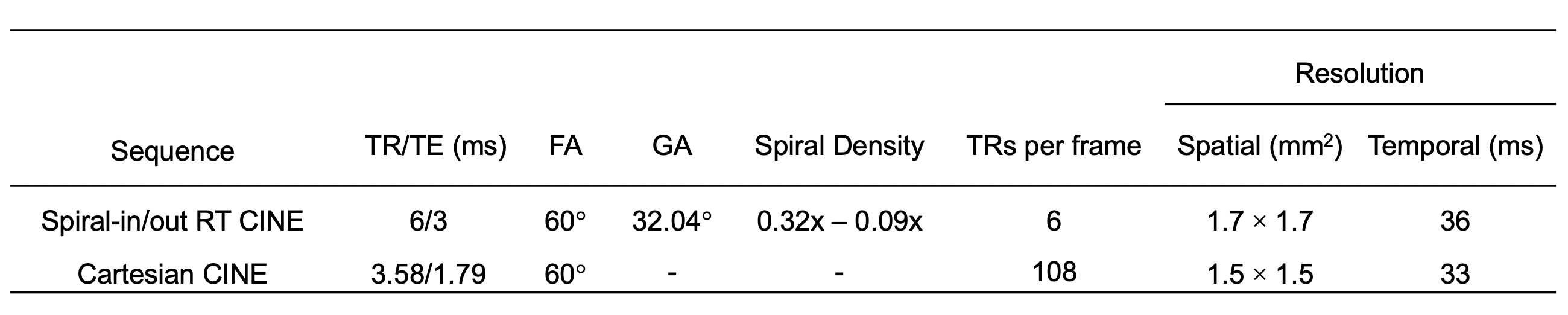
A schematic of the method is depicted in Figure 1. The first two single-shot spirals (green boxes) were fully sampled before the bSSFP acquisition for field map and coil sensitivity map estimation using ESPIRiT9. A dummy scan with 100 TRs was then used (yellow boxes) in order to approach steady state magnetization. Immediately after the pre-scan, dynamic data with a total of 384 spiral arms per slice were collected using a tiny golden angle rotation (blue boxes). Six spiral-in/out readouts with linearly decreasing sampling density were utilized in this study to reconstruct each cardiac frame with an undersampling rate of 8. A view-sharing method and a low rank plus sparse (L+S) algorithm were both used for image reconstruction. The regularization parameters and were set to 0.05 and 0.001, respectively. FOV was set to 340 x 340 mm2, and TR was set to 6ms with a readout length of 4ms. Other sequence parameters and the resulting spatial and temporal resolutions are given in Table 1.All of the experiments were performed on a 0.55T scanner (prototype MAGNETOM Area, Siemens Healthcare, Erlangen, Germany) with high gradient performance (maximum gradient amplitude = 45 mT/m, maximum slew rate = 200 T/m/s). Institutional review board approval and written informed consent were obtained for human studies. For each healthy volunteer, a midventricular short-axis view and a horizontal long-axis view were imaged under breath-held and free-breathing conditions. For each set of experiments, the spiral-in-out bSSFP cine and Cartesian cine were run consecutively at the same image plane.
Results and Discussion
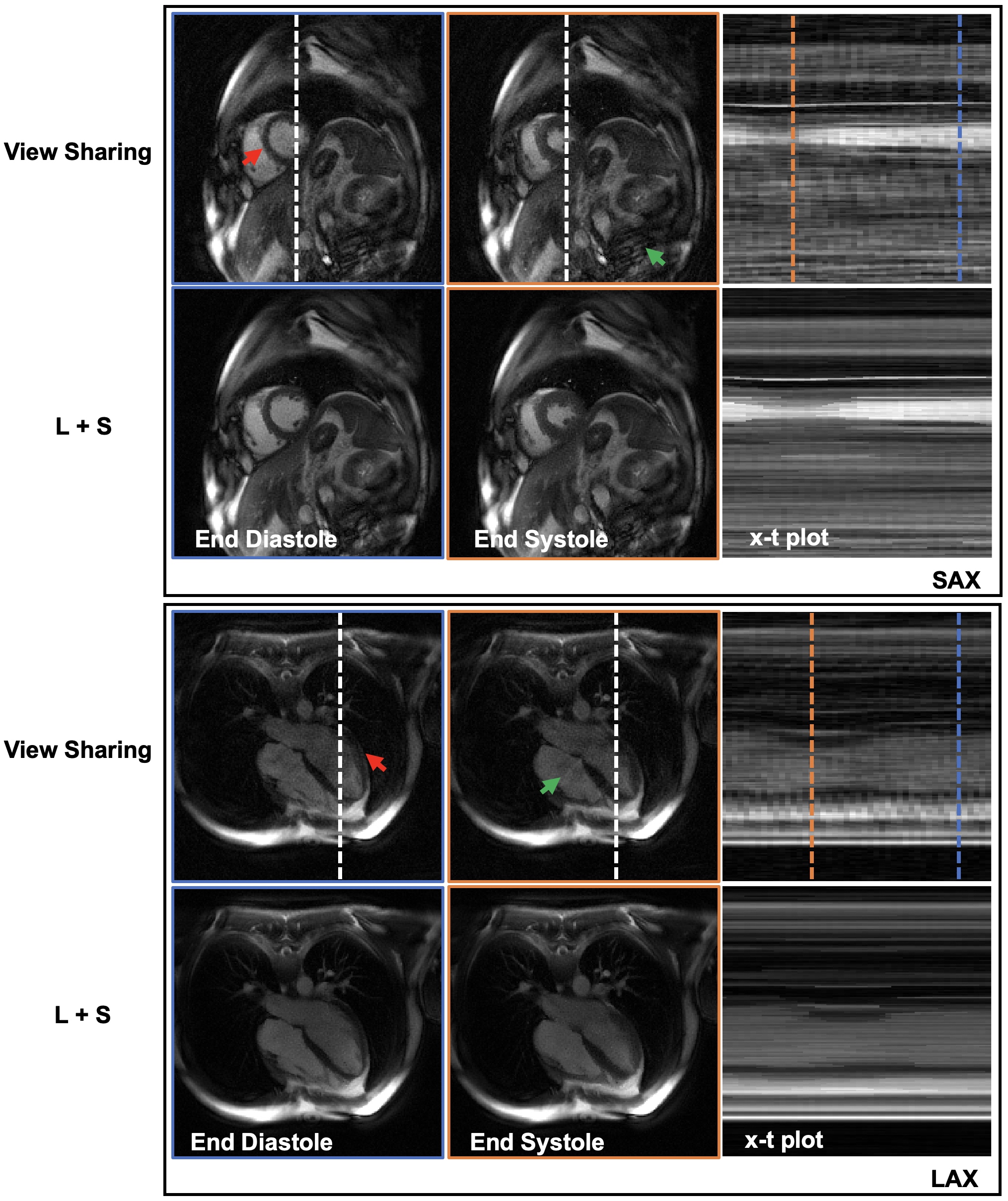
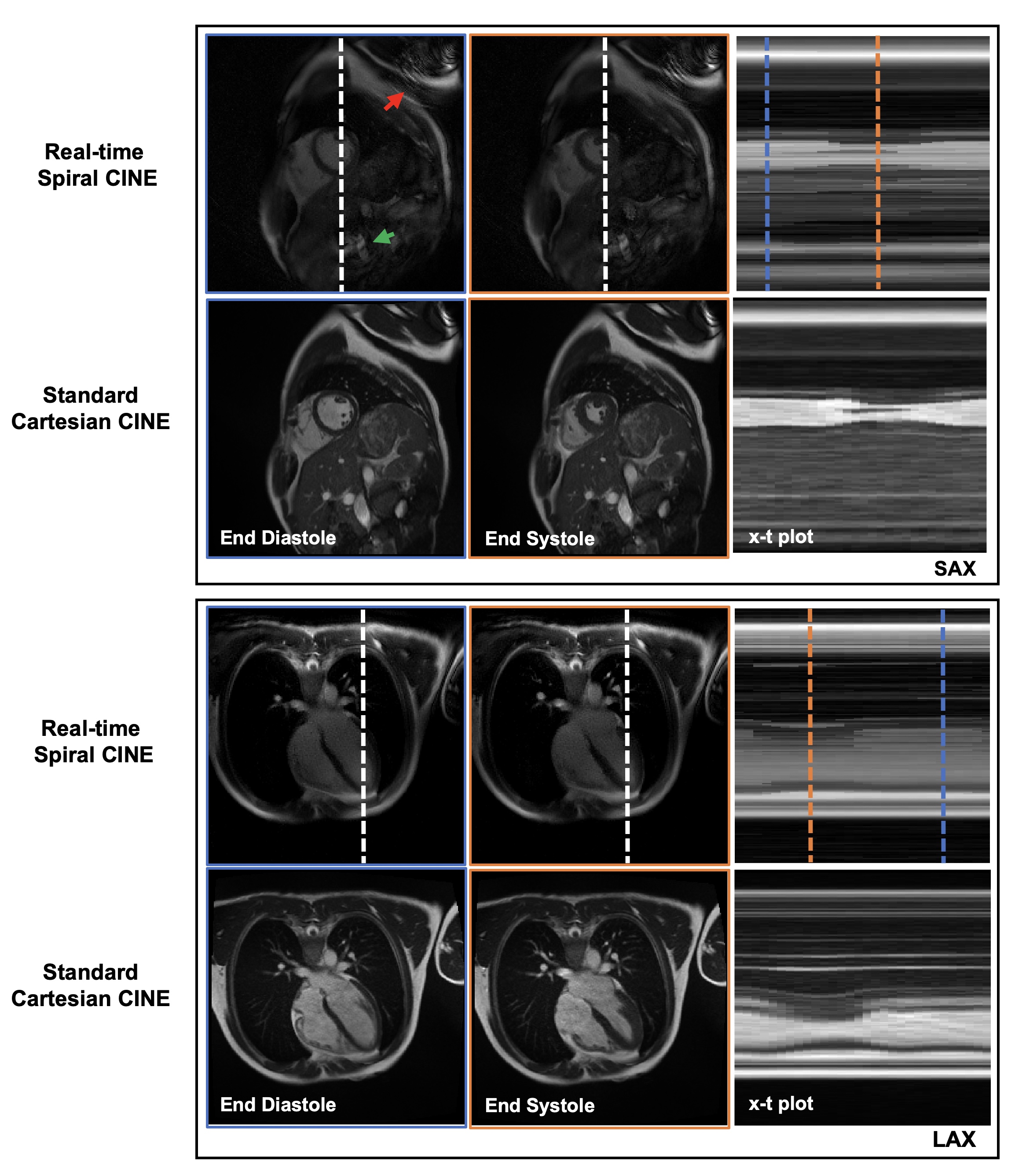
Figure 2 shows systolic and diastolic frames from short-axis and long-axis breath-held experiments using the spiral-in-out bSSFP sequence. Results are shown using view sharing (top row) and L+S reconstruction (bottom row) with the same temporal resolution.The right column shows the temporal profiles across the middle of the left ventricle. The green arrows point to structures with view-sharing that show obvious noise-like aliasing artifacts, while the red arrows point to structures that show temporal blurring. The L+S method performs better in removing aliasing while conserving detailed information with improved image quality. The cardiac movies are shown in Figure 4.Figure 3 shows systolic and diastolic frames from the free-breathing spiral-in-out bSSFP sequence combined with L+S (top row), and from the standard breath-held Cartesian bSSFP cine sequence (bottom row). The x-t plots indicate that the proposed method yields a relatively smooth transition between the end of systole and the end of diastole, when compared with the standard method. As demonstrated in Figure 2 and 3, B0 inhomogeneity-induced artifacts such as banding and blurring were not evident at 0.55T after good cardiac shimming. Lengthening the TR to 6.5ms or more may lead to an increase in pulsatile flow artifacts, especially in slices where the aortic pulsation is strong.
Future work will be focused on visual assessment and quantitative functional measures such as LV ejection fraction in comparison to Cartesian cine.
Conclusion
In this study, a high-resolution real-time spiral-in-out bSSFP cine sequence was developed and tested at 0.55T. By taking advantage of better B0 homogeneity, the results show that the proposed method can recover SNR and achieve diagnostic image quality at low field through high-efficiency spiral sampling and CS-based image reconstruction.Acknowledgements
The authors would like to acknowledge the assistance of Siemens Healthcare in the modification of the MRI system for operation at 0.55T under an existing cooperative research agreement (CRADA) between NHLBI and Siemens Healthcare.References
[1] Carr JC, Simonetti O, Bundy J, Li D, Pereles S, Finn JP. Cine MR angiography of the heart with segmented true fast imaging with steady- state precession. Radiology 2001;219:828–834.
[2] Simonetti OP. Ahmad R. Low-Field Cardiac Magnetic Resonance Imaging: A Compelling Case for Cardiac Magnetic Resonance’s Future. Circulation, Cardiovascular Imaging. 2017;10(6).
[3] Rashid S. Han F. Gao Y. Sung K. Cao M. Yang Y. Hu P. Cardiac Balanced steady-state free precession MRI at 0.35 T: a comparison study with 1.5 T. Quantitative Imaging in Medicine and Surgery. 2017;8(7):627-636.
[4] Campbell-Washburn, A.E. et al, Opportunities in interventional and diagnostic imaging using high-performance low field MRI. Radiology, 2019; 293: 384-393.
[5] Restivo MC, Ramasawmy R, Bandettini WP, Herzka DA, Campbell-Washburn AE. Efficient spiral in-out and EPI balanced steady-state free precession cine imaging using a high-performance 0.55T MRI. Magn Reson Med. 2020;84:2364–2375.
[6] Feng X, Salerno M, Kramer C M, Meyer CH. Non-Cartesian balanced steady-state free precession pulse sequences for real-time cardiac MRI. Magn Reson Med. 2016, 75(4):1546.
[7] Wang Z, Feng X, Dou Q, Meyer CH. Accelerated Spiral imaging for Real-time Cardiac MRI. Proceedings 26th Annual Meeting ISMRM, Paris. 2018:0935.
[8] Otazo R, Candes E, Sodickson DK. Low-rank plus sparse matrix decomposition for accelerated dynamic MRI with separation of background and dynamic components. Magn Reson Med. 2014. 73(3): 1125-1136.
[9] Uecker M, Lai P, Mruphy MJ, et al. ESPIRiT--an eigenvalue approach to autocalibrating parallel MRI: where SENSE meets GRAPPA. Magn Reson Med. 2014. 71(3): 990-1001.
Figures